Beyond Small Molecules
Bacteriophages, Endolysins, Antimicrobial Peptides & Monoclonal Antibodies as Antimicrobial Agents
2026-06-23
Bacteriophages, Endolysins,
Antimicrobial Peptides & Monoclonal Antibodies
Russell E. Lewis, Pharm.D
Associate Professor of Infectious Diseases (MEDS-10/B)

russelledward.lewis@unipd.it
https://github.com/Russlewisbo
Slides and course materials: www.idpadova.com
Learning objectives
By the end of this session, you should be able to:
- Explain the biology of obligately lytic vs. temperate phages and why it dictates therapeutic suitability
- Critically interpret phage susceptibility testing (plaque assay, EoP, phagogram) as a pharmacodynamic surrogate
- Reason through phage PK/PD, immunogenicity, and phage–antibiotic interactions at the bedside
- Appraise the disconnect between compassionate-use case reports and randomized trial data
- Place endolysins, antimicrobial peptides, and monoclonal antibodies within the same “targeted biologic” antimicrobial framework
Why now? The post-antibiotic anxiety
- Infectious disease caused ~1/3 of US deaths in 1900;
the antibiotic “golden era” (1950–70) reversed this - New class discovery has stalled while resistance accelerates
- Bacterial AMR was associated with ~4.95 million deaths (1.27 million attributable) in 2019; projections approach 10 million/year by 2050
- S. aureus sepsis mortality fell from ~85% (pre-antibiotic) to ~23%, but MRSA bacteremia mortality remains high
Four platforms, one logic
| Platform | Nature | Replicates? | Spectrum |
|---|---|---|---|
| Bacteriophages | Lytic virus | Yes (self-amplifying) |
Very narrow (strain) |
| Endolysins | Phage-derived enzyme | No | Narrow–moderate |
| Antimicrobial peptides | Small cationic peptide | No | Broad (often) |
| Monoclonal antibodies | Host-type IgG | No | Very narrow (epitope) |
A Brief History
Discovery: Hankin, Twort, d’Hérelle

- 1896 — Hankin describes antibacterial “substance” in the Ganges/Jumna passing through filters and killing Vibrio cholerae; later analyses doubt phages were the agent
- 1915 — Twort reports “ultramicroscopic” lytic agent
- 1917 — d’Hérelle gives unambiguous evidence of a replicating, bacteria-dependent organism; coins bacteriophage (“to devour bacteria”)
- First plaque assay and first quantification of titer described in the same lineage
Eclipse and survival in the East

- First published therapeutic use ~4 years after d’Hérelle’s discovery; he personally treated many patients
- Penicillin and the antibiotic era eclipsed phage therapy in the West
- Narrow host range, lack of pharma interest, and geopolitics shifted research to chemotherapeutics
- Phage therapy persisted in Eastern Europe and the former Soviet Union (Eliava Institute, Tbilisi) and is still used there
The modern resurgence
- AMR threat has driven renewed interest as a self-amplifying, self-limiting “drug”
- An estimated 10³¹ phage particles on Earth — a near-inexhaustible, biodiverse resource
- High-profile compassionate-use successes (Patterson/Acinetobacter, 2017) catalyzed Western academic programs
- Trajectory now hinges on translational PK/PD research and well-designed clinical trials
The 2017 Schooley/Patterson case at UCSD is the inflection point for US academic phage therapy and led to IPATH. However, enthusiasm currently outstrips controlled evidence.
Phage Biology
Diversity and taxonomy
- Most abundant biological entity on Earth (~10³¹ particles)
- As of 2022, 1653 phage genera recognized by the ICTV
- Only ~6300 phages examined by EM; ~14,200 sequenced — most with dsDNA genomes
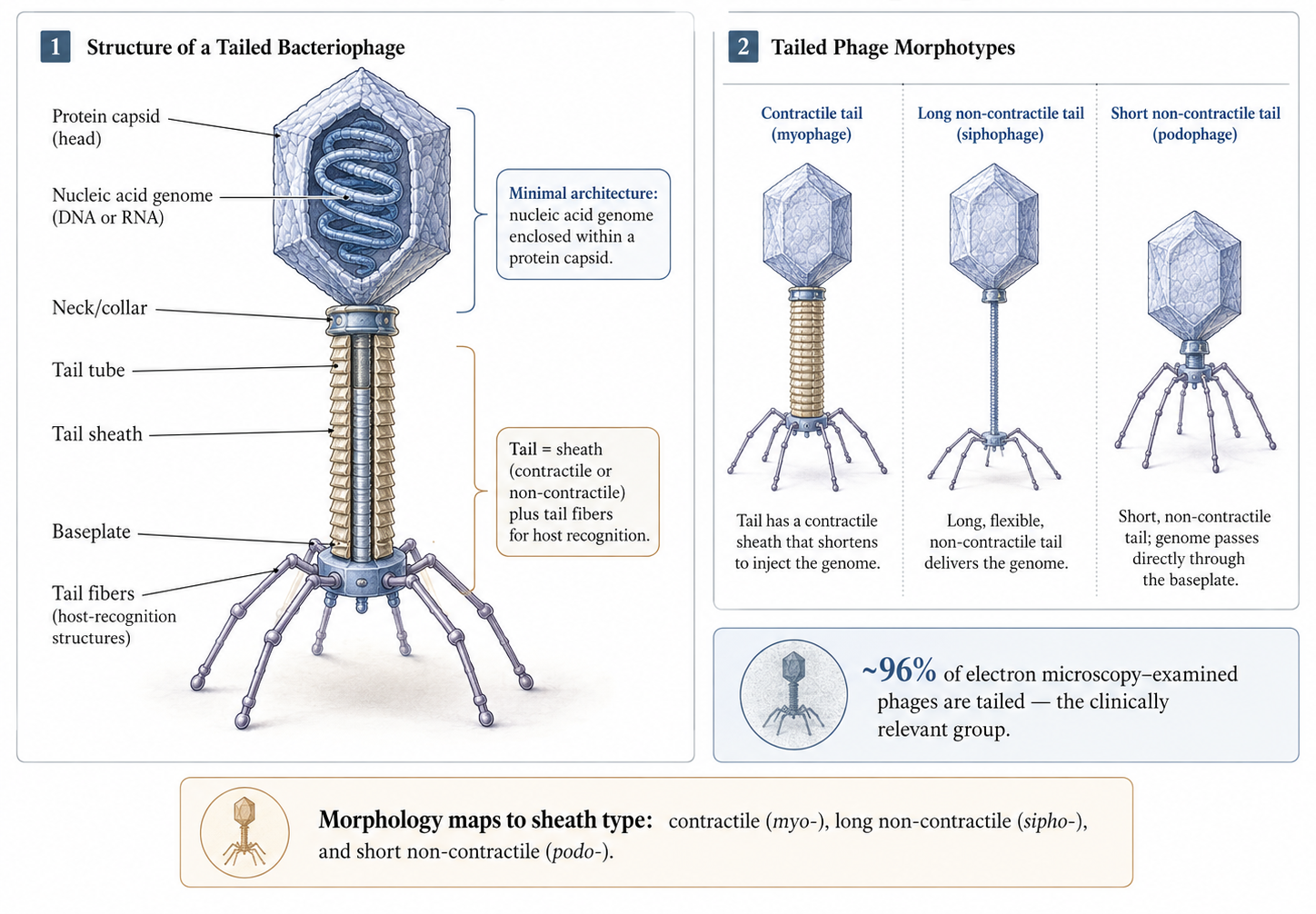
- Classical morphology-based families (Siphoviridae, Myoviridae, Podoviridae) now reorganized; morphology terms persist descriptively
Anatomy of a tailed phage
Lytic vs. lysogenic life cycles
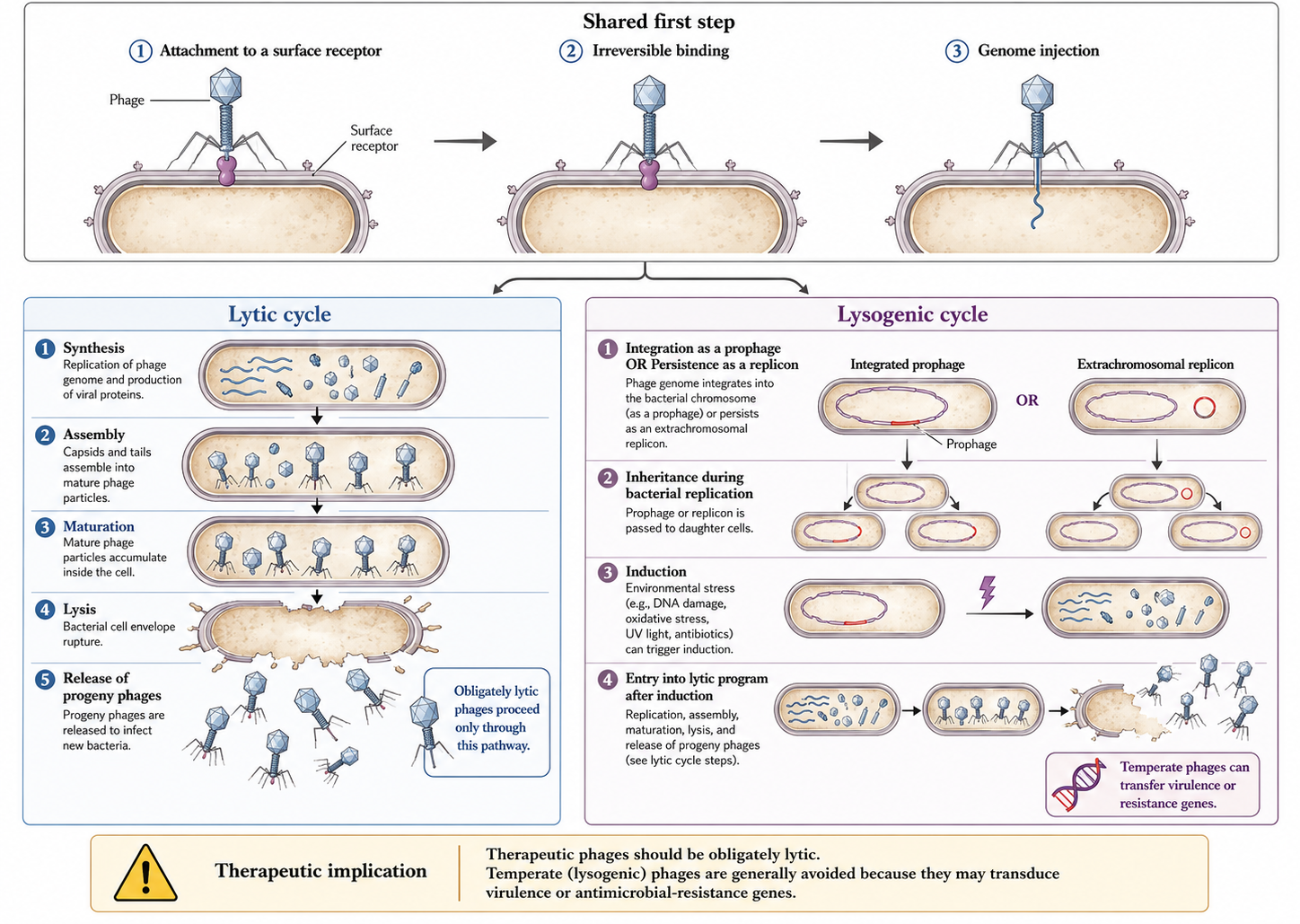
Adsorption: not just Brownian luck
Encounters are largely Brownian/stochastic — phages are non-motile
Reversible binding precedes irreversible binding and injection
Phages can “walk” or “roll” across the surface to find an injection site
Mucus-associated subdiffusive motion (Ig-like capsid domains binding mucin) raises encounter frequency at mucosal surfaces
Spectrum & Susceptibility Testing
Why we must test every isolate
- Narrow host range means no assumed susceptibility — test against each clinical isolate
- Best suited to monomicrobial infection; polymicrobial sites (diabetic foot, intra-abdominal) are harder
- If multiple strains of one species are present, test each strain
- This is the operational bottleneck that makes phage therapy a personalized intervention
The plaque assay and efficiency of plaquing
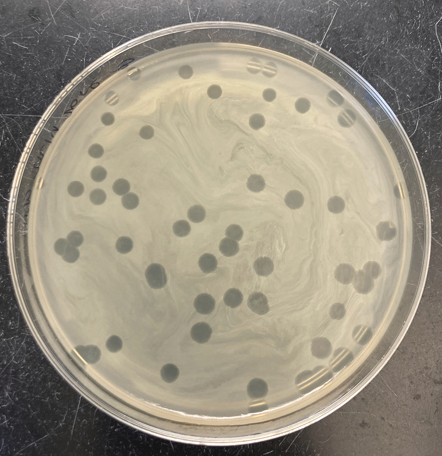
- Lawn of clinical isolate + serial phage titers → zones of clearance (plaques)
- EoP = titer producing plaques on the clinical isolate ÷ titer on the propagation host
- A pharmacodynamic surrogate analogous to MIC; allows ranking of candidate phages
- An EoP ≥ 0.1 appears associated with better outcomes (thresholds still provisional)
Spot tests and phagograms
- Dilutional spot test: spot decreasing titers on a lawn; compare candidate phages in one assay
- Phagogram: co-incubate fixed phage + bacteria, track optical density/respiration vs. growth control over ~24 h
- Time course mirrors broth microdilution kinetics used for antibiotic MICs
- Higher-throughput readouts (e.g., OmniLog respirometry) enable rapid screening
Testing for combinations — before the bedside
- Phage therapy is usually given with antibiotics — confirm no antagonism, ideally synergy
- For biofilm indications, test anti-biofilm activity against the clinical isolate in vitro first
- Combination/cocktail design should be deliberate, not ad hoc
- In vitro testing for synergy/antagonism between selected antibiotics and phages is a recommended step
Bacterial Resistance to Phages
Resistance is the default, not the exception
- ~1025 phage infections per second in the ocean; 20–40% of marine bacteria killed daily
- Enormous selective pressure has produced layered anti-phage defenses
- Spontaneous phage-resistant mutants arise at ~10⁻⁵ (range 10⁻⁹–10⁻²)
- Clinically, the question is not whether resistance emerges but whether it carries a fitness cost we can exploit
Receptor modification — and its trade-off
- Most common mechanism: alteration or loss of the phage-binding receptor
- Receptors are often virulence factors or efflux/porin components, so resistance can shift antibiotic susceptibility too
- Phage-resistant mutants are frequently less virulent
- The most common resistance route may yield bacteria that are easier to treat — a therapeutic silver lining
Abortive infection and CRISPR-Cas
- Abortive infection (Abi): infected cell commits altruistic suicide (DNA/membrane degradation) before progeny mature — kin selection
- CRISPR-Cas: adaptive immunity in ~40% of sequenced bacteria; spacers guide Cas nucleases to phage DNA
- Other layers: restriction-modification, CBASS/cyclic-nucleotide signaling, superinfection exclusion
- Pre-clinical screening of each clinical isolate sidesteps most defenses at the patient level
Mitigating resistance: cocktails and cycling
- Cocktails: combine phages using different receptors to raise the barrier to resistance
- Sequential therapy: rotate phages of differing antigenicity (also mitigates neutralizing antibody)
- Cocktails must be designed for no inter-phage antagonism (receptor competition, CRISPR upregulation)
- “Phage training” — experimental coevolution to pre-adapt phages — delays resistance
Manufacturing, Logistics & Regulation
From sewage to sterile vial

- Discovery sources: wastewater, environmental water, anywhere bacteria are abundant
- For ESKAPE pathogens a matching phage is often found quickly; for rare isolates it may take months or never
- Candidate phages are sequenced and characterized: confirm obligately lytic; exclude toxin/resistance/integrase genes
- Amplified on bacterial hosts to reach therapeutic titers
Timeline to produce bacteriophage therapy
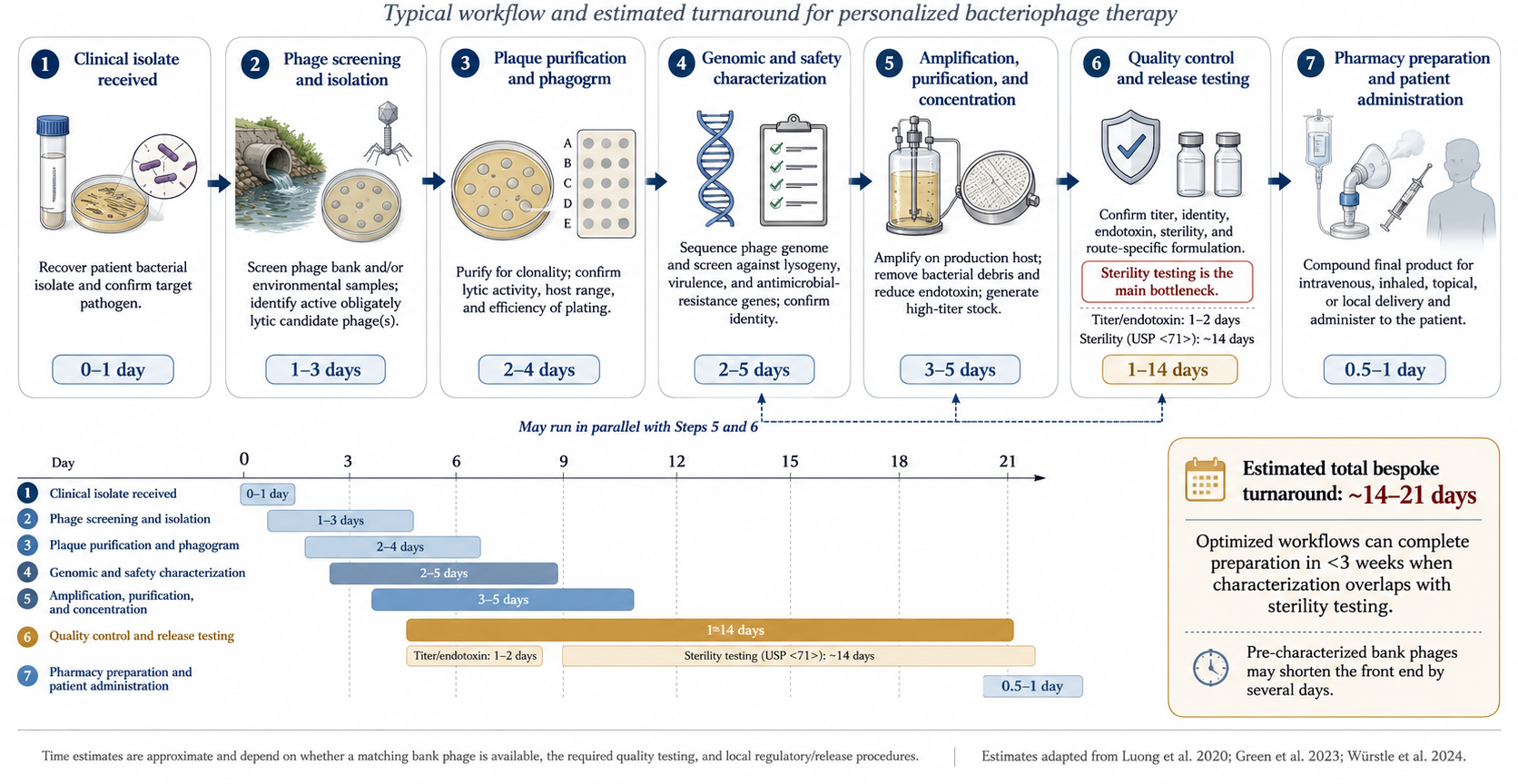
Endotoxin and the contaminant problem
- Bacterial lysis releases endotoxin — FDA limit 5 EU/kg/dose
- Removal: ultrafiltration, affinity and ion-exchange chromatography
- Other risks: prophages, pathogenicity islands, toxins, mobile genetic elements from the propagation host
- Mitigation: amplify on a clean surrogate host (e.g., S. carnosus or S. aureus RN4220) rather than the clinical isolate
Stability, storage, and formulation
Frozen at −80 °C with glycerol cryoprotectant; or 4–6 °C; or lyophilized for ambient storage
Shelf life can be years with proper storage
Diluted for use in Plasma-Lyte, normal saline, or other fluids — compatibility is phage-specific
Always confirm retained activity in the chosen diluent before administration
Regulatory pathway (EU vs. US)
- Phage therapy is not FDA-approved; use is via clinical trial or compassionate use after conventional failure
- No EU-wide authorised human phage medicinal product under EU law.
- Per-case emergency IND (eIND) or expanded-access IND required
- Emergent eIND can be granted rapidly once a phage is identified; non-emergent ~4 weeks
- Europe: magistral preparations (Belgium) and named-patient frameworks offer alternative routes
Pharmacokinetics & Pharmacodynamics
Phages break small-molecule PK rules
- Large, proteinaceous, self-replicating, and interactive with host immunity
- Concentration at the target can increase where bacteria are present (auto-dosing) then fall as bacteria clear
- “Dose” is entangled with bacterial density, burst size, and adsorption rate
- Routes: oral, intravenous, inhaled, and direct application
Oral and the GI gauntlet
- Proposed absorption via transcytosis across epithelial tight junctions — limited by phage size
- Vulnerable to gastric pH <6, mucins, and immune clearance
- Mitigation: co-administer with an alkaline/antacid buffer
- Systemic absorption after oral dosing is inconsistent, though phages are recoverable in blood/urine/tissue
Intravenous: fast in, fast out
Phages detectable in circulation soon after IV dosing, then cleared within 8–12 h by the mononuclear phagocyte system
Distributes to synovium, heart, muscle, marrow, kidney, bladder — dose-dependent
Site concentrations are typically several-fold lower than the input titer
IV most strongly stimulates neutralizing antibody and complement
Direct and inhaled administration
Direct (intra-articular, intravesical, intra-operative, topical) bypasses the MPS → higher local, lower systemic titers
Used for PJI, CIED, osteomyelitis, UTI in case reports
Controlled-release (hydrogels, microencapsulation) under study
Inhaled phages for respiratory infection; lung-specific clearance/barriers still being defined
Dosing: empirical, with rare rationale
- Regimens range from single doses to multiple daily dosing to continuous infusion — mostly empirical
- One rational example: twice-daily IV based on detectable phage DNA up to 12 h post-dose
- Multi-route administration is often combined to overcome single-route barriers
- ARLG Task Force: use the highest safe, tolerated dose with endotoxin below limits; repeat dosing to maximize site levels
ARLG ideal PK/PD properties
A favorable phage product should combine:
High microbial susceptibility (low EoP threshold met)
High local concentration at the site of infection
High adsorption rate (infectivity)
Large burst size (progeny per infected cell)
Short latent period (replication time within the cell)
Immunogenicity
The neutralizing antibody response
- Phages are live viruses → IgM within weeks, followed by IgG
- Neutralizing antibodies can sharply reduce phage titers and correlate with clinical failure (Dedrick et al., 2023)
- Cocktails do not solve this — antibodies form against all component phages, with cross-reactivity
- Not universal: some prolonged courses do not generate neutralizing titers
Route matters for immunogenicity
- IV elicits the most robust humoral response; oral and direct elicit less
- Direct administration → lower neutralizing titers, rising with systemic absorption
- Autoimmune phenomena are theoretical and not described with phage therapy to date
- Sequential therapy with antigenically distinct phages can outpace antibody — but narrow inventories limit cycling
Phage–Antibiotic
& Phage–Phage Interactions
Synergy, antagonism, or neutrality
- Phages + antibiotics can be synergistic, antagonistic, or neutral
- General rule: cell-wall agents → synergy; protein-synthesis inhibitors → potential antagonism
- “PAS” (phage–antibiotic synergy): sub-MIC β-lactams/quinolones can stimulate virulent phage production
- But responses are phage- and antibiotic-specific — general rules are only a starting point
When combinations backfire
- Colistin + LPS-binding phages: colistin destabilizes LPS, the very receptor the phage needs → antagonism
- Burst size, pH, viscosity, and fluid dynamics all modulate interactions
- Scoring systems have been proposed but in vitro testing of the actual pair is essential
- Bottom line: confirm the specific phage–antibiotic combination empirically before use
Phage–phage interactions in cocktails
- Phages can interfere with one another — reduced activity of each
- Drivers: competition for shared receptors and CRISPR-Cas upregulation
- Interactions are unpredictable → evaluate combinations individually
- Argues for precision-designed cocktails over ad hoc mixtures
Safety
A reassuring overall profile
- Generally favorable safety across preclinical, case-report, and phase I/II data
- FDA has granted GRAS status for certain phage applications
- Phages are part of the human gut virome — ubiquitous baseline exposure
- ARLG nonetheless recommends interval monitoring of renal/liver function and CBC during therapy
Mechanisms of adverse events
- Endotoxin/bacterial debris release from rapid lysis → proinflammatory cytokine response
- Contaminants: bacterial DNA, enterotoxins, exotoxins, lipoteichoic acid → hypersensitivity/cytokine release
- Manufacturing residues: cesium chloride, polyethylene glycol
- Net effect on the microbiome is narrow vs. antibiotics but understudied
Adverse events in practice
- Preclinical: generally well tolerated; occasional cytokine (IL-1β/IL-6) or IgG/IgM rises without clinical change
- Case reports: mostly none or transient — transient hypotension, fevers/chills, wheeze, flushing, nausea
- Self-limited IL-6/IL-8 cytokine storm resolving in ~1 day reported
- Transient transaminitis with IV/intra-articular dosing; reversible, outcomes still favorable
MDR Infections & Phage Steering
Phages against drug-resistant bacteria
- Resistance to antibiotics does not confer resistance to phages — different targets (surface receptors)
- Most case reports use phages with antibiotics, not as monotherapy
- Narrower microbiome impact than broad-spectrum antibiotics — less collateral resistance selection
- Efficacy in MDR infection will only be settled by prospective trials
Phage steering: weaponizing the trade-off
- Phage steering drives bacteria toward a more susceptible phenotype (Gurney et al., 2020)
- P. aeruginosa: selection for phage resistance via efflux/porin restores antibiotic susceptibility (Chan et al., 2016)
- Can even re-sensitize to drugs not normally used (e.g., tetracyclines for Pseudomonas) (Gurney et al., 2020)
- Klebsiella and Acinetobacter: phage resistance entails loss of capsule/MDR and re-sensitization (Gordillo Altamirano et al., 2021; Majkowska-Skrobek et al., 2021)
Biofilm Infections
Why phages suit biofilms
- Most bacteria live in sessile biofilm states, not planktonic (Doub, 2020)
- Phages encode depolymerases and endolysins that degrade the extracellular polymeric matrix (Chan and Abedon, 2015)
- Confined biofilm environment can increase chance phage–bacteria encounters (Doub, 2020)
- Can infect metabolically reduced cells, degrading biofilm piecemeal (Chan and Abedon, 2015)
Delivery determines biofilm success
- Direct administration reduces biofilm; systemic administration often does not reach device biofilm
- Murine PJI: IP phage + vancomycin synergized against planktonic bacteria but not the implant biofilm
- Phages are non-motile → maximize chance encounters by delivering directly to the biofilm
- Clinical case series support phages as a powerful adjuvant in recalcitrant biofilm infection
Clinical Trials: The Reality Check
Case reports vs. controlled trials
- Numerous case reports show promise across syndromes and pathogens
- M. abscessus: favorable response in 11/20 compassionate-use patients
- Since 2000, 13 English-language trials; 6 assessed efficacy
- Controlled trials have not reproduced the dramatic case-report outcomes
Early efficacy signals
- Wright 2009 (chronic P. aeruginosa otitis): single 6-phage cocktail, PST-confirmed → improved clinical scores and lower P. aeruginosa counts vs. placebo
- The first modern randomized, double-blind, placebo-controlled phage trial
- Small (n≈24) and single-center, but a genuine positive efficacy signal
The instructive failures
- Rose 2014 (burn wounds): fixed (non-personalized) cocktail, no prospective PST; no bacterial-load difference; spray ran off the wound
- Sarker 2016 (pediatric E. coli diarrhea, Bangladesh): oral T4-like coliphages, no PST; no clinical efficacy, no intestinal amplification
- Recurring culprits: fixed cocktails, no susceptibility testing, inadequate coverage, delivery failure
PhagoBurn and the delivery problem
Jault 2019 (PhagoBurn): RCT of a P. aeruginosa phage cocktail vs. standard care in burn wounds
Phages slower to reduce bacterial burden than standard-of-care antiseptic
Manufacturing reduced titer over storage → under-dosing; some isolates resistant at low residual titer
A landmark in showing how CMC/manufacturing can sink a phage trial
Intravesical phages and the honest null
Leitner 2021: intravesical phages vs. antibiotics vs. placebo for UTI before TURP
Phages were not superior to placebo and not non-inferior to antibiotics
Well-designed, multi-arm, double-blind — a rigorous neutral result
Reinforces that adjunctive, personalized, well-delivered phages remain the most defensible use today
Selected phage clinical trials
| Study (year) | Indication | Design | Efficacy signal |
|---|---|---|---|
| Wright (2009) | Chronic P. aeruginosa otitis | RCT, DB, PC | Positive |
| Rose (2014) | Burn wound colonization | Self-controlled | Null |
| Sarker (2016) | Pediatric diarrhea | RCT, PC | Null |
| Jault / PhagoBurn (2019) | Burn wound P. aeruginosa | RCT | Inferior (under-dosed) |
| Leitner (2021) | UTI pre-TURP | RCT, DB, 3-arm | Null |
Endolysins
Enzybiotics: lysis from the outside
- Phage-derived enzymes that hydrolyze peptidoglycan → osmotic lysis
- Three classes: glycosidases, amidases, endopeptidases
- Gram-positive endolysins: N-terminal catalytic domain + C-terminal cell-wall-binding domain
- Gram-negative endolysins: globular, no discrete binding domain
The Gram-negative barrier
- Exogenous endolysins reach peptidoglycan readily in Gram-positives (thick, exposed PG)
- Gram-negative outer membrane blocks access to PG
- Workarounds: EDTA/weak acids to permeabilize, or engineered “Artilysins” fusing endolysin to a membrane-translocating peptide
- Receptor-binding-protein fusions can enable Gram-negative killing
Resistance, PK, and immunogenicity
- Resistance less likely than to phages — peptidoglycan bonds are highly conserved and hard to alter
- More conventional PK than phages (a defined protein, not a replicating particle)
- Can still elicit anti-protein antibodies, but routine exposure tempers immunogenicity
- Broader host range than phages, but narrower than most antibiotics
Endolysins in the clinic
- SAL200 (staphylococcal, IV up to 10 mg/kg): phase I — only mild fatigue/myalgia
- Staphefekt (topical): improved symptoms in atopic dermatitis (placebo-controlled)
- Exebacase (CF-301): synergy with anti-staphylococcal antibiotics in vitro
- Exebacase phase III for S. aureus bacteremia/endocarditis stopped for futility at interim
Antimicrobial Peptides
AMPs: ancient innate effectors
- Small (<100 aa), usually cationic, amphipathic (hydrophobic + hydrophilic domains)
- Primary action: cytoplasmic membrane disruption; also inhibit nucleic-acid/protein/cell-wall synthesis
- Broad spectrum and immunomodulatory properties
- Phage-encoded AMPs: lytic factors (non-enzymatic) and tail-complex proteins
Promise vs. the historical wall
Attractive for biofilm and MDR infection; some can cross the Gram-negative OM (Mirski et al., 2019)
Historically limited by toxicity, poor PK, and weak in vivo activity (Deslouches et al., 2020)
Engineered peptides (eCAPs) that mimic endogenous AMPs are an emerging fix (Deslouches et al., 2020)
PLG0206: engineered AMP, phase I IV single-dose — linear PK, well tolerated; phase II in acute PJI (Huang et al., 2022)
Three platforms compared
| Feature | Phages | Endolysins | AMPs |
|---|---|---|---|
| Self-replicating | Yes | No | No |
| Spectrum | Strain-narrow | Narrow–moderate | Often broad |
| Gram-negative use | Yes | Hard (needs engineering) | Some natively |
| Resistance barrier | Low–moderate | High | Variable |
| PK predictability | Low | Higher | Variable |
Monoclonal Antibodies as Antimicrobials
From serum therapy to monoclonals
Antibody-based anti-infectives predate antibiotics: serum therapy for diphtheria/pneumococcus (1890s–1930s)
Displaced by antibiotics, now revived for the same reason as phages — AMR and unmet niches
A monoclonal antibody (mAb) is a defined, host-type IgG targeting a single epitope
Like phages: a narrow-spectrum, manufactured biologic — but it recruits host immunity rather than lysing directly
Mechanisms of anti-infective mAbs
- Toxin neutralization — bind and inactivate a toxin (no direct bactericidal effect)
- Neutralization of attachment/entry — block a viral or bacterial receptor interaction
- Opsonophagocytosis & ADCC — Fc-mediated recruitment of phagocytes/NK cells
- Complement activation (CDC) — classical pathway via Fc
Immunologic rationale and engineering
- Format evolution: murine → chimeric → humanized → fully human to cut immunogenicity
- Fc engineering tunes effector function (ADCC/CDC) up or down
- Half-life extension (e.g., YTE mutations) enables single-dose, season-long prophylaxis (nirsevimab)
- Specificity is the double-edged sword: exquisite targeting, but no breadth and vulnerability to antigenic change
Bezlotoxumab — anti-toxin, not antibacterial
- Human mAb against C. difficile toxin B; does not kill the organism
- MODIFY I/II (adjunct to standard antibiotics): recurrent CDI reduced ~17% vs. ~28% with placebo
- FDA-approved 2016 for prevention of CDI recurrence in high-risk adults
- Caveat: heart-failure exacerbation signal in patients with CHF
Ibalizumab — a mAb as antiretroviral
Humanized mAb binding CD4 domain 2; blocks HIV-1 entry post-attachment (a post-attachment inhibitor)
First-in-class, FDA-approved 2018 for multidrug-resistant HIV-1, IV every 2 weeks
TMB-301: ≥1 log₁₀ viral-load drop in 83% at day 7; ~43% achieved <50 copies/mL by week 25
Does not share resistance pathways with small-molecule antiretrovirals
Anti-anthrax mAbs — neutralizing protective antigen
- Both target protective antigen (PA) to block anthrax toxin assembly/entry (Migone et al., 2009)
- Raxibacumab — FDA-approved 2012 for inhalational anthrax (treatment + prophylaxis) (Migone et al., 2009)
- Obiltoxaximab — FDA-approved 2016, same indication (Greig, 2016)
- Approved via the FDA Animal Rule (efficacy from animal models; human safety only)
RSV — palivizumab to nirsevimab
- Palivizumab: anti-RSV F protein; IMpact-RSV cut hospitalization ~55% in high-risk infants; monthly dosing (The IMpact-RSV Study Group, 1998)
- Nirsevimab: YTE half-life-extended anti-F mAb; single dose per season (Hammitt et al., 2022)
- MELODY: ~75% reduction in medically attended RSV LRTI (Hammitt et al., 2022)
- HARMONIE: ~83% reduction in RSV hospitalization in a pragmatic European trial (Drysdale et al., 2023)
Anti-SARS-CoV-2 mAbs — the escape lesson
- Sotrovimab (COMET-ICE): ~79% reduction in hospitalization/death in early high-risk COVID-19
- Casirivimab/imdevimab, bamlanivimab, tixagevimab/cilgavimab also deployed
- Authorizations withdrawn as Omicron sublineages escaped neutralization
- The defining cautionary tale: monoclonal specificity collapses against a rapidly evolving target
The antibacterial mAb graveyard
Suvratoxumab (anti-S. aureus α-toxin), SAATELLITE: lower VAP incidence numerically but did not meet its primary endpoint
Gremubamab / MEDI3902 (bispecific anti-P. aeruginosa PcrV + Psl), EVADE: did not reduce P. aeruginosa pneumonia
Despite strong preclinical data, no antibacterial mAb is FDA-approved for treating bacterial infection
Successes remain toxin neutralization (bezlotoxumab) and prophylaxis
Why antibacterial mAbs keep failing
- Redundancy: bacteria deploy many virulence factors — neutralizing one is rarely enough
- Single-epitope fragility: antigenic variation defeats narrow targeting (cf. COVID escape)
- Timing & access: mAbs work best as prophylaxis, less as rescue in established sepsis/biofilm
- No self-amplification: unlike phages, a fixed dose cannot “follow” the bacterial burden
Synthesis & Future
Phages vs. mAbs: two targeted biologics
| Dimension | Bacteriophages | Monoclonal antibodies |
|---|---|---|
| Mechanism | Direct lysis + amplification | Neutralization / Fc effector |
| Self-amplifying | Yes | No |
| Spectrum | Strain-level | Epitope-level |
| Main use today | Established MDR/biofilm (adjuvant) | Prophylaxis / toxin neutralization |
| Resistance/escape | Receptor change | Antigenic variation |
| Manufacturing/regulatory | Immature, personalized | Mature, standardized |
Where the field is heading
- Engineered phages: tail-fiber swapping to broaden host range; synthetic/CRISPR-armed phages (Yehl et al., 2019)
- Phage steering & PAS integrated into rational antibiotic-sparing regimens (Gu Liu et al., 2020; Gurney et al., 2020)
- Standardized PK/PD and susceptibility methods; adaptive, personalized trial designs (Suh et al., 2022)
- Biologic combinations: phages + endolysins + antibiotics; mAb cocktails to counter escape (Pirnay, 2020)
Take-home messages
- Use obligately lytic, susceptibility-confirmed phages; screen every isolate
- Phage PK/PD is non-classical — self-amplification, MPS clearance, neutralizing antibody, route-dependent delivery
- Case reports outrun controlled evidence; design failures (no PST, fixed cocktails, under-dosing) explain most negative trials
- Endolysins, AMPs, and mAbs complete a spectrum of targeted biologics — mAbs win at prophylaxis/toxin neutralization, phages at established MDR/biofilm infection