Penicillin and Antibiotic Allergies
Prof. Russell E. Lewis
Department of Molecular Medicine
University of Padua
 |
russelledward.lewis@unipd.it
https://github.com/Russlewisbo
Slides and course materials: www.padovaid.com
On target vs. off-target drug effects
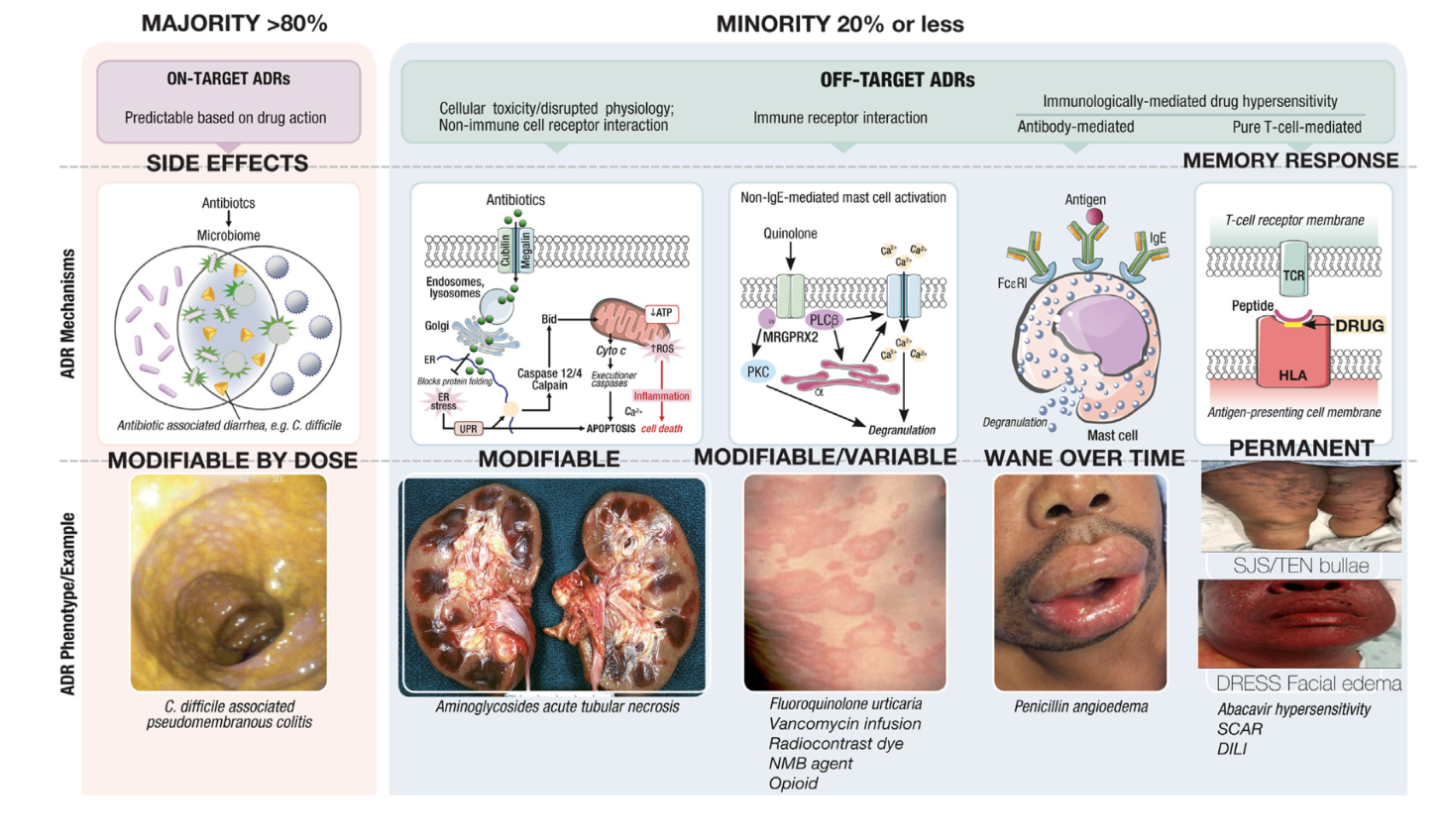
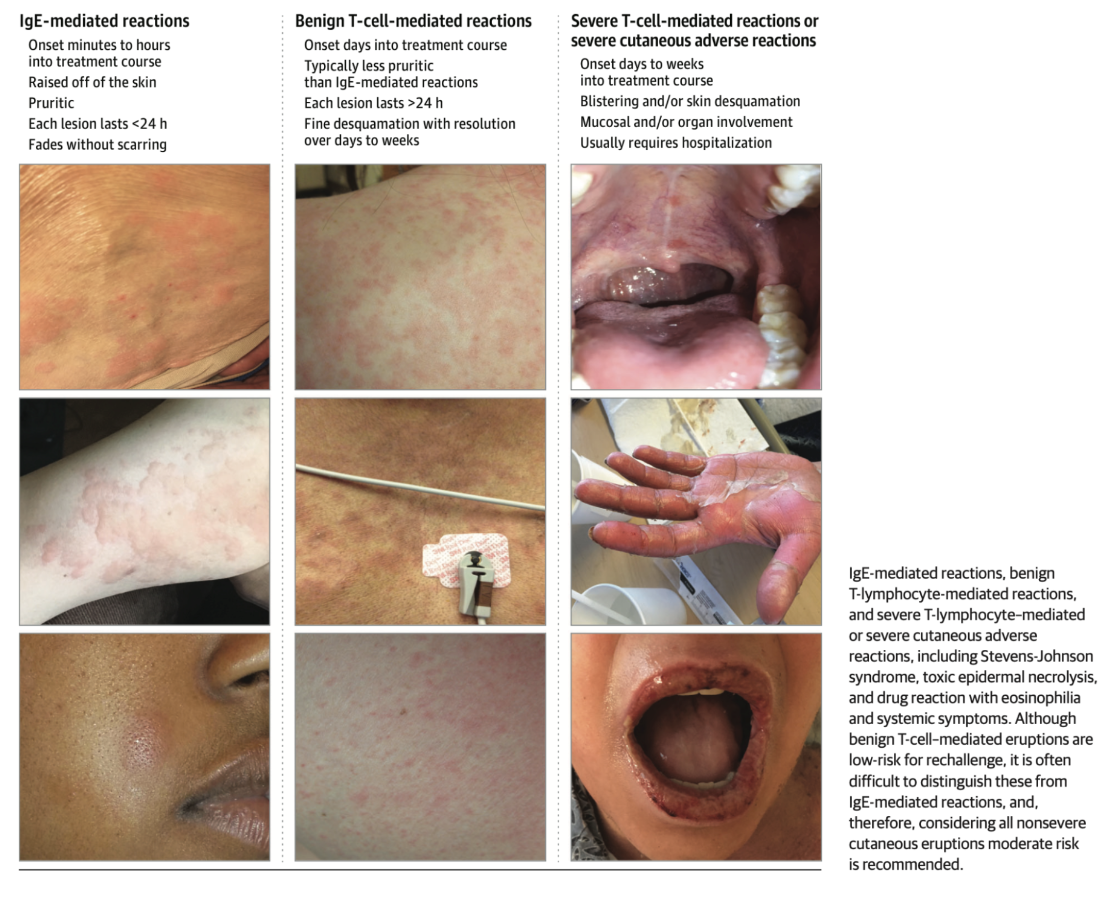
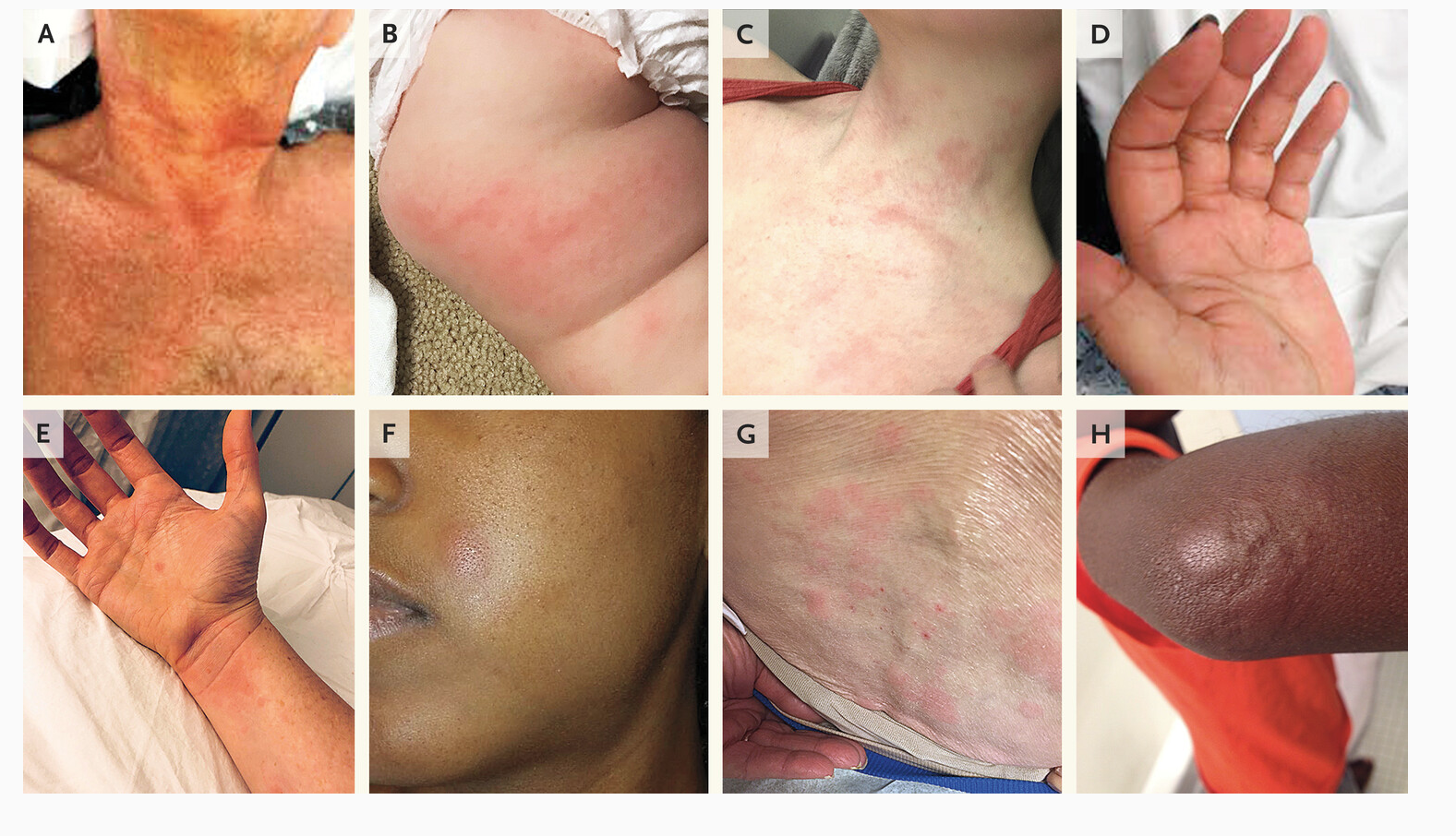
Variable cutaneous presentation of
allergic drug reactions




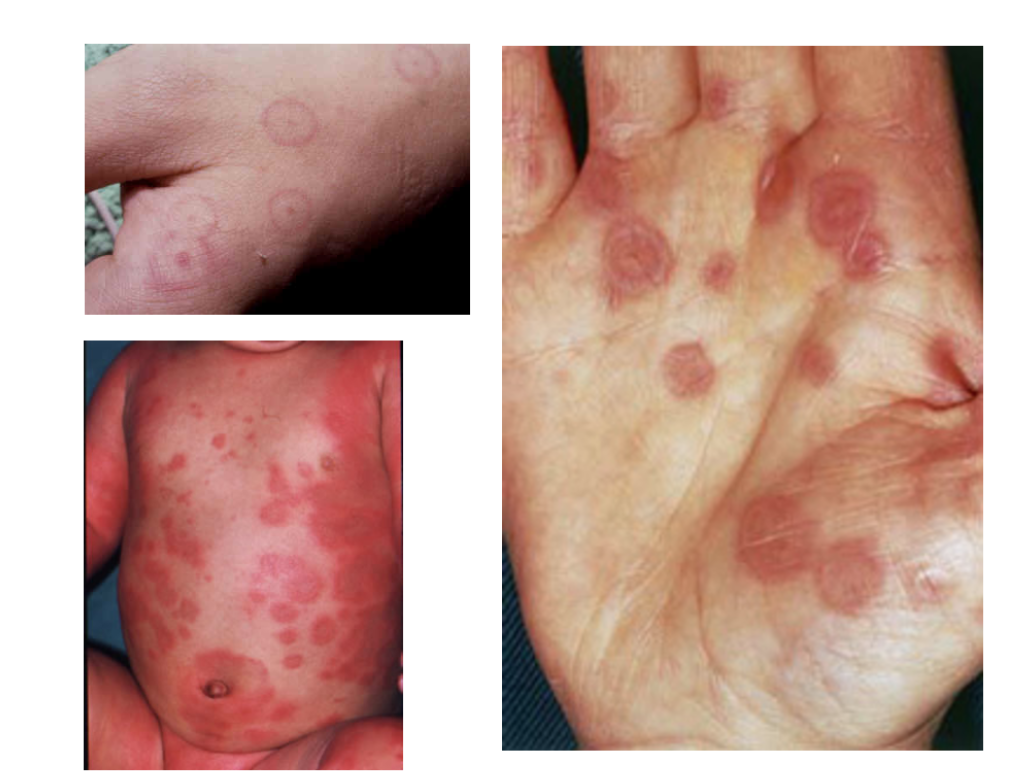
Urticaria and angioedema


Fixed drug eruption

Erythema multiforme,
Toxic epidermal necrolysis (TEN)
DRESS: Drug rash with eosinophilia
and systemic symptoms
Latency: 2-8 weeks
Non-specific symptoms:
- Fever (75%), lymphadenopathy (55-65%)
Hematological abnormalities:
Eosinophilia > 700 mcL (85-95%)
Leukocytosis (95%), neutrophilia (78%), monocytosis (69%)
Atypical lymphocytosis (35-67%)
Visceral involvement:
Liver (53-90%)-cholestatic and/or hepatocellular
Pulmonary (30%)-shortness of breath, cough
Cardiac involvement (2-20%)- hypotension, tachycardia, dyspnea, LV dysfunction, myocarditis

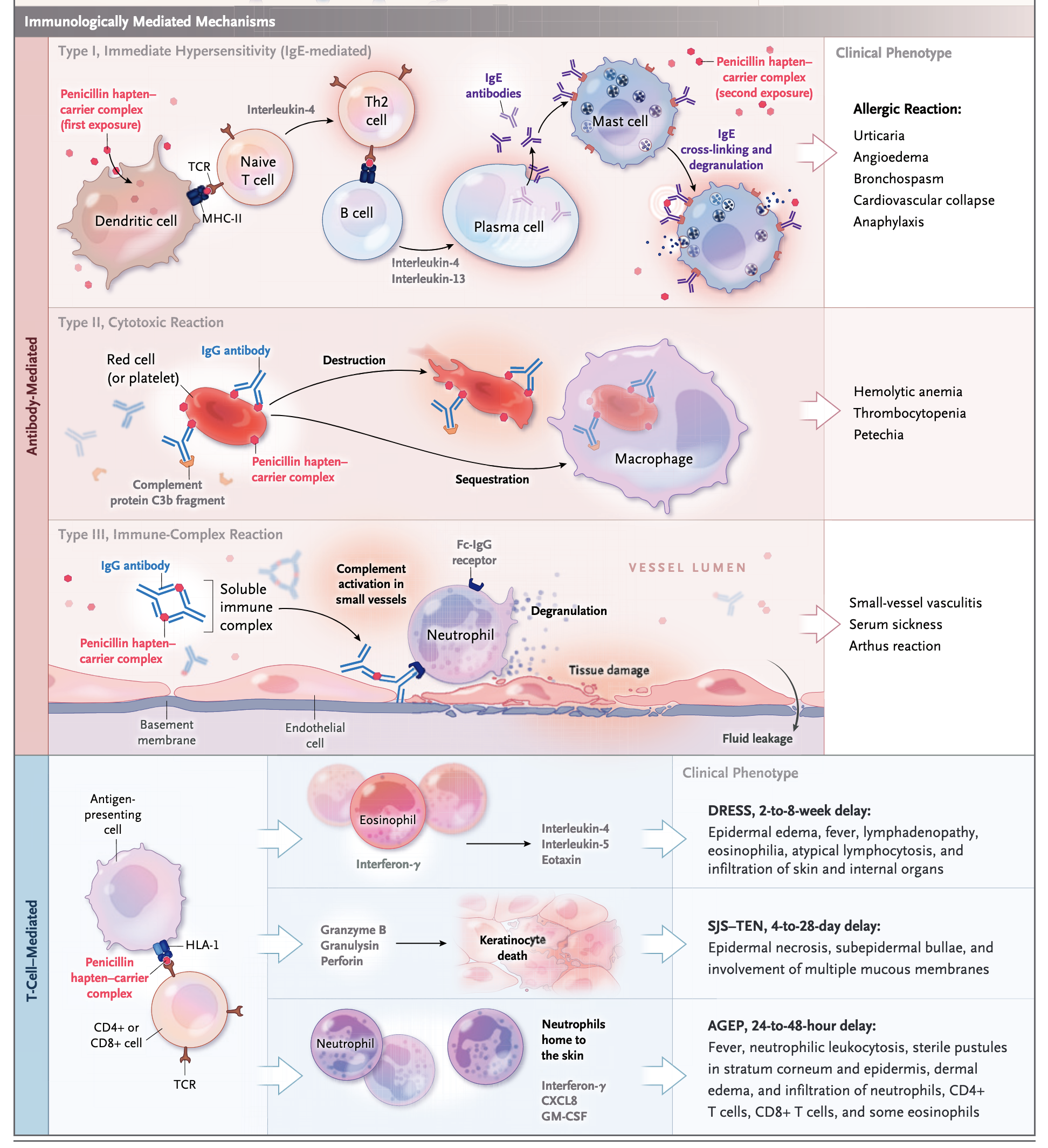
DRESS: Pathophysiology
and systemic symptoms
Pathophysiology:
Type IV T-cell activation (CD4+/CD8+) producing TNF-α
Reactivation of viruses from the Herpesviridae family (eg, HHV-6, HHV-7, Epstein-Barr virus [EBV], cytomegalovirus [CMV]) occurs in up to 75 percent of patients-cause or consequence?
Some patient human leukocyte antigens are associated with higher risk
RegiSCAR scoring system is a commonly used tool for diagnosis
Symptoms may worsen or recur despite drug discontinuation or persisnt, requing immunosuppressive treatment
Stevens-Johnson Syndrome
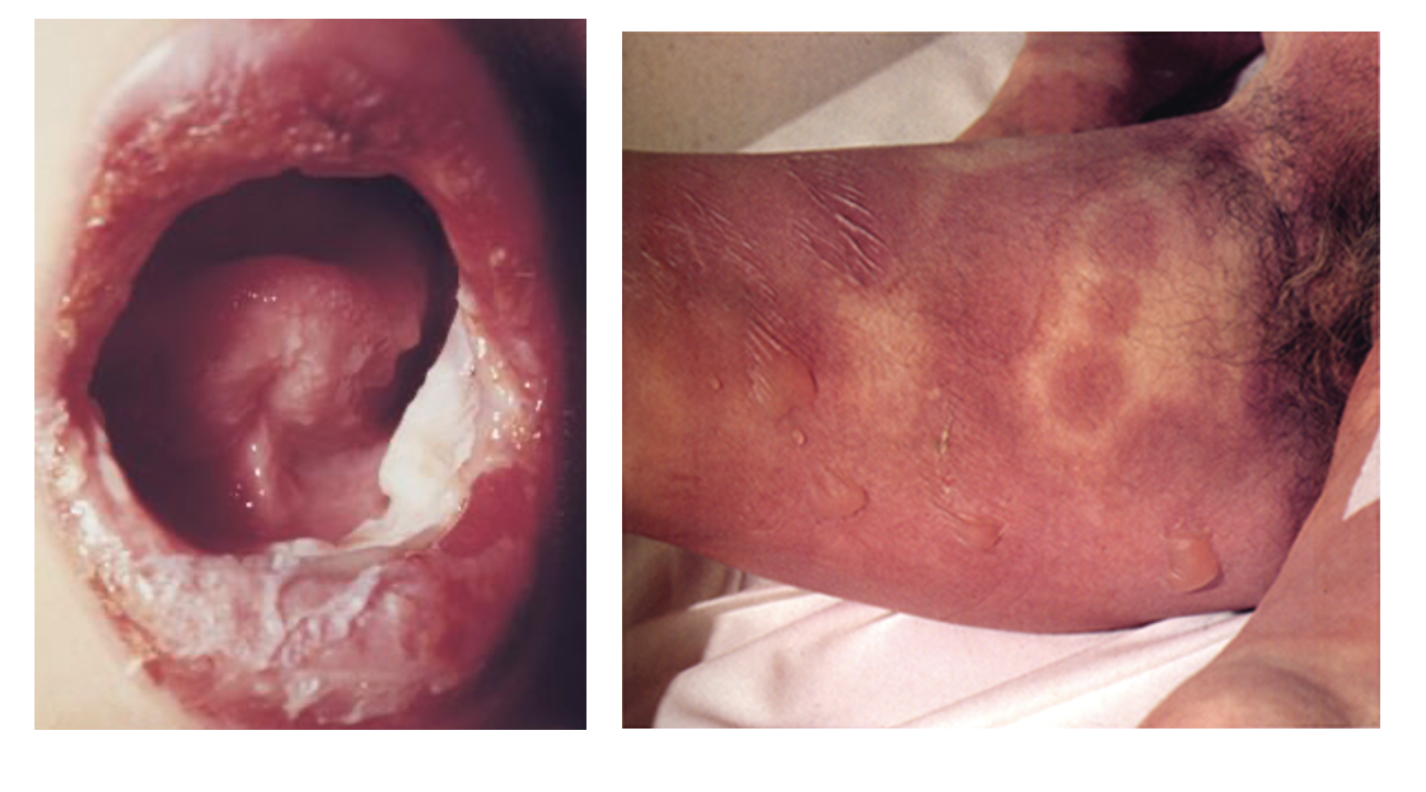
Drug-sensitized cytotoxic CD8+ T cells mediate keratinocyte necrosis
TEN has a mortality rate of approximately 30% that can exceed 50% in elderly or immunosuppressed patients
The severity-of-illness score for TEN (SCORTEN) algorithm facilitates clinical diagnosis and prognostication
SJS is associated with the maintenance of long-lasting tissue-resident memory T-cell responses in the skin that persist after SCAR, necessitating accurate identification and lifelong avoidance of the culprit antibiotic
Acute generalized exanthematous pustulosis (AGEP)
AGEP is a drug eruption characterized by an extensive sterile, nonfollicular pustular reaction superimposed on erythematous plaques, with a prominent leukocytosis and neutrophilic dominance
Most cases of antimicrobial-induced AGEP, such as that caused by β-lactams and quinolones, typically cause symptoms within a day of exposure, whereas other drugs take 7 to 14 days of exposure before symptoms.


Modified Gell and Coombs Classification
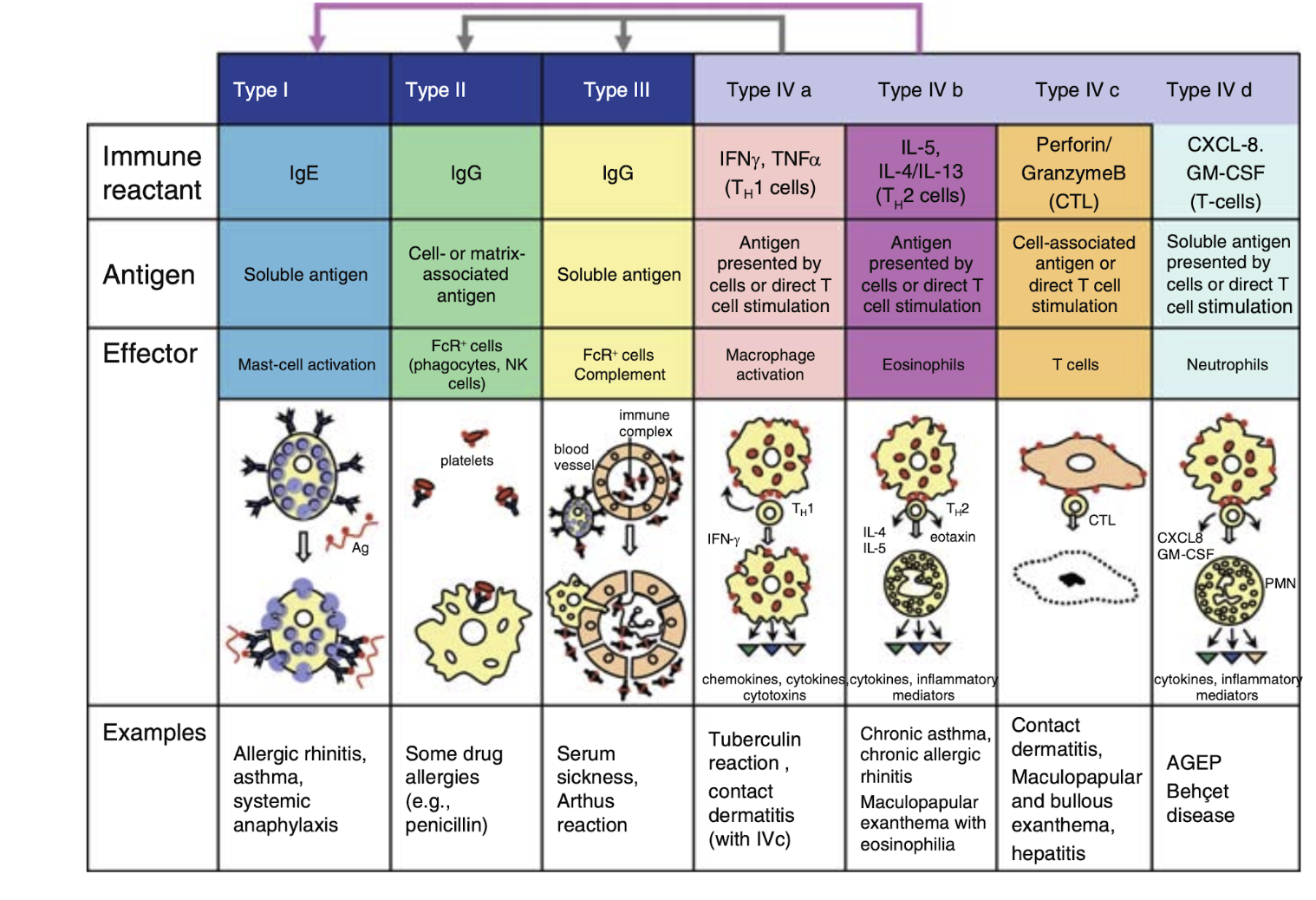
Immunological mechanisms
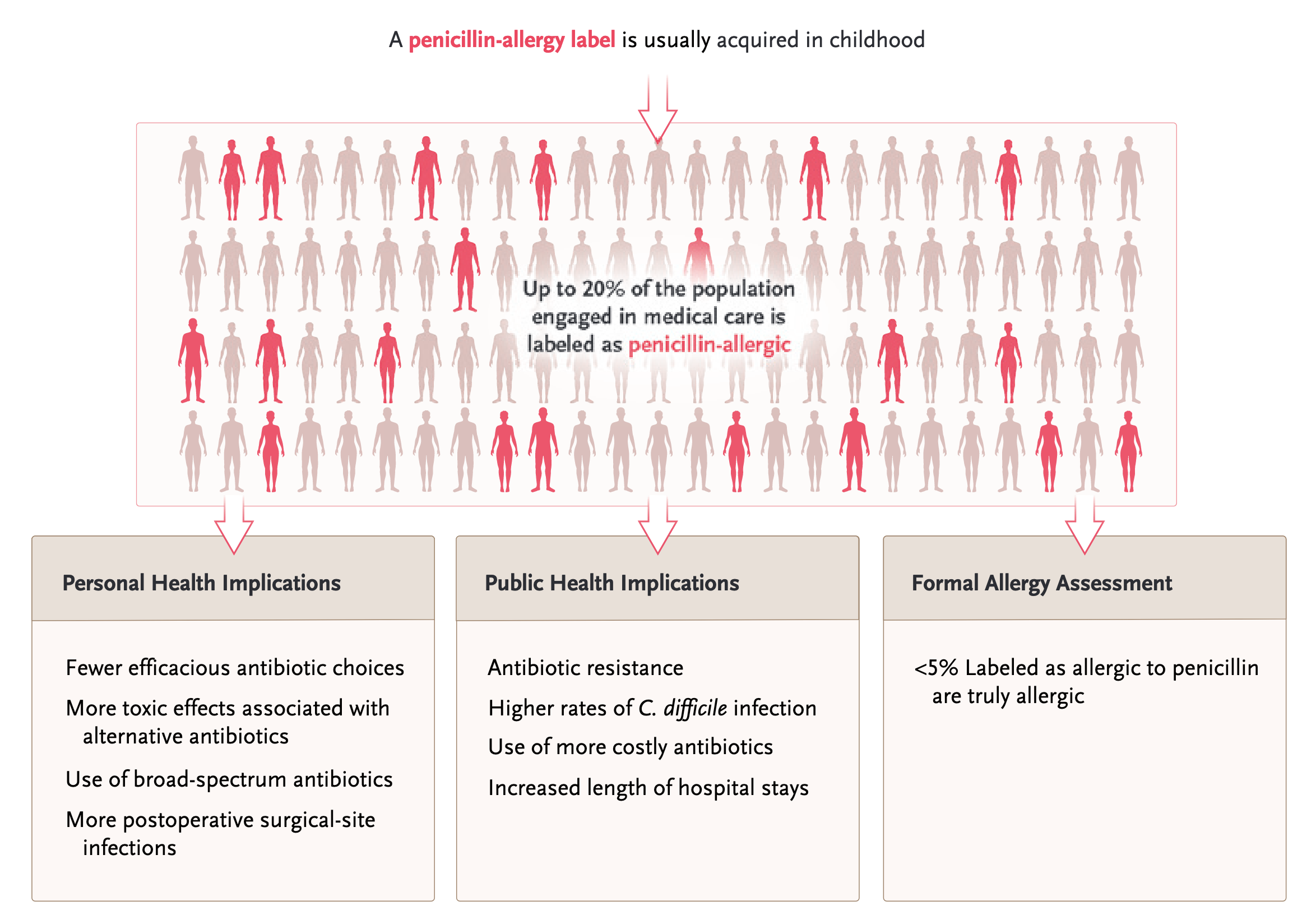
Public health implications
Penicillin allergy history
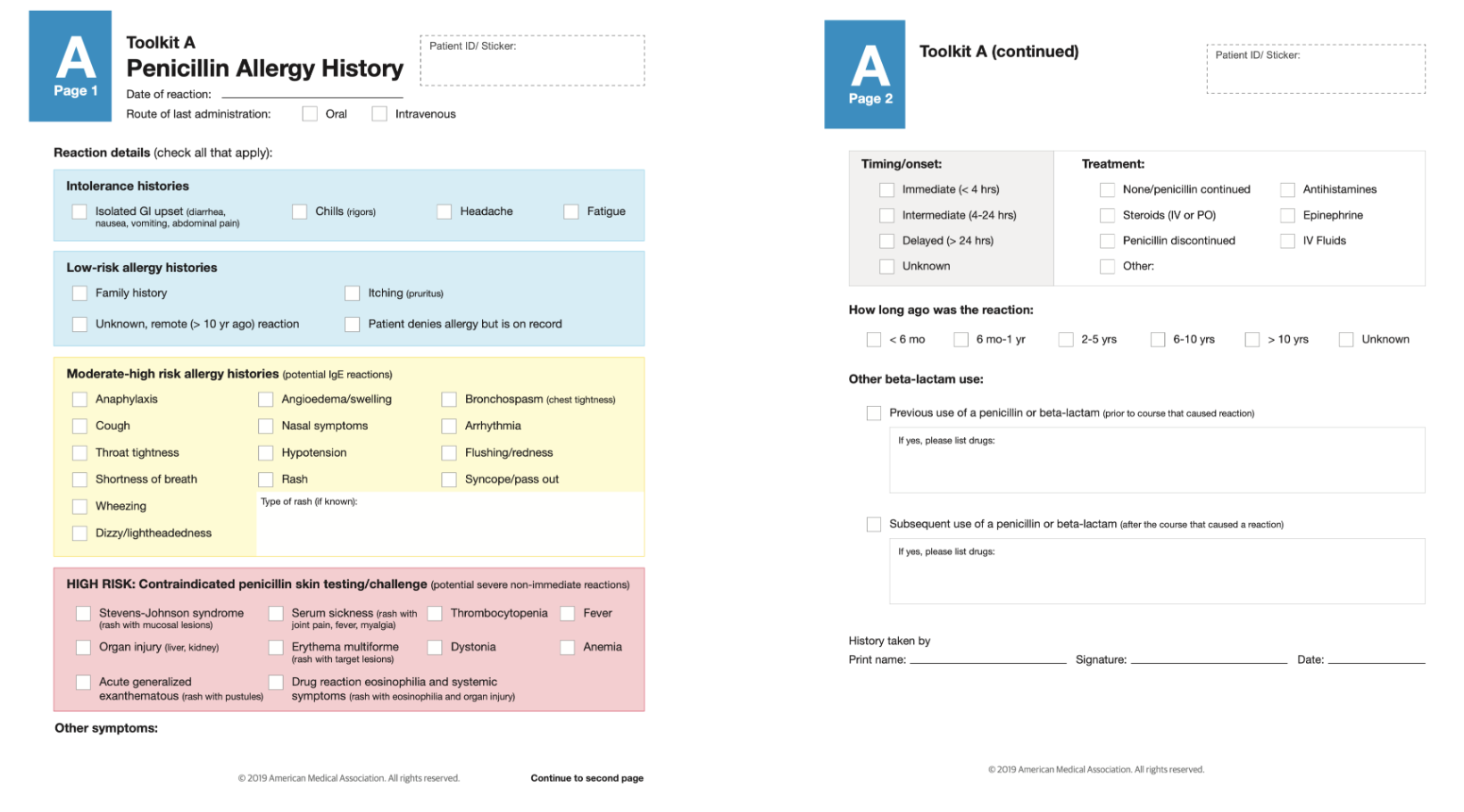
Timing and clinical presentation of reaction
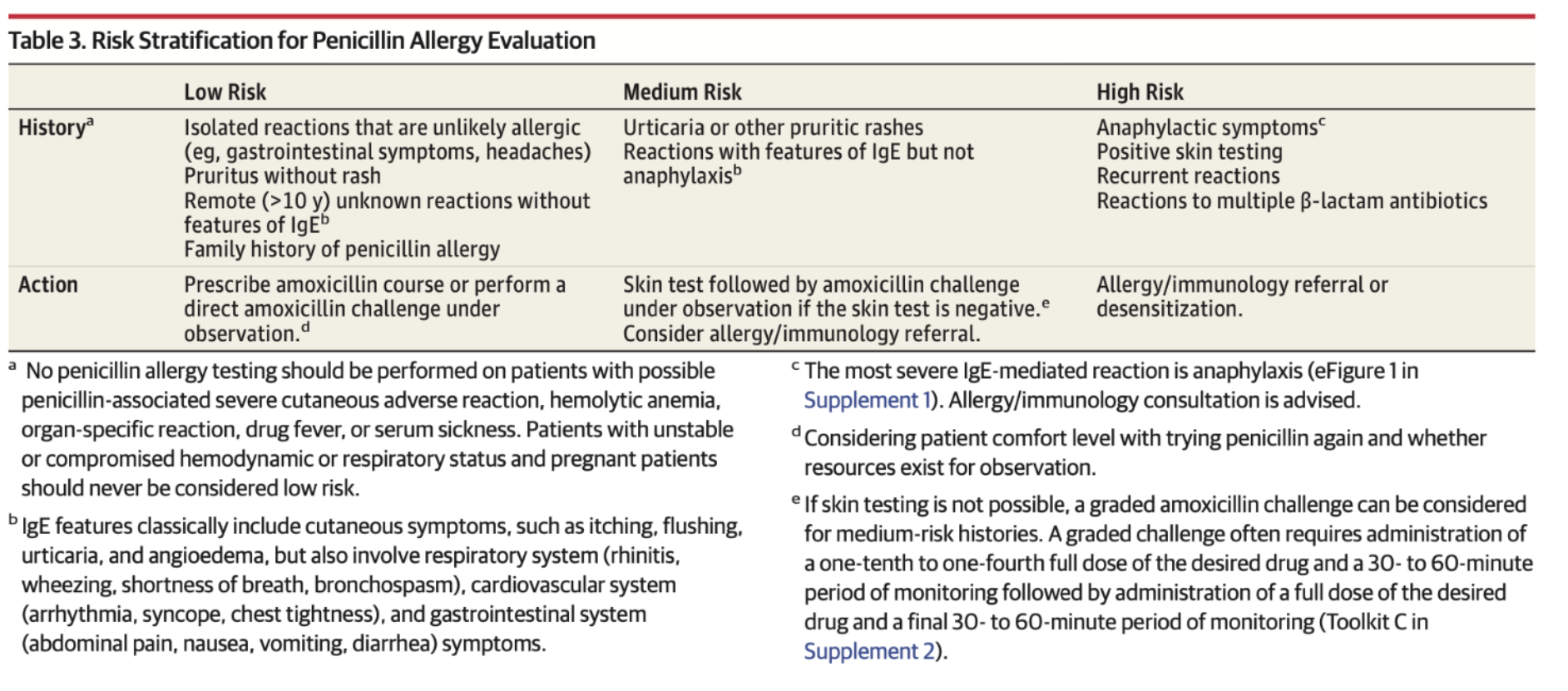
How to assess patient risk
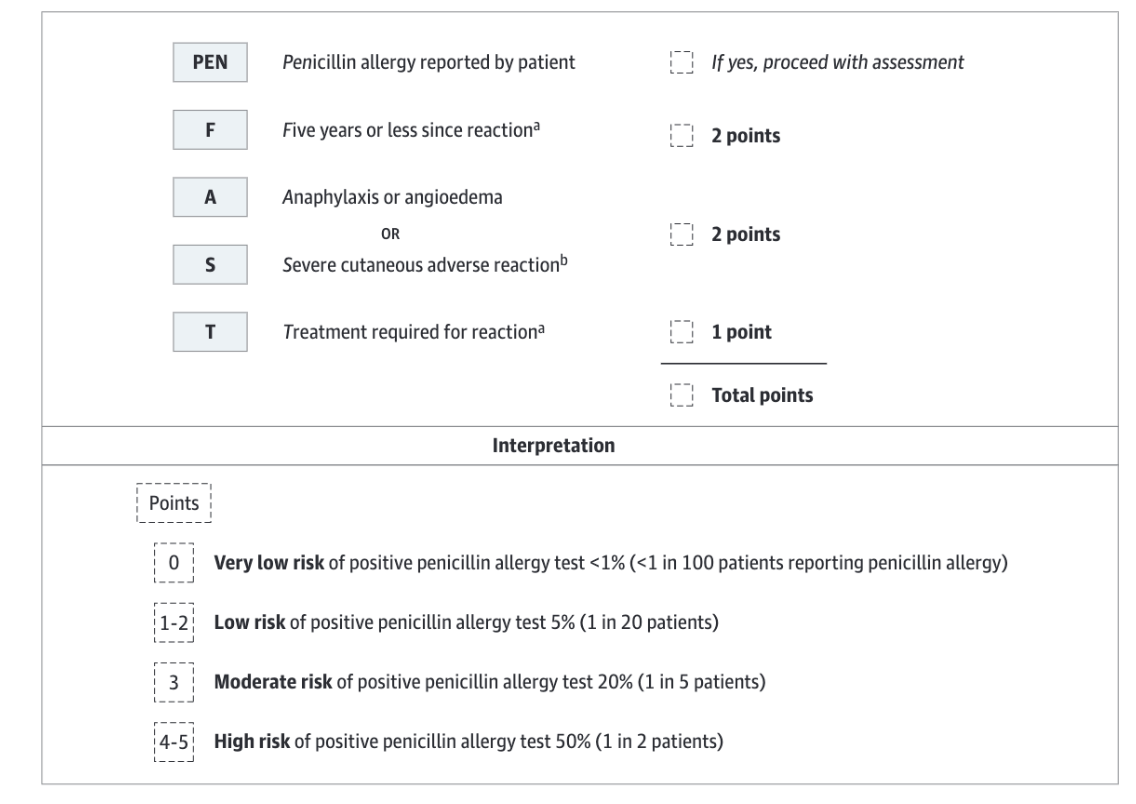
PENFAST score
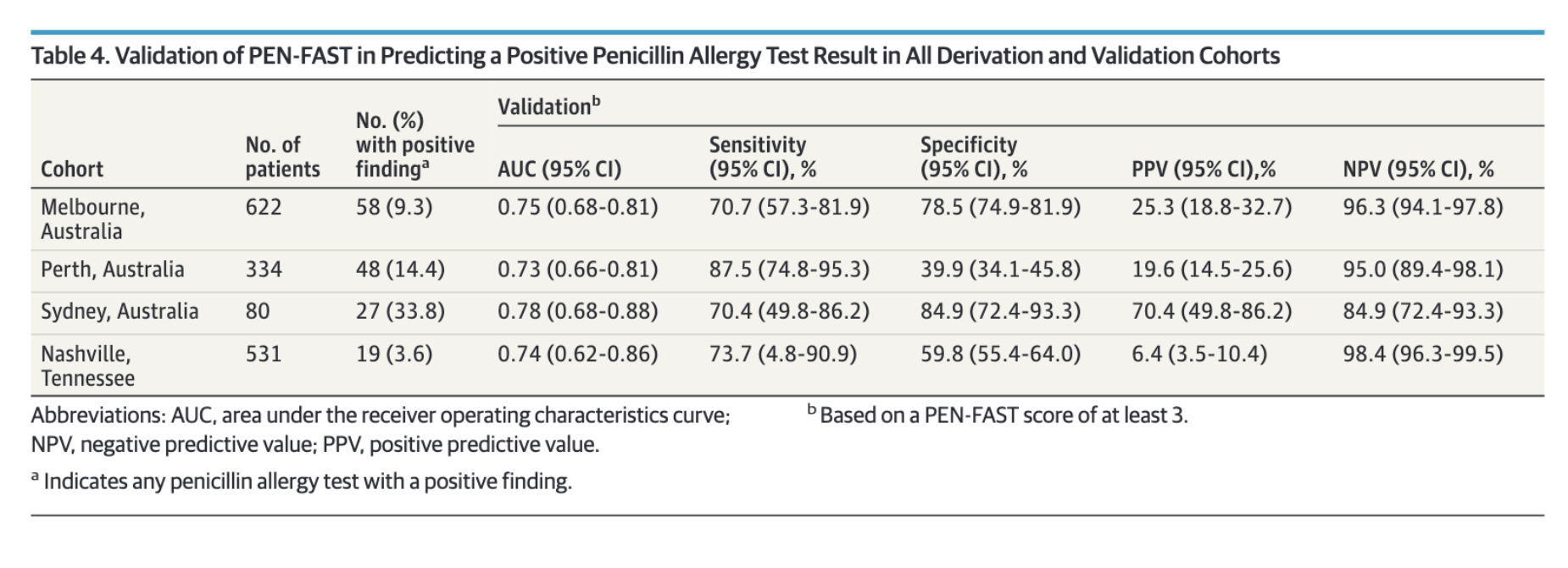
PENFAST performance
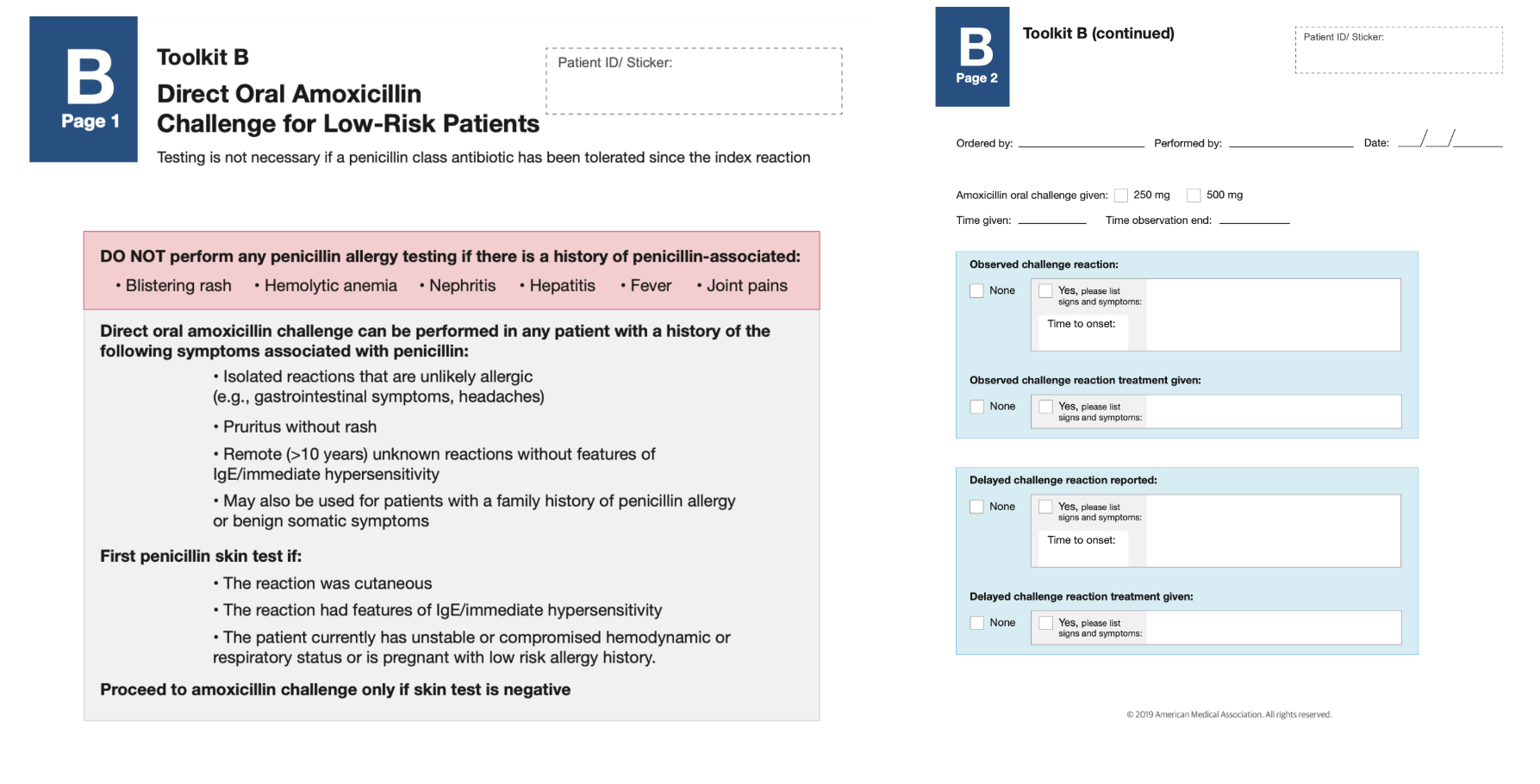
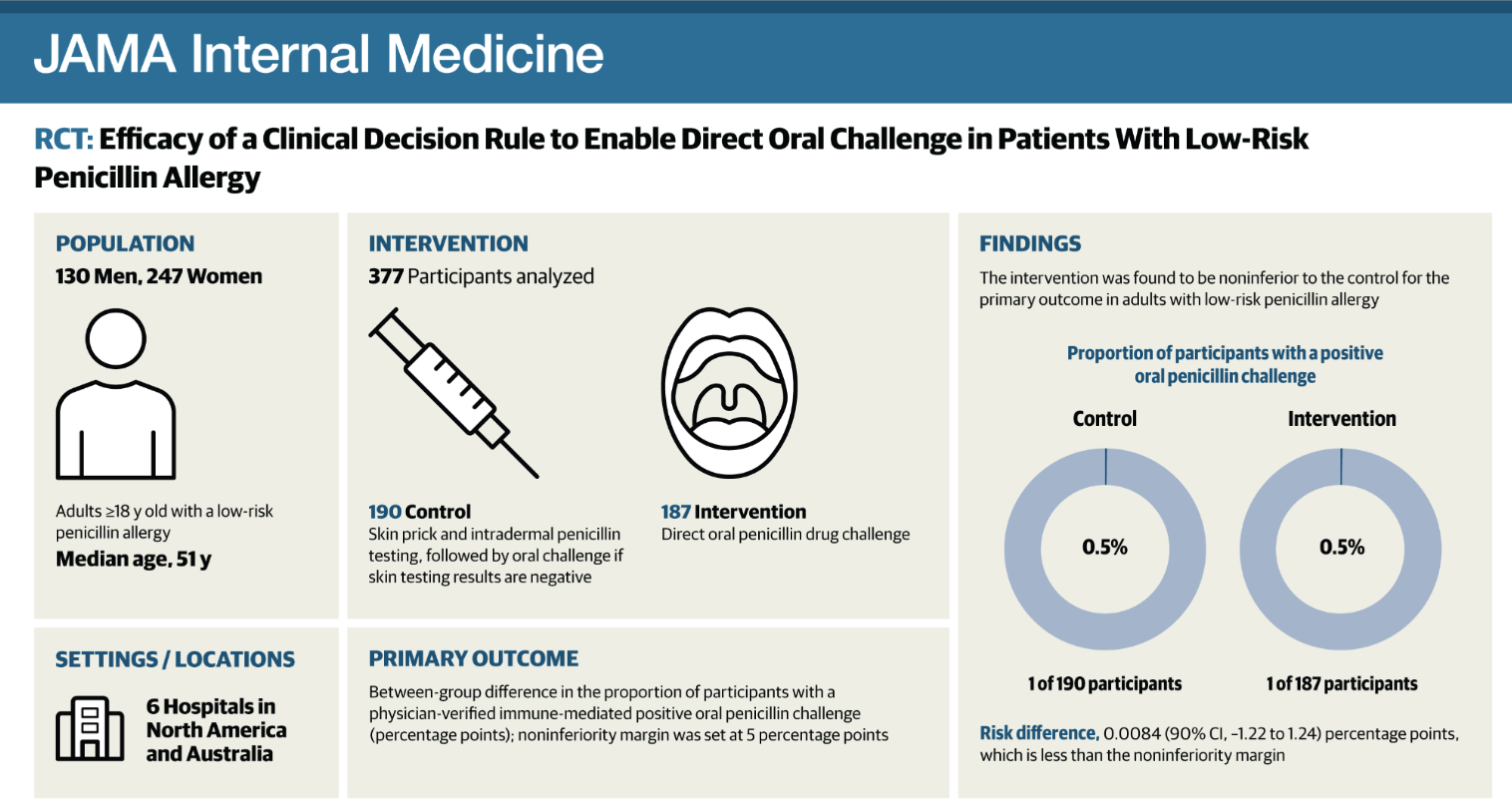
Direct oral amoxicillin challenge
Palace study
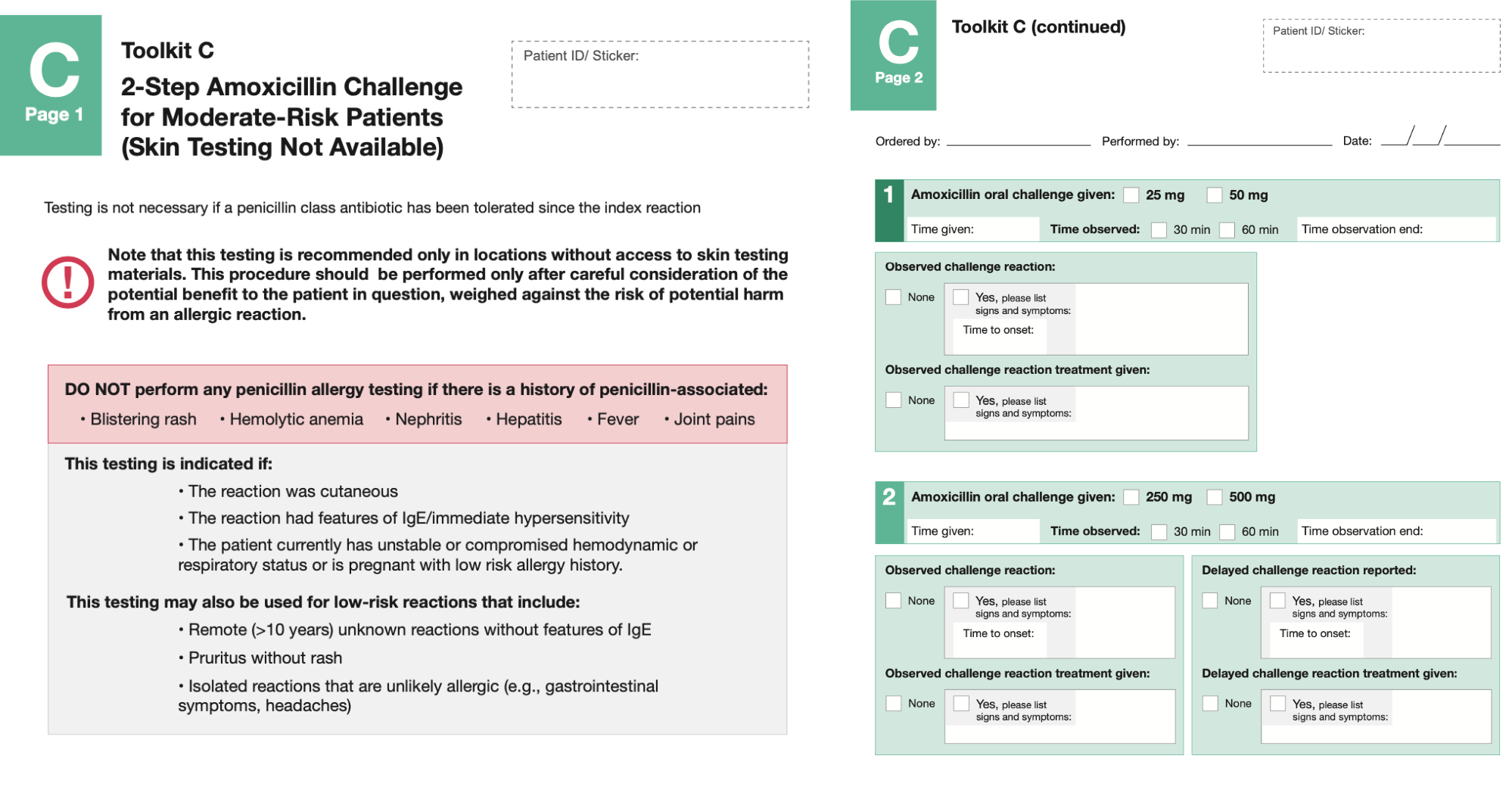
Two step oral amoxicillin challenge
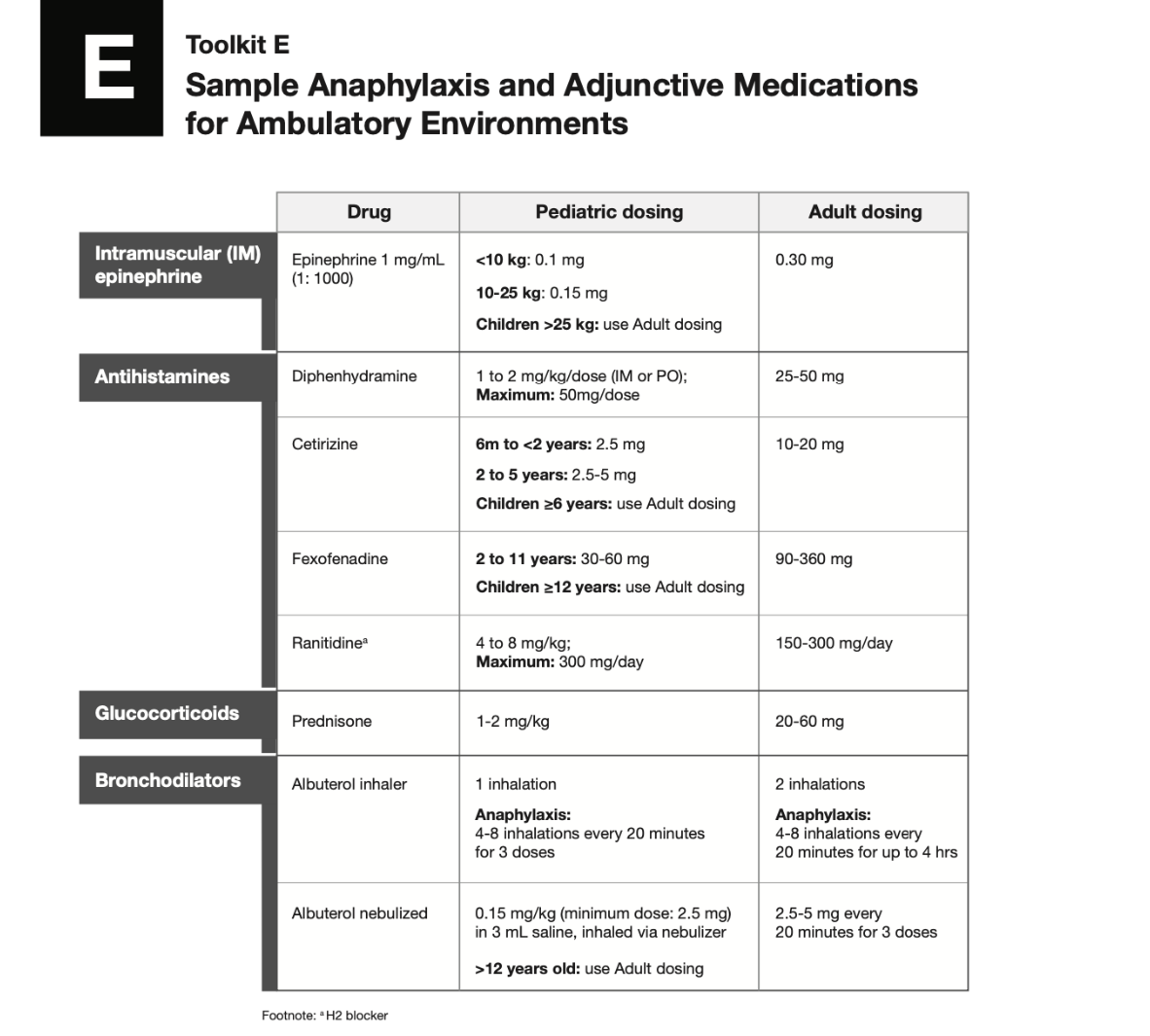
Anaphylaxis medications
How to assess patient risk
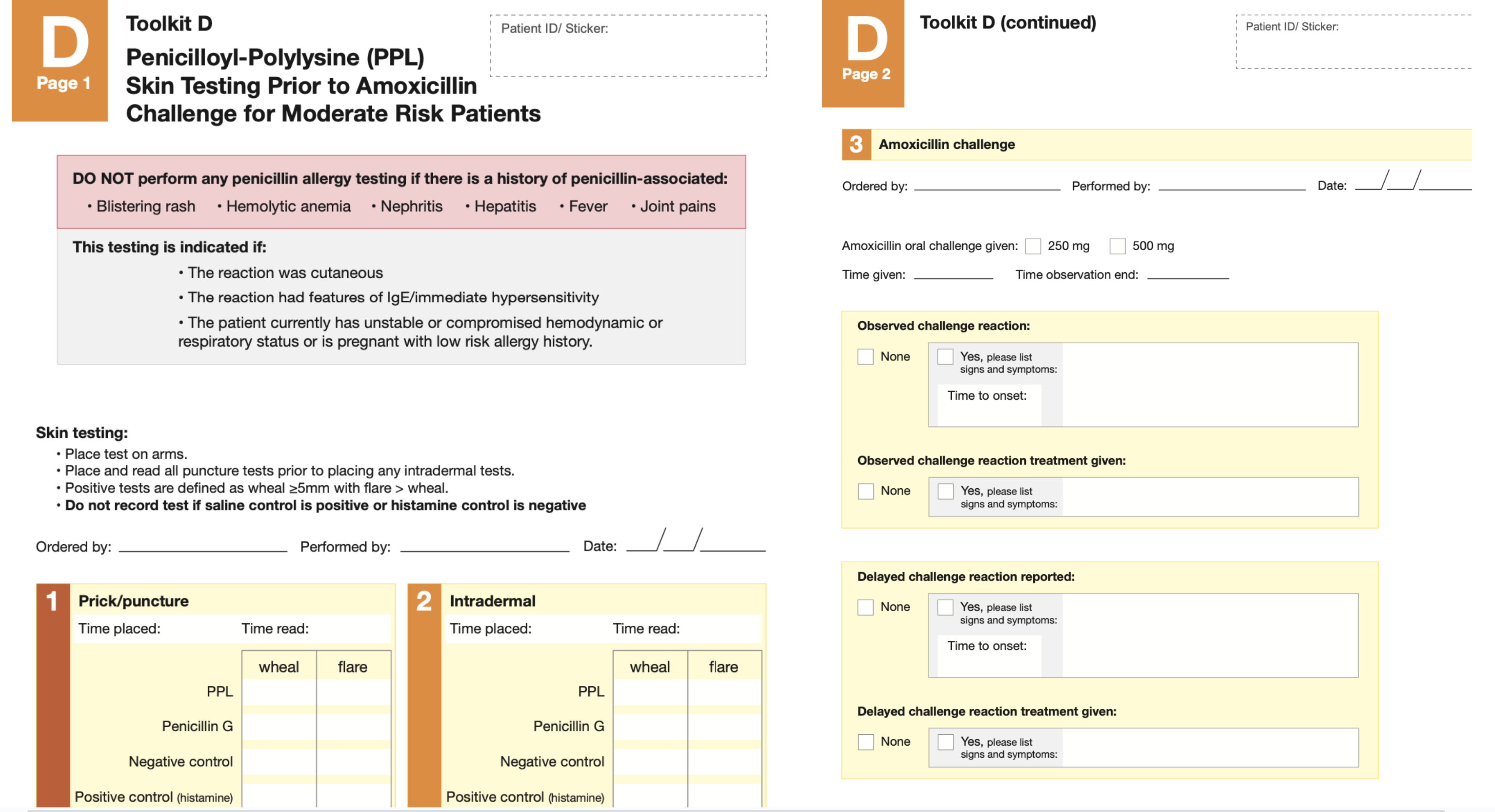
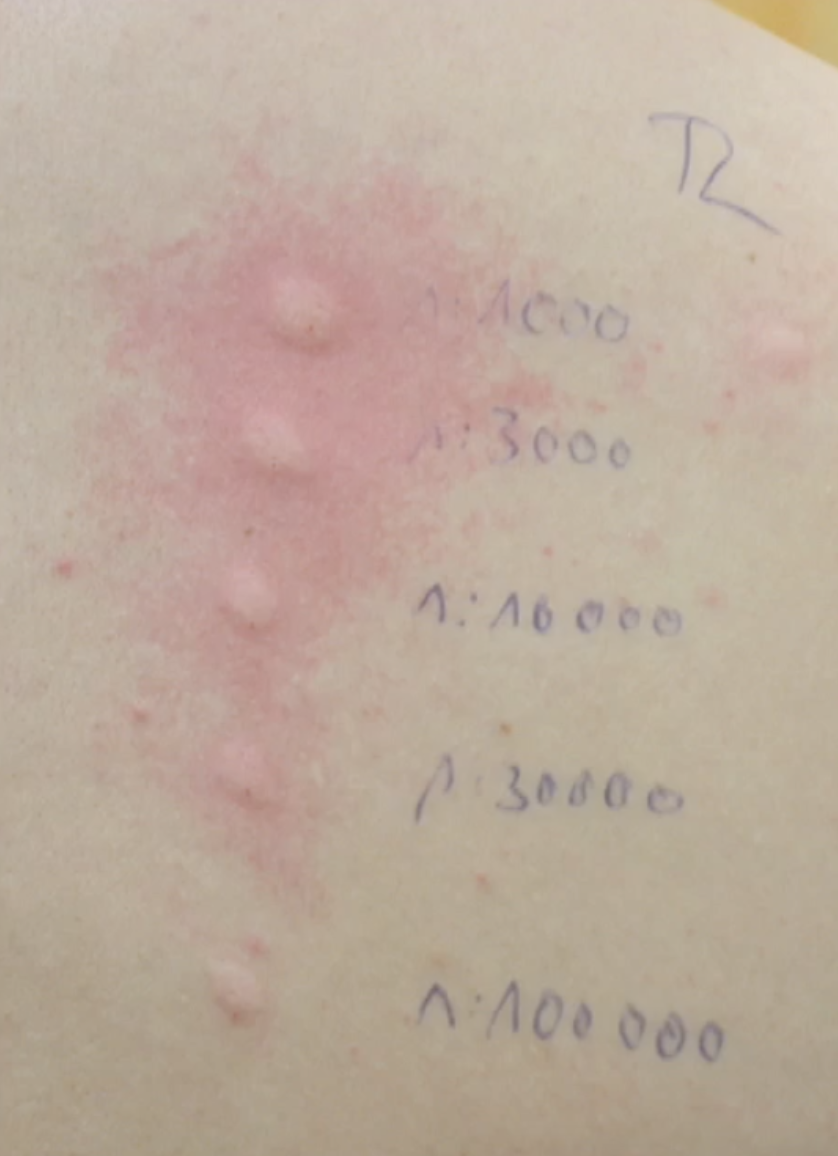
Skin testing
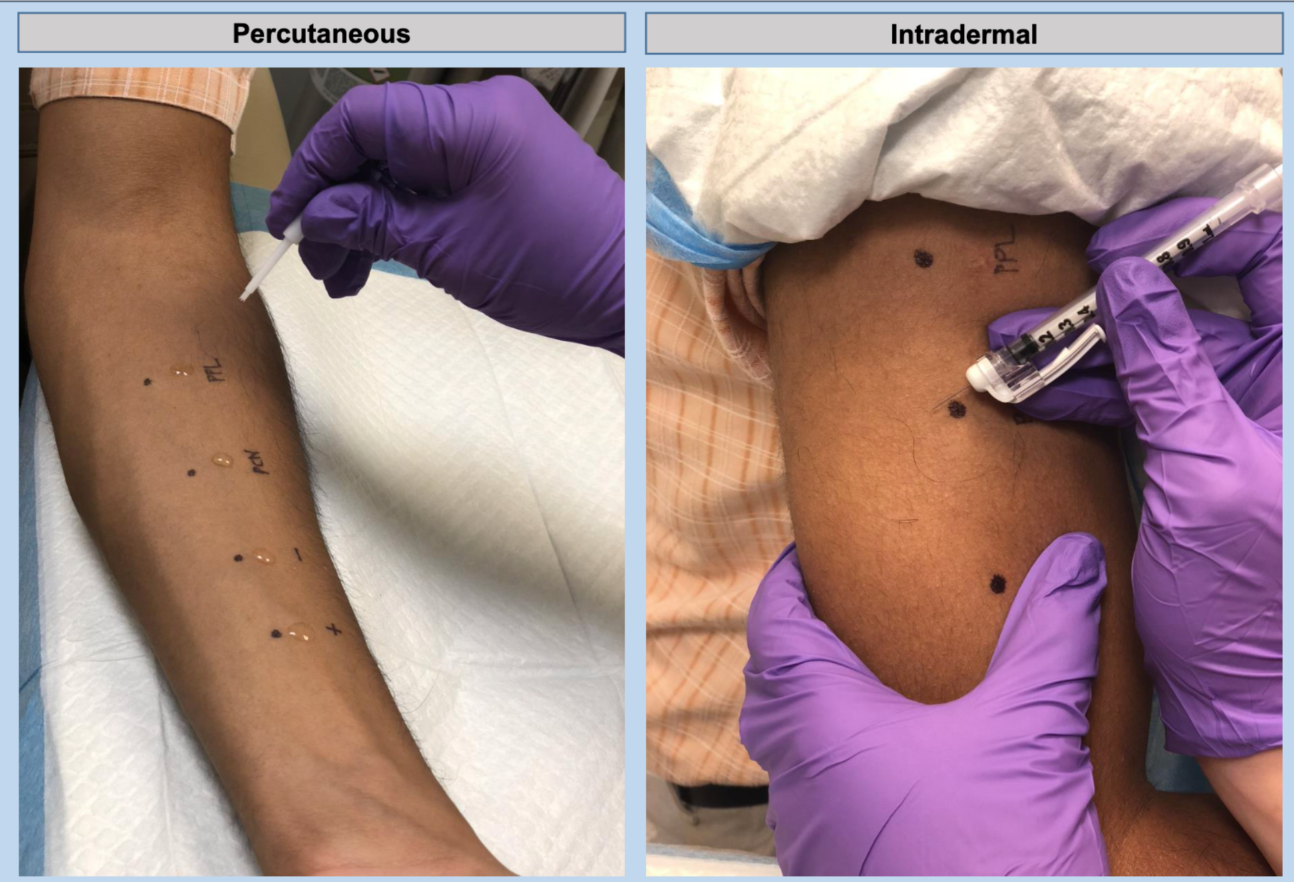
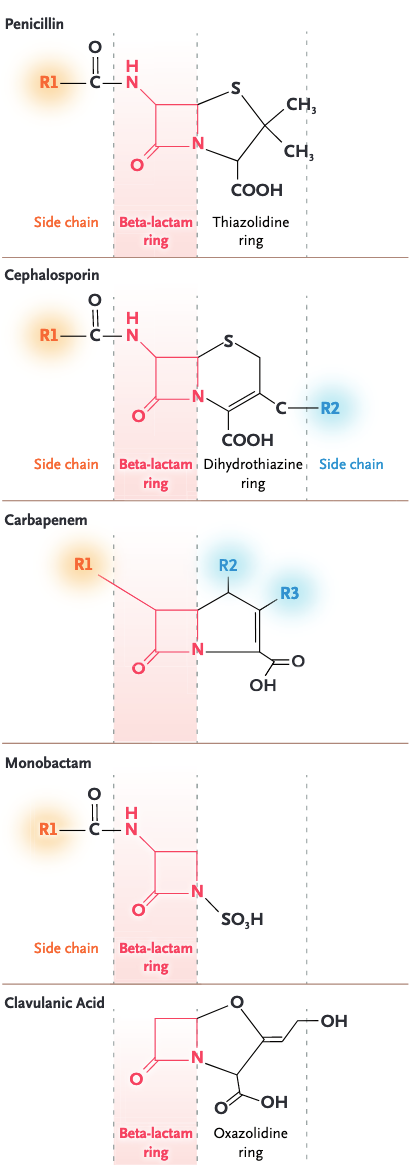
Allergic determinates
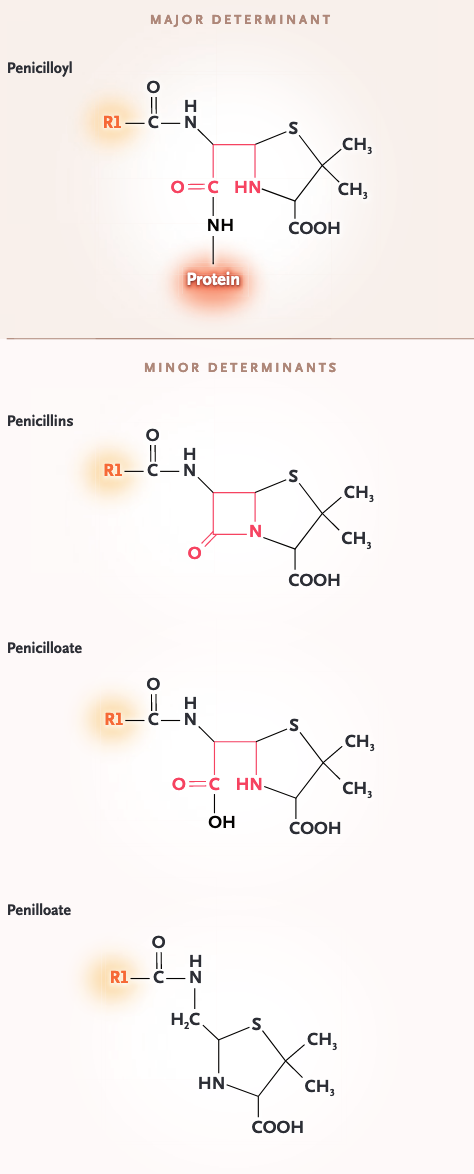
Penicillin skin test assessment

Penicillin skin test assessment
-Medium risk history
Sample desensitization protocol
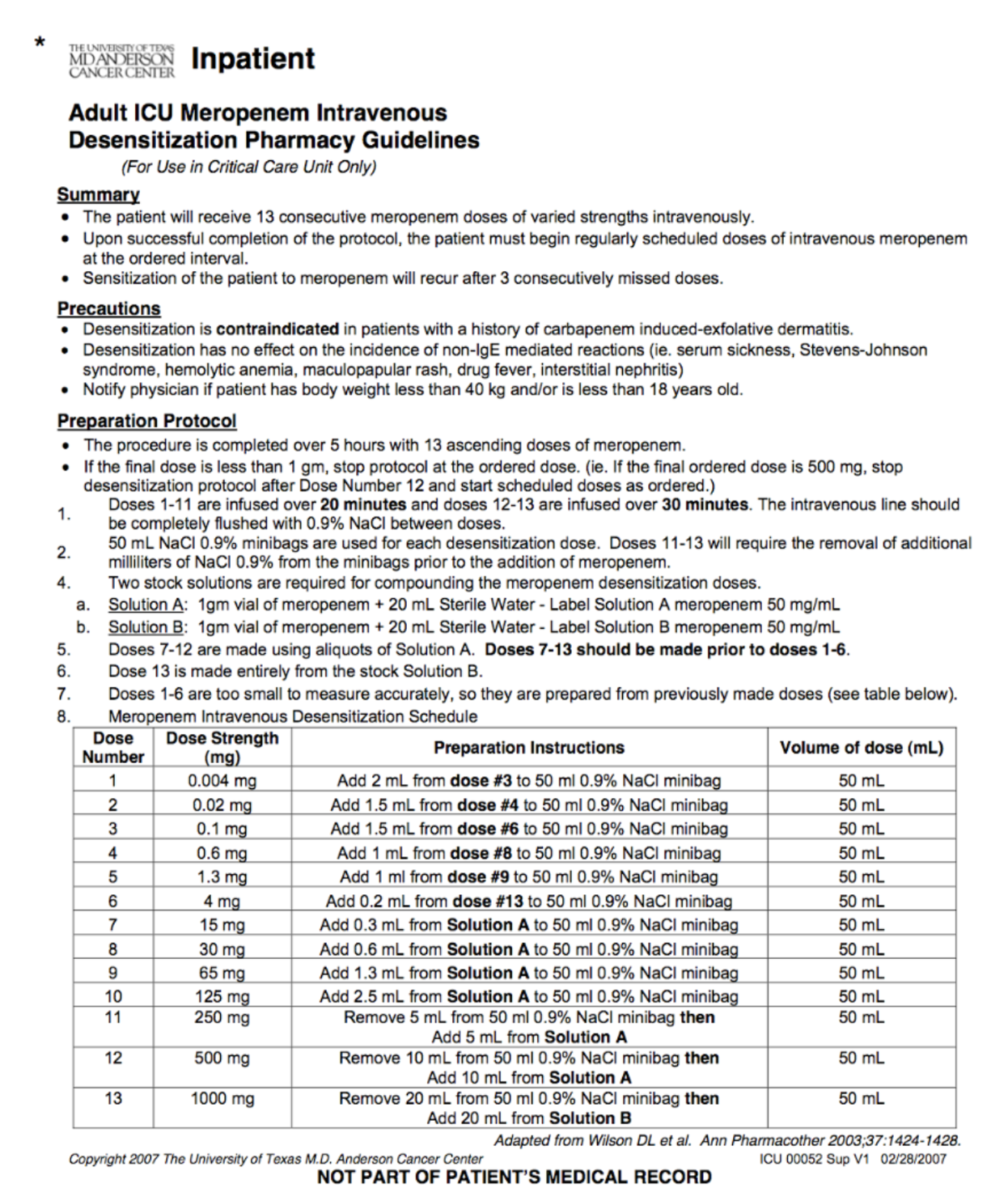
Other desensitization protocols
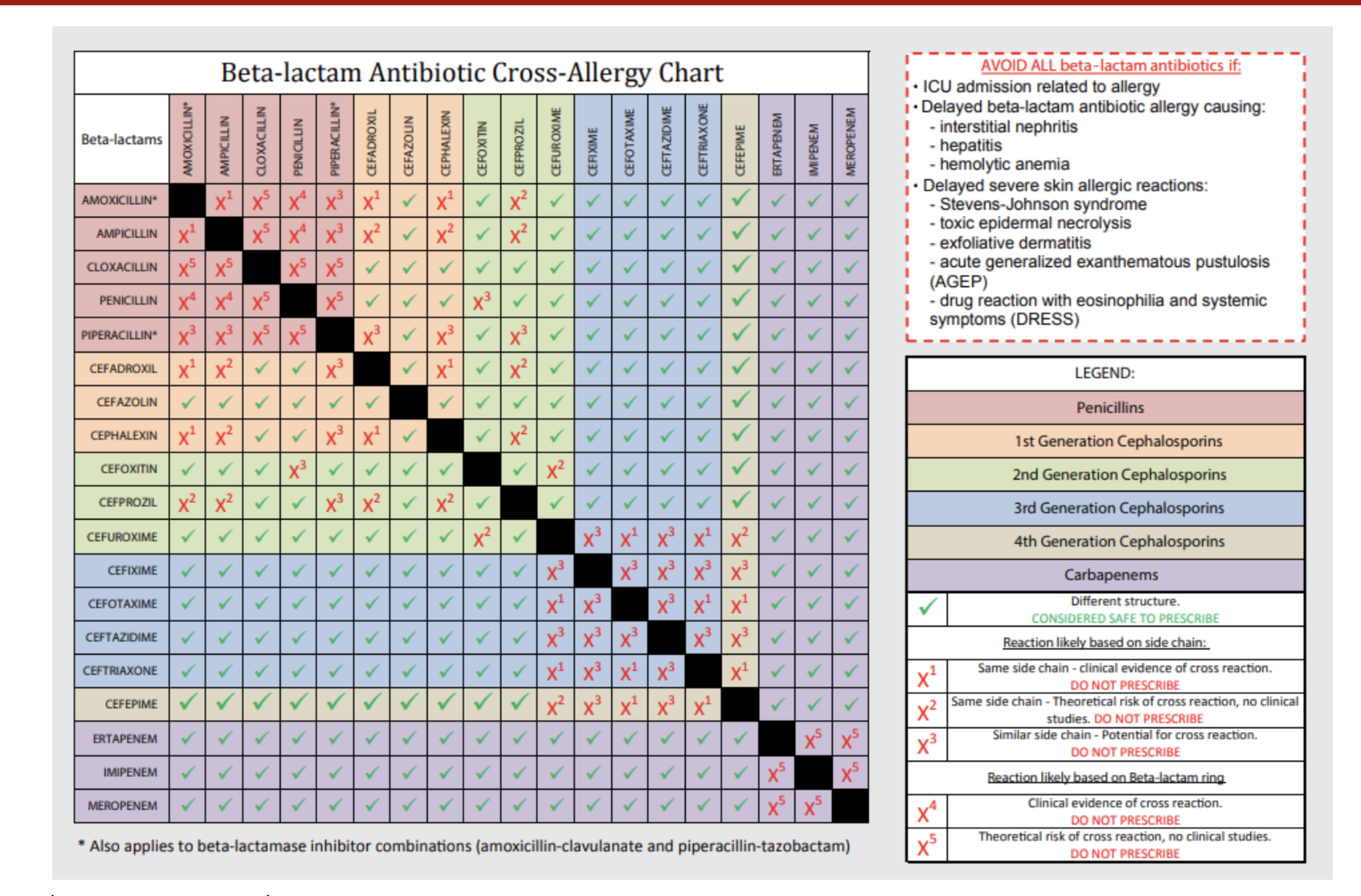
Risk of cross-reactivity related to cephalosporin sidechain
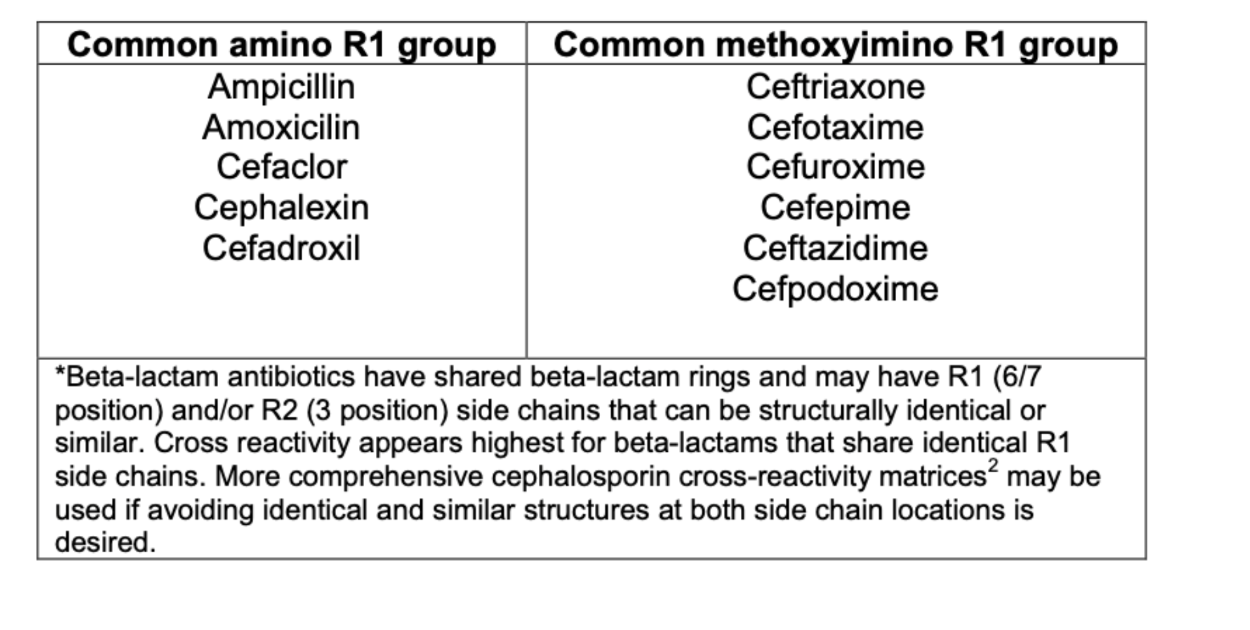
β-lactams with common side chains
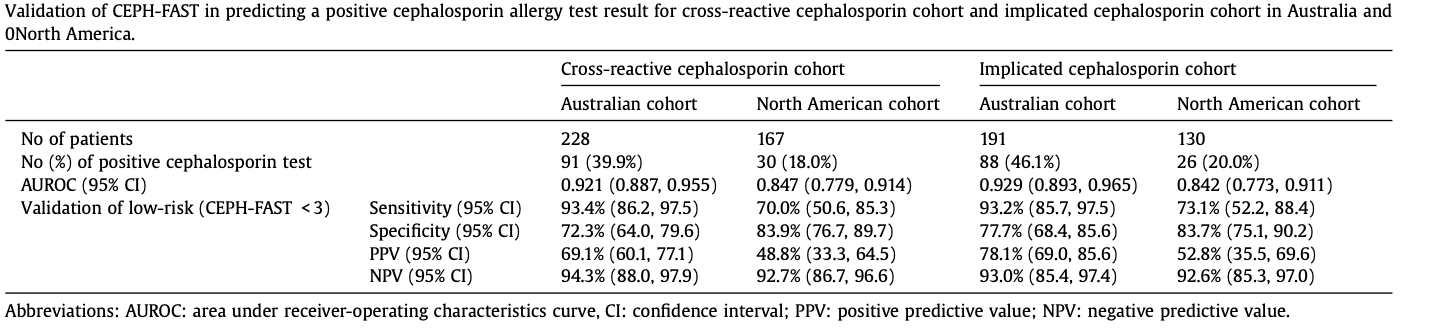
CEPHTEST: Application of PENFAST
score to cephalosporin allergies
Intradermal testing-Non beta-lactams
- Skin tests for most antimicrobial agents lack high negative predictive values, and skin test positivity is often a function of the time elapsed since the index reaction
- Prick and intradermal tests less well standardized- non-irritating formulations required
- Some antibiotics are irritating even at low concentrations, making testing difficult
- Special cellular activation tests may be available in some centers for some drugs
- e.g., The BAT (flow cytometry) detects the upregulation of activation markers CD63 and CD203c on the surface of basophils after incubation with the implicated drug
Approach to delayed-type
hypersensitivity testing

- Intradermal or patch testing with reading 24-72 hours
- Low sensitivity, high specificity
- Lymphocyte transformation testing
- Available in specialized laboratories
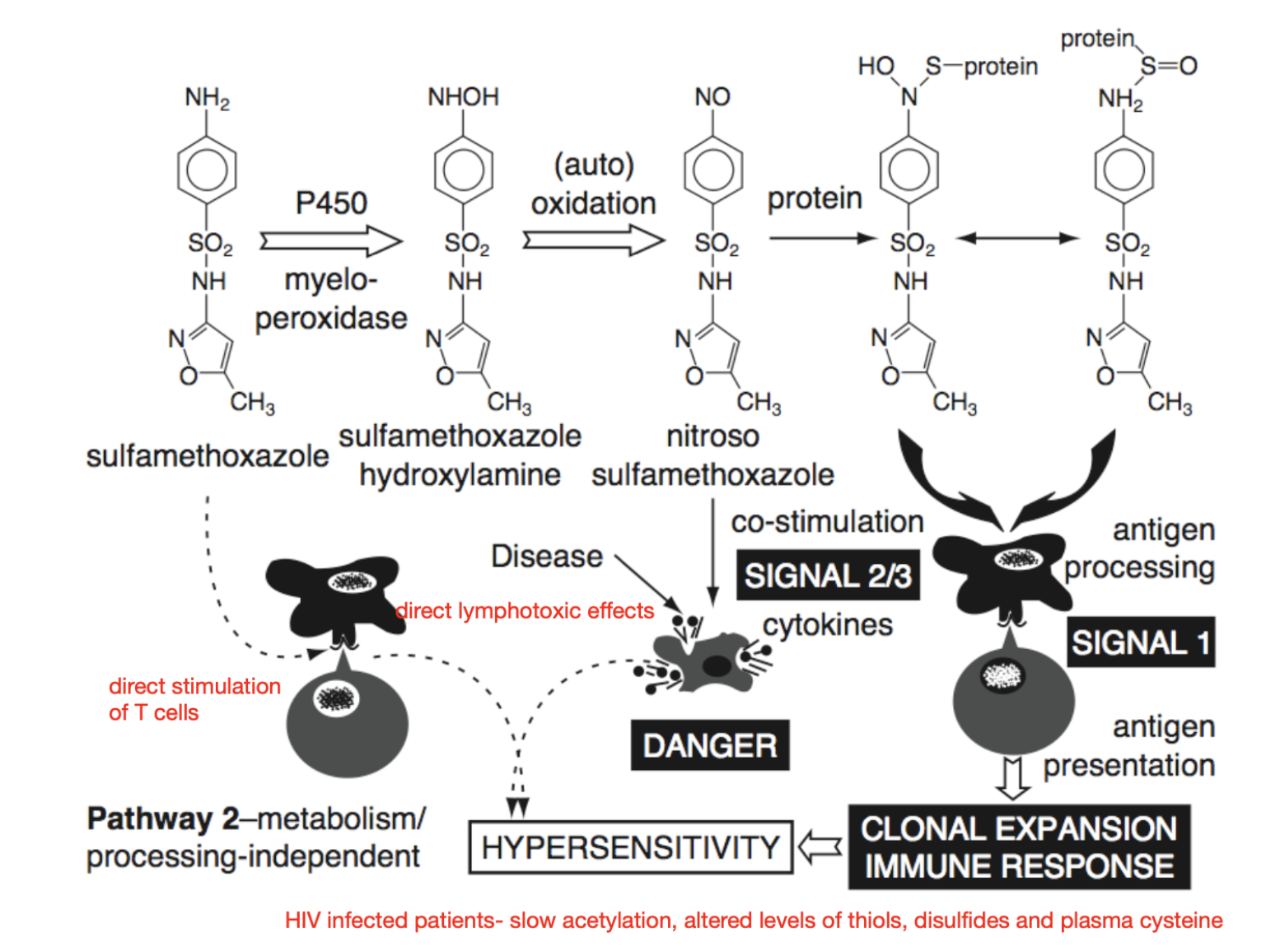
- Haptenization to become an antigen in vivo (hard to imitate in lab)
Mechanism of sulfonamide hypersensitivity
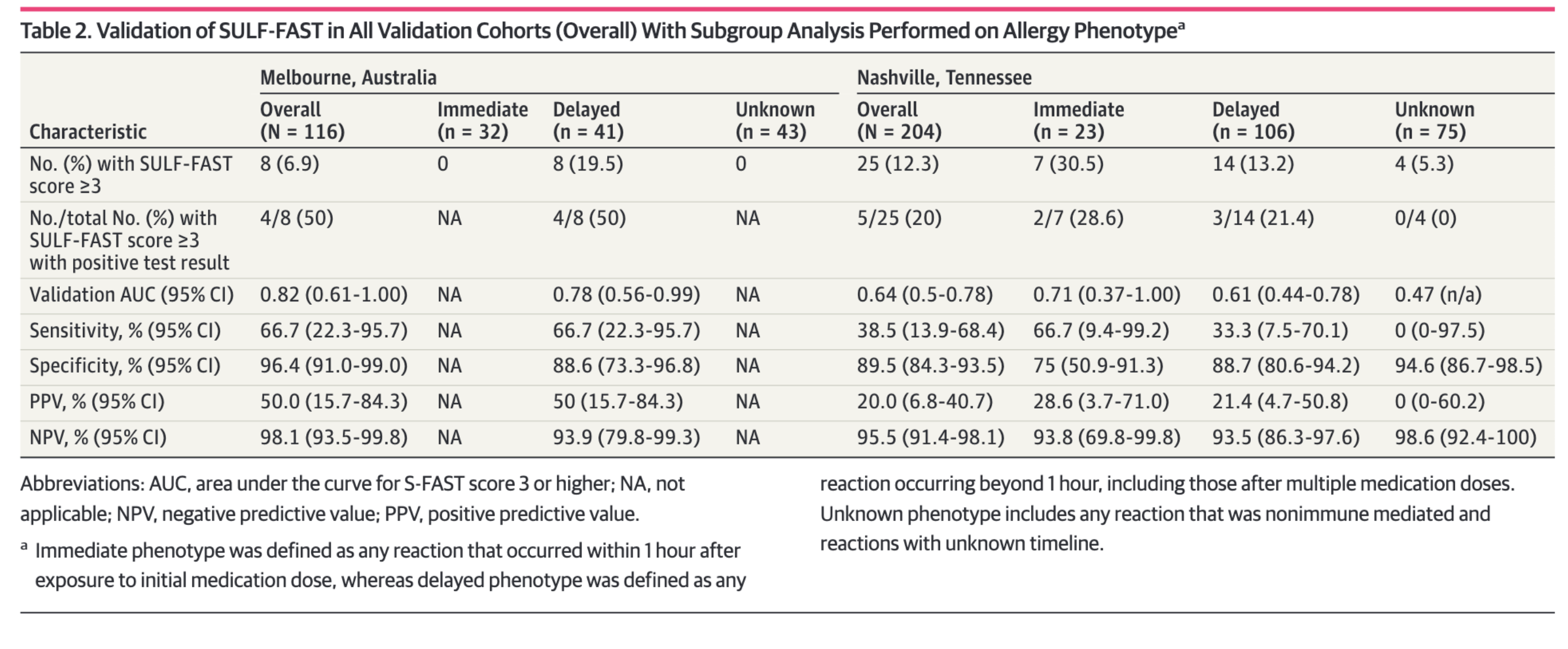
PENFAST score applied to sulfa allergies
Non-sensitizing allergic reactions
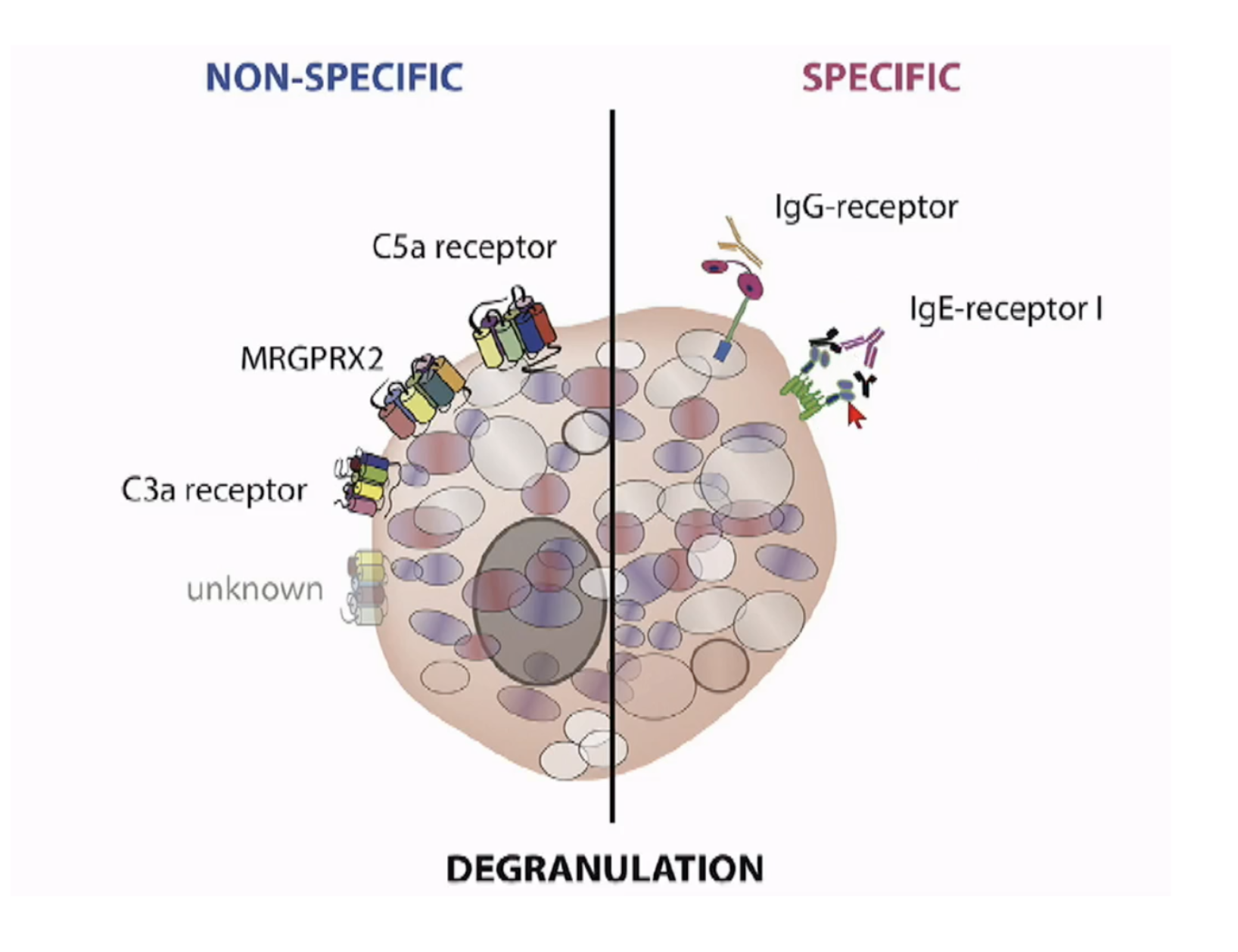
- Mas-related G protein coupled receptor (MRGPRX2)
- Neuromuscular blocking agents
- Opioids
- Radiocontrast media
- Vancomycin, glycopeptides, fluoroquinolones
- Complement-activation-related pseudoallergy (CARPA)
- Liposomes, drug carriers
Vancomycin infusion reaction
“red man syndrome”
- Vancomycin can also cause:
- Hypotension, anaphylaxis
- Maculopapular exanthems
- Vasculitis E
- Eosinophilia Exfoliative dermatitis/DRESS/Stephens-Johnson