Oxazolidinones
Oxazolidinones
Russell E. Lewis
Associate Professor of Infectious Diseases (MEDS-10/B)

russelledward.lewis@unipd.it
https://github.com/Russlewisbo
Slides and course materials: www.idpadova.com
Learning objectives
- Describe the chemical features that distinguish linezolid and tedizolid and the structural basis for activity against cfr-carrying strains
- Explain the mechanism of action and why oxazolidinones avoid cross-resistance with β-lactams, glycopeptides, daptomycin and quinupristin-dalfopristin
- Recognize the four major resistance mechanisms and their clinical implications
- Apply PK/PD principles, dosing and TDM thresholds in adults, including special populations
- Choose oxazolidinones appropriately in MRSA, VRE, MDR-TB, and Nocardia infections
- Anticipate, monitor for, and manage hematologic, neurologic, metabolic, and serotonergic toxicities
Overview and chemistry
A fully synthetic antibiotic class
- Oxazolidinones are prepared entirely by organic synthesis — no fermentation product
- 1978: DuPont patents 5-(halomethyl)-3-aryl-2-oxazolidinones with activity against plant pathogens
- Further optimization → first agents with activity against human pathogens
Two FDA/EMA-approved agents
| Drug | Trade name | FDA approval |
|---|---|---|
| Linezolid | Zyvox | April 2000 |
| Tedizolid (phosphate) | Sivextro | June 2014 |
- Investigational agents: sutezolid, radezolid, delpazolid, contezolid
- No drug-class cross-resistance with β-lactams, vancomycin, daptomycin, or quinupristin-dalfopristin
Basic oxazolidinone scaffold
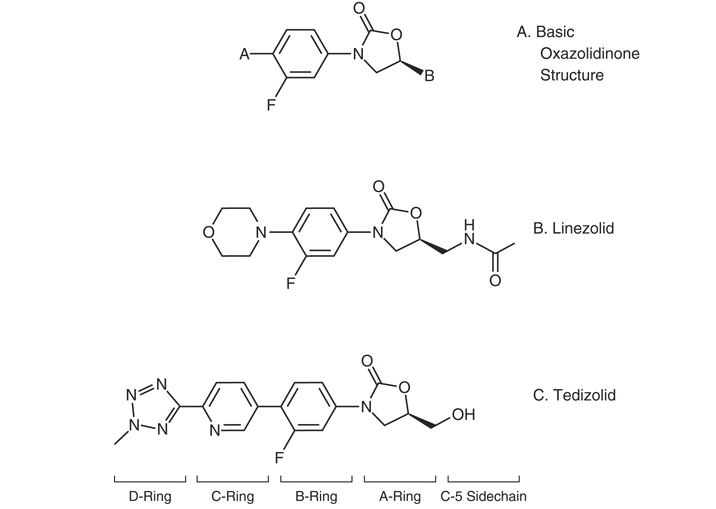
- Core five-membered 2-oxazolidinone ring (the “A-ring”)
- C5 modification of the A-ring and N-aryl B-ring are essential for antibacterial activity
- Fluorination of the B-ring further increases potency
Linezolid — structural features
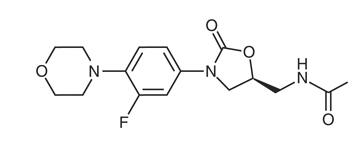
- C5 acetamide side chain on the A-ring
- N-aryl B-ring with single fluorine
- Single morpholine D-substituent
- Sufficient for activity against typical Gram-positive targets
Tedizolid — engineered for breadth
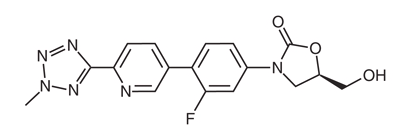
- C5 hydroxymethyl group replaces acetamide → preserves activity against cfr-carrying strains
- Added pyridine (C-ring) and tetrazole (D-ring) moieties → lower MICs
- Administered as the phosphate prodrug (Sivextro)
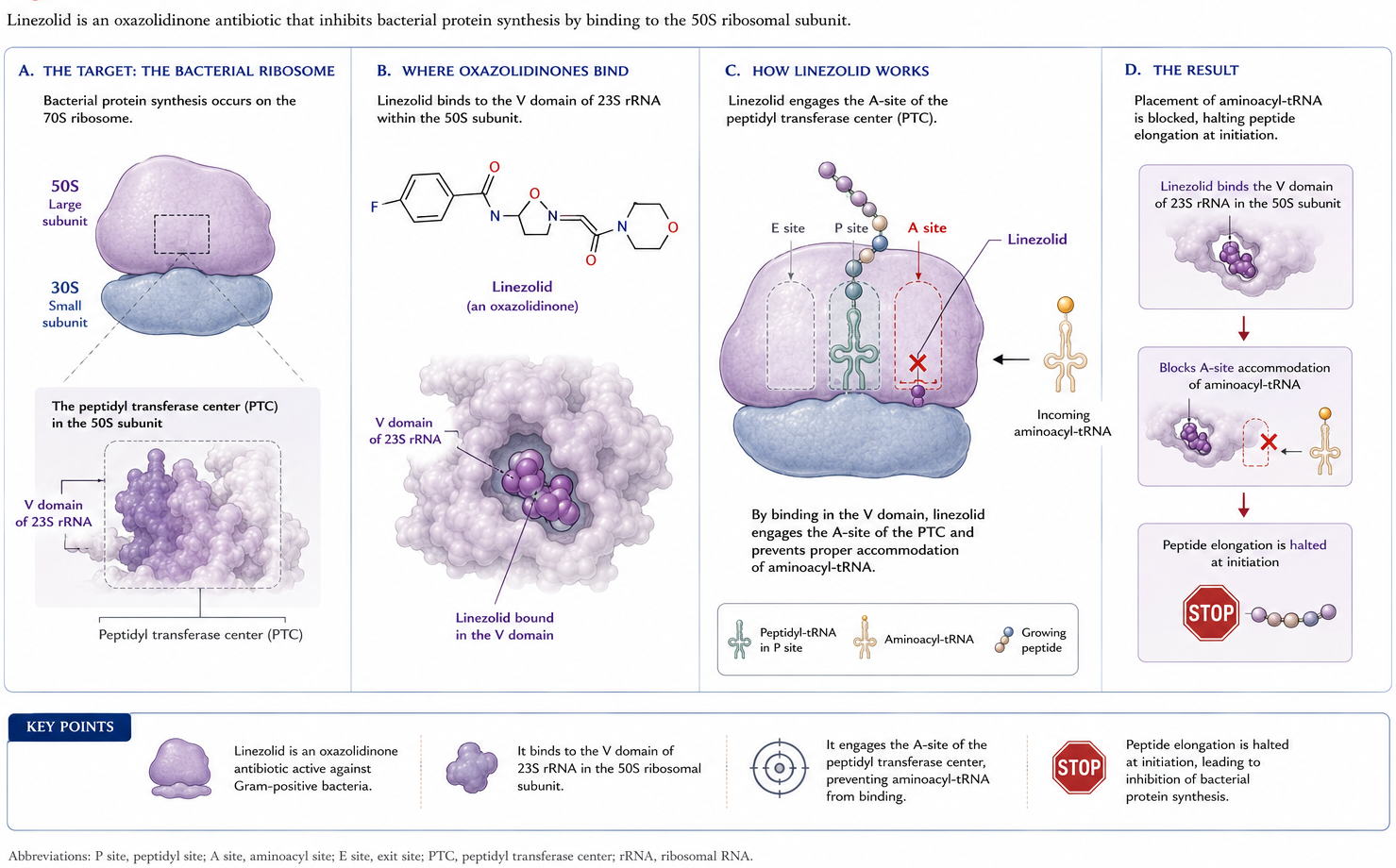
Mechanism of action
Where do oxazolidinones bind?
Bacteriostatic — and why that’s fine
- Generally bacteriostatic against staphylococci and enterococci; modestly bactericidal against streptococci
- “Static vs cidal” distinction may be clinically overrated — systematic reviews have found no consistent outcome difference
- Don’t withhold linezolid in S. aureus bacteremia on cidal-vs-static grounds alone
Spectrum of activity
Aerobic Gram-positive activity
| Organism | Linezolid MIC₉₀ (μg/mL) | Tedizolid MIC₉₀ (μg/mL) |
|---|---|---|
| MSSA | 2 | 0.25 |
| MRSA | 2 | 0.25 |
| S. agalactiae | 2 | 0.25 |
| S. anginosus gp | 1 | 0.25 |
| S. pyogenes | 2 | 0.25 |
| E. faecalis | 2 | 0.25 |
| E. faecalis (LZD-NS) | 8 | 1 |
| E. faecium | 2 | 0.5 |
Tedizolid is more potent in vitro — but…
- Tedizolid MICs are 2–8× lower than linezolid across most Gram-positive species
- Lower MIC ≠ better clinical outcome without head-to-head trials
- CLSI: tedizolid susceptibility can be inferred from linezolid susceptibility for S. aureus, E. faecalis, S. agalactiae, S. pyogenes, S. anginosus
- Linezolid-resistant strains may still be tedizolid-susceptible
Mycobacteria
- Excellent activity against MDR- and XDR-M. tuberculosis
- Linezolid MIC range: 0.125–2 μg/mL
- Tedizolid MIC range: 0.125–0.5 μg/mL
- Active against rapid growers (M. abscessus spp., M. massiliense) and slow-grower M. kansasii
- Higher MICs for M. avium / M. intracellulare
Nocardia and other higher-order bacteria
- Linezolid: virtually 100% in vitro susceptibility across Nocardia spp.
- MIC₉₀ 1–4 μg/mL
- Tedizolid: lower MICs than linezolid for most Nocardia spp.
- Comparable to linezolid for N. nova complex and N. brasiliensis
- Variable activity vs. actinomycetes; Corynebacterium, Listeria, Bacillus, Erysipelothrix, Rhodococcus equi, Leuconostoc, Pediococcus — case-by-case
Where oxazolidinones do NOT shine
- Aerobic Gram-negatives: limited
- Incomplete coverage of respiratory pathogens H. influenzae and Moraxella catarrhalis
- Anaerobes: decent activity against both Gram-positive and Gram-negative anaerobes
- Clostridium spp., Bacteroides spp.
Resistance
The headline numbers
- Linezolid resistance reported pre-marketing (Compassionate Use Program, VRE)
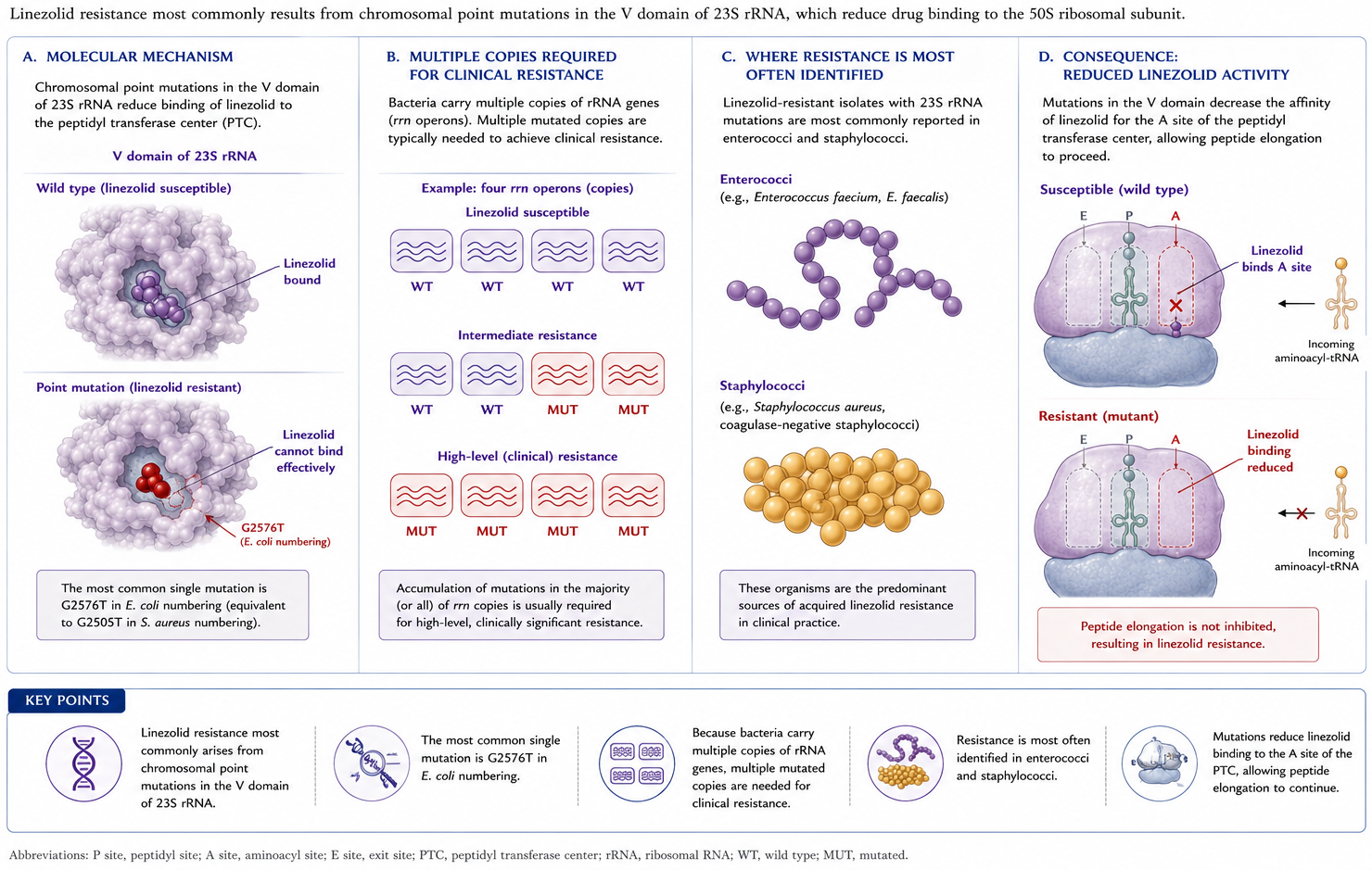
- ~25 years post-launch, resistance still <1% of clinical isolates
- Tedizolid resistance rarer than linezolid resistance over a 5-year surveillance
- Enterococci > staphylococci for resistance frequency
Risk factors for resistance
- Prior linezolid exposure
- Prolonged therapy (weeks to months)
- Horizontal spread within ICUs and long-term care facilities
- Stewardship implication: limit duration, monitor when prolonged use unavoidable
Mechanism 1 — 23S rRNA mutations
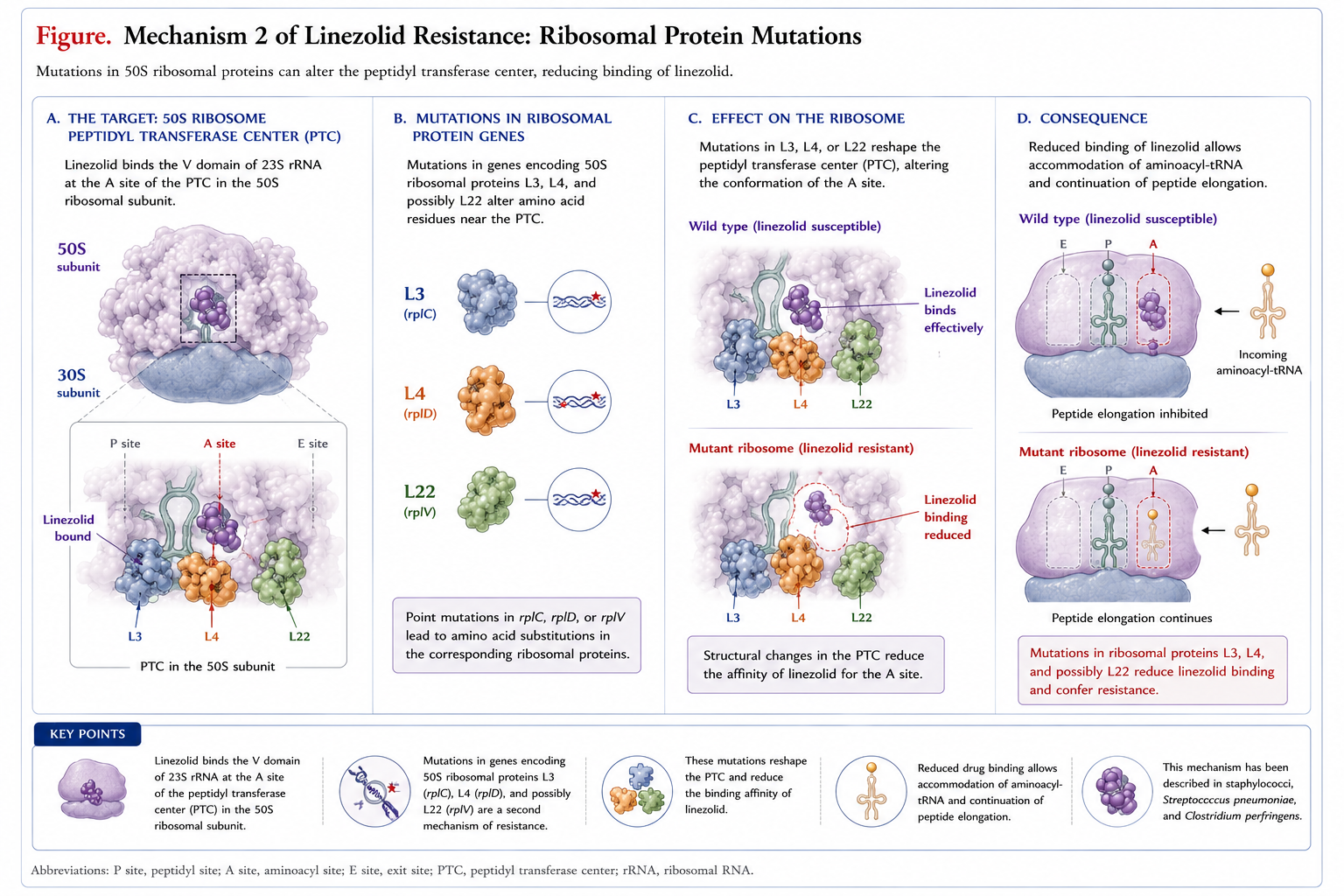
Mechanism 2 — ribosomal protein mutations
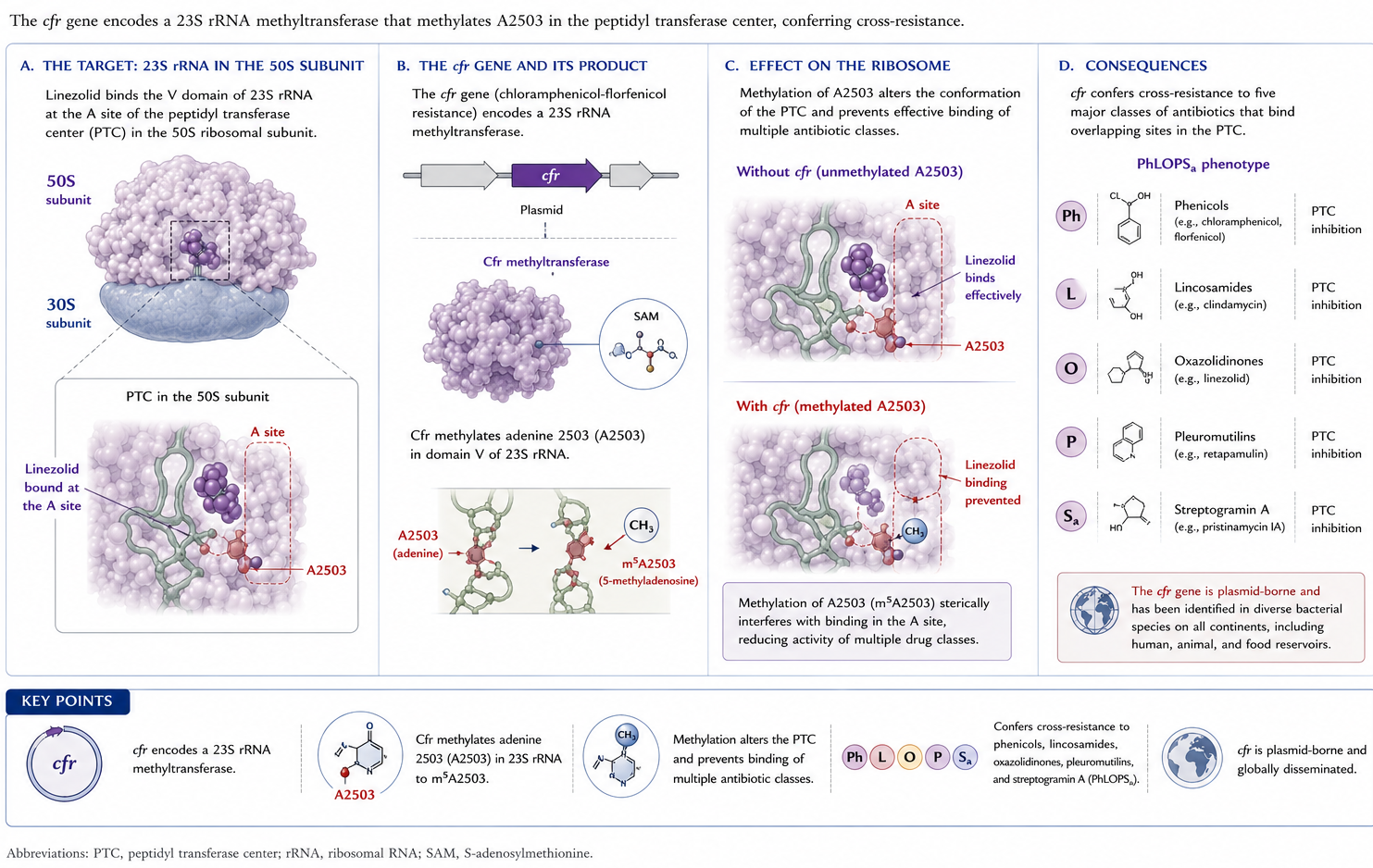
Mechanism 3 — cfr methyltransferase
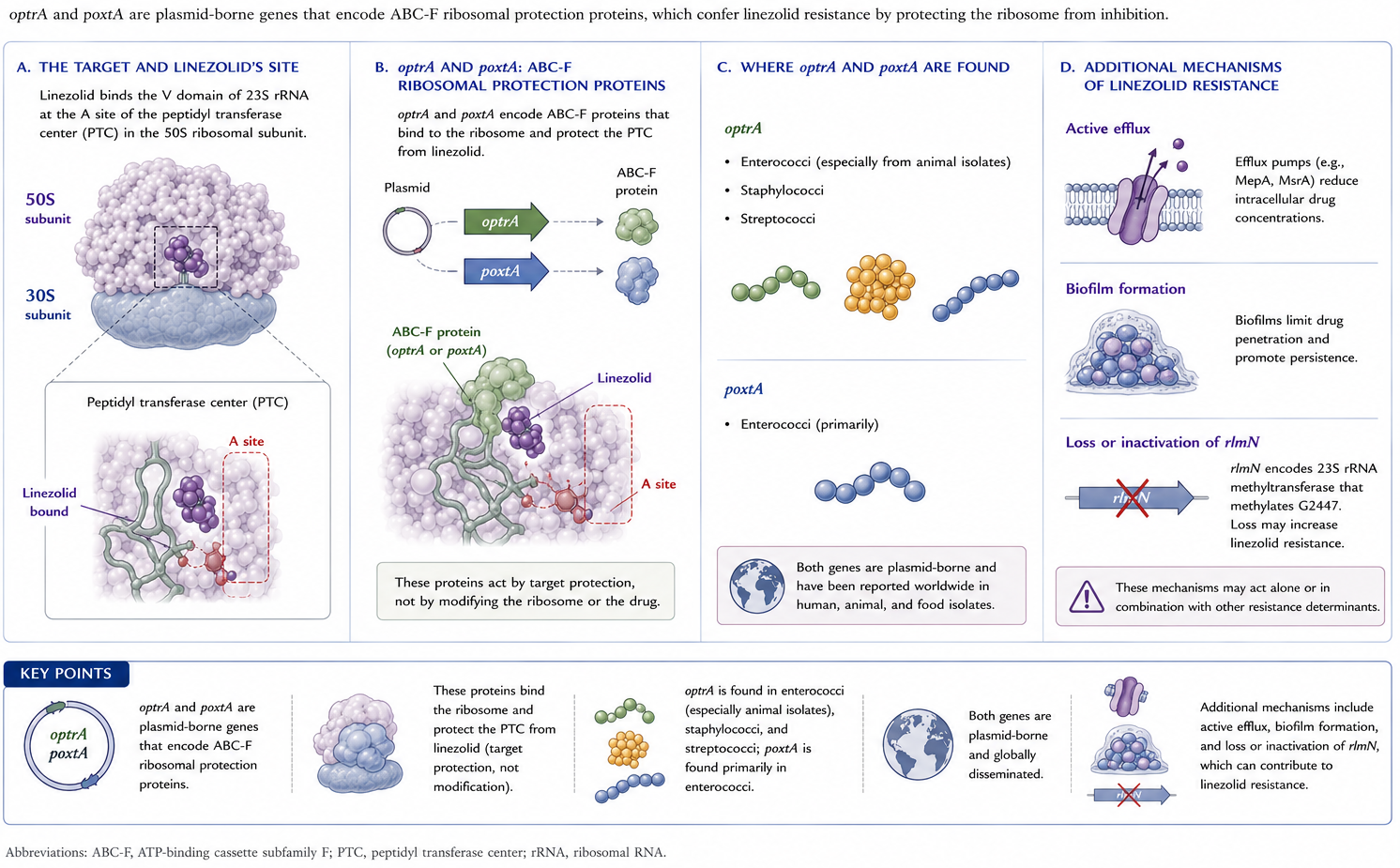
Mechanism 4 — optrA and poxtA
Tedizolid vs. linezolid-resistant strains
- Tedizolid retains activity against many cfr-positive strains of S. aureus, CoNS, and enterococci
- Activity lost when cfr coexists with chromosomal ribosomal mutations
- Practical message: test before assuming susceptibility in known LZD-R isolates
Pharmacology — linezolid
Linezolid — dosing fundamentals
- Adults / adolescents: 600 mg PO or IV every 12 hours
- Uncomplicated SSTI in adults: 400 mg every 12 hours
- Pediatric (birth–11 y): 10 mg/kg every 8 hours (every 12 h for uncomplicated SSTI in children 5–11 y)
- Bioavailability ~100% — oral and IV interchangeable
Linezolid — distribution
- Plasma protein binding: 31%
- Excellent penetration into lung (ELF, alveolar macrophages) and skin and soft tissue
- CSF: trough <0.2–7.0 μg/mL; peaks 3.1–12.5 μg/mL in meningitis; CSF/plasma ratio 0.77–1.0
- Bone and joint penetration variable — case-by-case
Linezolid — metabolism and clearance
- Metabolized by oxidation — minimal CYP450 interaction
- 65% nonrenal clearance; 30% excreted unchanged in urine
- Two inactive carboxylic-acid metabolites in feces
- Linezolid undergoes non-CYP3A4 oxidative metabolism, mainly morpholine-ring oxidation/ring opening, producing inactive metabolites A and B. The enzymatic component appears to involve atypical CYP4F enzymes, especially CYP4F3B and CYP4F11, rather than conventional hepatic CYP450 metabolism
- Half-life ~5–7 hours in adults
- Hemodialysis removes linezolid → dose after dialysis
- CRRT also removes drug; no routine dose change recommended
Linezolid — PK/PD targets
- Driver of efficacy: fT > MIC ≈ 85% and AUC₀₋₂₄/MIC 80–120
- High inter-individual variability can compromise targets at standard dose
- At-risk populations:
- Overexposure: renal dysfunction, older age, hepatic failure, low body weight
- Under-exposure: augmented renal clearance, younger age, obesity
- Both: critical illness
Linezolid — when to consider TDM
- Trough Cmin 2–7 mg/L suggested for Gram-positive infection
- Cmin <2 mg/L proposed for M. tuberculosis (MICs lower)
- Cmin >7.5–22.1 mg/L → hematologic toxicity risk rises
- Strongest case for TDM: critically ill, prolonged therapy, renal dysfunction, drug interactions
Linezolid — drug interactions (PK)
- Rifampin → ↓ AUC ~32% (P-gp induction?)
- Levothyroxine → ↓ linezolid concentrations
- Clarithromycin → ↑ linezolid AUC >3-fold
- Amlodipine, amiodarone, omeprazole, warfarin → linezolid overexposure reports
- Linezolid likely a P-glycoprotein substrate
Pharmacology — tedizolid
Tedizolid — the prodrug story
- Tedizolid phosphate → cleaved by plasma phosphatases → active tedizolid
- Bioavailability ~91% — no dose adjustment IV vs. PO
- 200 mg once daily PO or IV (adults and pediatric ≥ 12 y)
- Half-life ~12 hours supports once-daily dosing
- Oral product taken without regard to meals
Tedizolid — distribution and metabolism
- Plasma protein binding 70–90% (free fraction ≈ linezolid)
- ELF AUC : plasma AUC = 40 and AM : plasma = 20 → high lung penetration
- Hepatic metabolism → sulfate conjugate in feces; <3% unchanged in urine
- No dose adjustment for hepatic, renal, dialysis, or obesity (BMI >30)
Tedizolid — special PK/PD caveats
- Free AUC/MIC ratio best predicts efficacy in murine models
- Markedly reduced antistaphylococcal activity in granulocytopenic mice — concerning signal
- Less pronounced effect in S. pneumoniae lung models
- Product label cautions against use in neutropenic patients — sparse human data
Tedizolid — drug interactions
- Negligible CYP450 interaction
- Inhibits intestinal BCRP → ↑ serum levels of rosuvastatin, methotrexate
- Weak, reversible MAOI activity in vitro — less risk than linezolid but not zero
- Four post-marketing serotonin syndrome reports to FAERS
Clinical use
FDA-approved indications — linezolid
- Nosocomial pneumonia (MRSA/MSSA, S. pneumoniae)
- Community-acquired pneumonia (S. pneumoniae including bacteremic; MSSA)
- Complicated SSTI (including diabetic foot, without osteomyelitis)
- Uncomplicated SSTI (MSSA, S. pyogenes)
- VRE E. faecium infections (including bacteremia)
FDA-approved indications — tedizolid
- Acute bacterial skin and skin-structure infection (ABSSSI) in adults and pediatric patients ≥ 12 years
- Susceptible Gram-positive pathogens:
- S. aureus (MRSA/MSSA), S. pyogenes, S. agalactiae, S. anginosus group, E. faecalis
MRSA SSTI — linezolid vs vancomycin
- Cochrane review (9 RCTs): linezolid superior to vancomycin for clinical and microbiologic cure; shorter LOS, lower cost
- Superiority observed in adults but not in <18 y
- Recent network meta-analysis: linezolid superior to vancomycin; comparable to dapto, ceftaroline, telavancin, tigecycline, tedizolid
MRSA nosocomial pneumonia — the Wunderink saga
- Pooled analysis of 2 RCTs (Wunderink 2003): linezolid + aztreonam ≈ vanc + aztreonam overall; subgroup analysis suggested superior survival in MRSA
- Subgroup analysis criticized by FDA (Powers, 2004)
- Subsequent ZEPHyR trial (Wunderink 2012): higher clinical success with linezolid, no 60-day mortality difference; questioned by under-dosed vancomycin arm
MRSA pneumonia — meta-analytic verdict
- Pooled RCT data: no difference in clinical or microbiologic efficacy or all-cause mortality
- Nephrotoxicity higher with vancomycin — robust signal
- Practical message: either is acceptable; choose by toxicity profile, route, and TDM feasibility
S. aureus bacteremia — linezolid’s evolving role
- Effective for MSSA and MRSA bacteremia in selected patients
- Persistent bacteremia, vancomycin failure, salvage scenarios
- Static vs. cidal concerns no longer hold up
- Oral step-down to linezolid as effective as exclusive parenteral therapy in propensity-matched cohorts (mostly uncomplicated bacteremia)
POET — oral step-down for left-sided IE
- 400 adults with stable left-sided IE (Strep, E. faecalis, S. aureus, CoNS)
- ≥ 10 days IV therapy → randomized to continued IV vs. oral switch
- 6-month composite (death, surgery, embolism, relapse): 9.0% PO vs. 12.1% IV — noninferior
- MRSA IE not evaluated — do not extrapolate
- Guidelines still do not list linezolid for MRSA endocarditis
Coagulase-negative staphylococci
- Case series support linezolid for bone/joint, meningitis, VP-shunt, and endocarditis with prosthetic material
- Insufficient data to recommend linezolid as routine first-line
- CoNS endocarditis: small subset in POET treated successfully with oral step-down
Vancomycin-resistant enterococci
- Multiple meta-analyses comparing linezolid vs. daptomycin for VRE bacteremia
- Early data favored linezolid (low daptomycin doses limited interpretation)
- More recent 22-study meta-analysis: nonsignificant ↑ mortality with daptomycin; no difference in microbiologic cure or recurrence
- VA cohort (Britt 2015): daptomycin better clinical success and 30-day mortality even at relatively low doses
- Choice should be individualized — susceptibility, exposure history, source, comorbidities
VRE endocarditis
- Both linezolid and daptomycin are recommended for enterococcal IE resistant to penicillin, aminoglycosides, vancomycin
- Evidence base limited — small numbers, treatment success and failure described
- Animal data suggest possible synergy with gentamicin, doxycycline, ceftriaxone, daptomycin; clinical use of combinations unproven
Streptococci including S. pneumoniae
- Effective for CAP caused by S. pneumoniae in open-label RCTs
- Not first-line empirical CAP — poor H. influenzae and atypical coverage
- Case reports support pneumococcal CNS infection use, usually with ceftriaxone
- Group A streptococcal necrotizing soft-tissue infection / toxic shock: considered as a clindamycin substitute (also inhibits exotoxin production)
- 2023 focused debate: linezolid is a reasonable alternative when clindamycin is contraindicated, resistant, or in short supply
Tedizolid — ESTABLISH-1 and -2
- Two non-inferiority Phase III trials in ABSSSI
- Tedizolid 200 mg × 6 days vs linezolid 600 mg BID × 10 days
- S. aureus most common pathogen; MRSA in 27–42%
- Both trials: non-inferior at 48–72 h and end of therapy
- Less GI toxicity and less thrombocytopenia with tedizolid
Tedizolid — beyond skin
- Phase III RCT (pediatric ≥ 12 y) for ABSSSI: comparable efficacy and safety
- Phase III HAP/VAP trial (Wunderink 2021): non-inferior day-28 mortality vs linezolid; failed non-inferiority for investigator-assessed clinical response — reason unclear
- Network meta-analysis: tedizolid clinical response superior to vancomycin, comparable to linezolid, dapto, ceftaroline, telavancin, teicoplanin, tigecycline
Linezolid in MDR/XDR-TB — the modern role
- Linezolid is now central to drug-resistant TB regimens
- BPaL regimen (bedaquiline + pretomanid + linezolid 1200 mg/day, 6 mo): ~90% favorable outcomes in highly drug-resistant TB
- WHO 2022: BPaL endorsed for 6–9 months in MDR/RR-TB
- BUT: >80% experienced toxicity at 1200 mg/day (neuropathy, myelosuppression)
ZeNix — getting the dose right
- 2×2 factorial: linezolid 1200 vs 600 mg/day and 26 vs 9 weeks within BPaL
- 600 mg/day × 26 weeks: favorable outcome 91% (vs 94% with 1200 mg)
- Substantially less neuropathy and myelosuppression at the lower dose
- Modeling: 600 mg/day balances efficacy and AE risk
- Bottom line: 600 mg/day × 26 weeks is the preferred dose
Nocardia — linezolid’s place
- Near-universal susceptibility, oral bioavailability, CNS penetration → attractive option
- Combination induction therapy for disseminated, cutaneous, or moderate-severe pulmonary disease
- Often with TMP-SMX + ceftriaxone; alternative when amikacin or TMP-SMX toxicity limits use
- 1-year survival ~85% — comparable to other regimens
- Main toxicity = thrombocytopenia
Oral vs. intravenous
- Bioavailability ≈ 100% (linezolid) and ~91% (tedizolid) → oral substitutes for IV when clinically appropriate
- Use oral when:
- Patient clinically stable and reliable
- GI absorption intact
- Indication has supporting peer-reviewed evidence
- Strong stewardship argument — earlier discharge, lower cost
Adverse effects
Overall tolerability
- Both agents generally well tolerated
- Common AEs (more frequent with linezolid):
- Headache, nausea, vomiting, diarrhea
- Serious AEs are uncommon but dose- and duration-dependent
Hematologic toxicity — the headline AE
- Reversible myelosuppression: thrombocytopenia >> anemia, pancytopenia, pure red cell aplasia
- Phase III data: thrombocytopenia in 2.4% of adults (range 0.3–10%)
- Risk factors: prolonged duration, renal insufficiency, hepatic impairment, baseline marrow suppression
- Mechanism: drug-induced immune-mediated and progenitor suppression
Hematologic toxicity — monitoring
- Weekly CBC if therapy ≥ 2 weeks (per label)
- TDM useful: trough >7.5–22.1 mg/L associated with hematologic toxicity
- Tedizolid: thrombocytopenia 2.1% (6 d) vs 3.8% linezolid (10 d) in pooled ABSSSI data
- Long-term tedizolid (median 28 d): 6/81 thrombocytopenia — uncommon, often clinically tolerable
Monoamine oxidase inhibition
- Linezolid: reversible, nonselective MAO inhibitor
- Serotonin syndrome with concurrent serotonergic agents
- Highest-risk co-medications in FAERS: citalopram, escitalopram, methadone
- Overall a rare event — risk/benefit reasonable in many patients
- Tedizolid: weak in vitro MAOI; only 4 FAERS reports — risk likely lower but not zero
Tyramine and adrenergic interactions
- Modest ↑ systolic BP with concurrent tyramine → label dietary cautions
- Blood pressure monitoring recommended with concurrent adrenergic agents or hypertension
- Practical: review SSRI/SNRI/MAOI co-medications before starting linezolid
Mitochondrial toxicity — unifying concept
- Disruption of mitochondrial protein synthesis explains:
- Peripheral and optic neuropathy
- Lactic acidosis
- Possibly rhabdomyolysis and drug-induced liver injury
- Tedizolid is theoretically a more potent mitochondrial inhibitor — but lower free exposure and a recovery window each dosing interval may reduce in vivo risk
Neuropathy
- Peripheral neuropathy: distal dysesthesias, often poorly reversible — prolonged therapy
- Optic neuropathy: gradual visual blurring; visual loss can be permanent if drug not stopped — reversible if caught early
- Phase III data: peripheral/optic neuropathy similar between tedizolid (6 d) and linezolid (10 d) — short courses
- Watch for it in prolonged TB or osteomyelitis courses — French MDR-TB cohort: high neurologic AE burden
Lactic acidosis
- Rare but including fatal cases
- Most often during prolonged therapy — but can develop within the first week
- Prompt recognition and drug discontinuation are critical
- Risk increased: age, renal insufficiency, drug interactions causing overexposure
- Possible genetic predisposition (mitochondrial ribosome polymorphisms)
- Tedizolid lactic acidosis reported to FAERS — causality less clear
Miscellaneous and rare AEs
- Increased mortality when used as monotherapy for catheter-related infections with Gram-negative or mixed flora
- Hyponatremia / SIADH, PRES, seizures
- Tooth and tongue discoloration, black hairy tongue
- Hypoglycemia in diabetic patients on insulin or oral hypoglycemics
- Oral suspension contains phenylalanine — caution in PKU
Pipeline
Investigational oxazolidinones
- Radezolid — broader Gram-positive activity, including LZD-R strains
- Sutezolid — structurally similar to linezolid; potent anti-mycobacterial activity
- Delpazolid — Gram-positive activity similar to linezolid; superior in vitro vs mycobacteria
- Contezolid (MRX-I) — activity vs MRSA, VRE, mycobacteria; approved in China for ABSSSI
Take-home points
Five things to remember
Two FDA agents — linezolid (BID, 100% bioavail), tedizolid (QD prodrug, retains activity vs many cfr strains)
Bind 23S rRNA / PTC — no cross-resistance with β-lactams, glyco, dapto, Q-D
Resistance is rare but rising — 23S mutations, L3/L4, cfr, optrA/poxtA
TDM when prolonged, renal failure, or critically ill — trough 2–7 mg/L for Gram-positive infection
Toxicity profile drives long-term decisions — myelosuppression, neuropathy, lactic acidosis, serotonin syndrome
References
Aono A, Murase Y, Chikamatsu K, et al. In vitro activity of tedizolid and linezolid against multidrug-resistant Mycobacterium tuberculosis: A comparative study using microdilution broth assay and genomics. Diagnostic Microbiology and Infectious Disease 2022;103:115714. https://doi.org/10.1016/j.diagmicrobio.2022.115714.
Baddour LM, Wilson WR, Bayer AS, et al. Infective endocarditis in adults: Diagnosis, antimicrobial therapy, and management of complications: A scientific statement for healthcare professionals from the American Heart Association. Circulation 2015;132:1435–86. https://doi.org/10.1161/CIR.0000000000000296.
Bender JK, Cattoir V, Hegstad K, et al. Update on prevalence and mechanisms of resistance to linezolid, tigecycline, and daptomycin in enterococci in Europe: Towards a common nomenclature. Drug Resistance Updates 2018;40:25–39. https://doi.org/10.1016/j.drup.2018.10.002.
Bernstein WB, Trotta RF, Rector JT, et al. Mechanisms for linezolid-induced anemia and thrombocytopenia. Annals of Pharmacotherapy 2003;37:517–20. https://doi.org/10.1345/aph.1C361.
Biedenbach DJ, Jones RN. In vitro activity of linezolid (U-100766) against Haemophilus influenzae measured by three different susceptibility testing methods. Diagnostic Microbiology and Infectious Disease 2001;39:49–53. https://doi.org/10.1016/s0732-8893(00)00216-1.
Birmingham MC, Rayner CR, Meagher AK, et al. Linezolid for the treatment of multidrug-resistant, gram-positive infections: Experience from a compassionate-use program. Clinical Infectious Diseases 2003;36:159–68. https://doi.org/10.1086/345744.
Bolhuis M, Altena R van, Uges DR, et al. Clarithromycin significantly increases linezolid serum concentrations. Antimicrobial Agents and Chemotherapy 2010;54:5418–9. https://doi.org/10.1128/AAC.00757-10.
Bonilla H, Huband MD, Seidel J, et al. Multicity outbreak of linezolid-resistant Staphylococcus epidermidis associated with clonal spread of a cfr-containing strain. Clinical Infectious Diseases 2010;51:796–800. https://doi.org/10.1086/656281.
Brenciani A, Morroni G, Schwarz S, et al. Oxazolidinones: Mechanisms of resistance and mobile genetic elements involved. Journal of Antimicrobial Chemotherapy 2022;77:2596–621. https://doi.org/10.1093/jac/dkac263.
Britt NS, Potter EM, Patel N, et al. Comparison of the effectiveness and safety of linezolid and daptomycin in vancomycin-resistant enterococcal bloodstream infection: A national cohort study of Veterans Affairs patients. Clinical Infectious Diseases 2015;61:871–8. https://doi.org/10.1093/cid/civ444.
Brown-Elliott BA, Wallace Jr R. J. In vitro susceptibility testing of tedizolid against isolates of Nocardia. Antimicrobial Agents and Chemotherapy 2017;61:e01537–17. https://doi.org/10.1128/AAC.01537-17.
Carvalhaes CG, Sader HS, Streit JM, et al. Five-year analysis of the in vitro activity of tedizolid against a worldwide collection of indicated species causing clinical infections: Results from the surveillance of tedizolid activity and resistance (STAR) programme. JAC-Antimicrobial Resistance 2022;4:dlac088. https://doi.org/10.1093/jacamr/dlac088.
Chuang YC, Wang JT, Lin HY, et al. Daptomycin versus linezolid for treatment of vancomycin-resistant enterococcal bacteremia: Systematic review and meta-analysis. BMC Infectious Diseases 2014;14:687–97. https://doi.org/10.1186/s12879-014-0687-9.
Clinical and Laboratory Standards Institute. Performance standards for antimicrobial susceptibility testing 2022.
Colca JR, McDonald WG, Waldon DJ, et al. Cross-linking in the living cell locates the site of action of oxazolidinone antibiotics. Journal of Biological Chemistry 2003;278:21972–9. https://doi.org/10.1074/jbc.M302109200.
Conradie F, Bagdasaryan TR, Borisov S, et al. Bedaquiline-pretomanid-linezolid regimens for drug-resistant tuberculosis (ZeNix). New England Journal of Medicine 2022;387:810–23. https://doi.org/10.1056/NEJMoa2119430.
Conradie F, Diacon AH, Ngubane N, et al. Treatment of highly drug-resistant pulmonary tuberculosis (Nix-TB). New England Journal of Medicine 2020;382:893–902. https://doi.org/10.1056/NEJMoa1901814.
Cortes-Penfield N, Ryder JH. Should linezolid replace clindamycin as the adjunctive antimicrobial of choice in group A streptococcal necrotizing soft tissue infection and toxic shock syndrome? A focused debate. Clinical Infectious Diseases 2023;76:346–50. https://doi.org/10.1093/cid/ciac720.
De Vriese AS, Van Coster R, Smet J, et al. Linezolid-induced inhibition of mitochondrial protein synthesis. Clinical Infectious Diseases 2006;42:1111–7. https://doi.org/10.1086/501356.
Diaz L, Kiratisin P, Mendes RE, et al. Transferable plasmid-mediated resistance to linezolid due to cfr in a human clinical isolate of Enterococcus faecalis. Antimicrobial Agents and Chemotherapy 2012;56:3917–22. https://doi.org/10.1128/AAC.00419-12.
Drusano GL, Liu W, Kulawy R, et al. Impact of granulocytes on the antimicrobial effect of tedizolid in a mouse thigh infection model. Antimicrobial Agents and Chemotherapy 2011;55:5300–5. https://doi.org/10.1128/AAC.00502-11.
European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters, version 12.0 2022.
Feng J, Xiang F, Cheng J, et al. Comparative efficacy and safety of vancomycin, linezolid, tedizolid, and daptomycin in treating patients with suspected or proved complicated skin and soft tissue infections: An updated network meta-analysis. Infectious Diseases and Therapy 2021;10:1531–47. https://doi.org/10.1007/s40121-021-00456-0.
Flanagan S, McKee EE, Das D, et al. Nonclinical and pharmacokinetic assessments to evaluate the potential of tedizolid and linezolid to affect mitochondrial function. Antimicrobial Agents and Chemotherapy 2015;59:178–85. https://doi.org/10.1128/AAC.03684-14.
Foti C, Piperno A, Scala A, et al. Oxazolidinone antibiotics: Chemical, biological, and analytical aspects. Molecules 2021;26:4280. https://doi.org/10.3390/molecules26144280.
Gandelman K, Zhu T, Fahmi OA, et al. Unexpected effect of rifampin on the pharmacokinetics of linezolid: In silico and in vitro approaches to explain its mechanism. Journal of Clinical Pharmacology 2011;51:229–36. https://doi.org/10.1177/0091270010366445.
Gatti M, Raschi E, De Ponti F. Serotonin syndrome by drug interactions with linezolid: Clues from pharmacovigilance-pharmacokinetic/pharmacodynamics analysis. European Journal of Clinical Pharmacology 2021;77:233–9. https://doi.org/10.1007/s00228-020-02990-1.
Gerson SL, Kaplan SL, Bruss JB, et al. Hematologic effects of linezolid: Summary of clinical experience. Antimicrobial Agents and Chemotherapy 2002;46:2723–6. https://doi.org/10.1128/AAC.46.8.2723-2726.2002.
Goldstein EJ, Citron DM, Merriam CV. Linezolid activity compared to those of selected macrolides and other agents against aerobic and anaerobic pathogens isolated from soft tissue bite infections in humans. Antimicrobial Agents and Chemotherapy 1999;43:1469–74. https://doi.org/10.1128/AAC.43.6.1469.
Hölzel CS, Harms KS, Schwaiger K, et al. Resistance to linezolid in a porcine Clostridium perfringens strain carrying a mutation in the rplD gene encoding the ribosomal protein L4. Antimicrobial Agents and Chemotherapy 2010;54:1351–3. https://doi.org/10.1128/AAC.01208-09.
Imperial MZ, Nedelman JR, Conradie F, et al. Proposed linezolid dosing strategies to minimize adverse events for treatment of extensively drug-resistant tuberculosis. Clinical Infectious Diseases 2022;74:1736–47. https://doi.org/10.1093/cid/ciab699.
Iqbal K, Milioudi A, Wicha SG. Pharmacokinetics and pharmacodynamics of tedizolid. Clinical Pharmacokinetics 2022;61:489–503. https://doi.org/10.1007/s40262-021-01099-7.
Iversen K, Ihlemann N, Gill SU, et al. Partial oral versus intravenous antibiotic treatment of endocarditis. New England Journal of Medicine 2019;380:415–24. https://doi.org/10.1056/NEJMoa1808312.
Jang HC, Kim S-H, Kim KH, et al. Salvage treatment for persistent methicillin-resistant Staphylococcus aureus bacteremia: Efficacy of linezolid with or without carbapenem. Clinical Infectious Diseases 2009;49:395–401. https://doi.org/10.1086/600295.
Jaspard M, Butel N, El Helali N, et al. Linezolid-associated neurologic adverse effects in patients with multidrug-resistant tuberculosis, France. Emerging Infectious Diseases 2020;26:1792–800. https://doi.org/10.3201/eid2608.191499.
Kalil AC, Klompas M, Haynatzki G, et al. Treatment of hospital-acquired pneumonia with linezolid or vancomycin: A systematic review and meta-analysis. BMJ Open 2013;3:e003912. https://doi.org/10.1136/bmjopen-2013-003912.
Larruskain J, Idigoras P, Marimón JM, et al. Susceptibility of 186 Nocardia sp. Isolates to 20 antimicrobial agents. Antimicrobial Agents and Chemotherapy 2011;55:2995–8. https://doi.org/10.1128/AAC.01279-10.
Locke JB, Finn J, Hilgers M, et al. Structure-activity relationships of diverse oxazolidinones for linezolid-resistant Staphylococcus aureus strains possessing the cfr methyltransferase gene or ribosomal mutations. Antimicrobial Agents and Chemotherapy 2010;54:5337–43. https://doi.org/10.1128/AAC.00663-10.
Long KS, Vester B. Resistance to linezolid caused by modifications at its binding site on the ribosome. Antimicrobial Agents and Chemotherapy 2012;56:603–12. https://doi.org/10.1128/AAC.05702-11.
Luque S, Grau S, Alvarez-Lerma F, et al. Plasma and cerebrospinal fluid concentrations of linezolid in neurosurgical critically ill patients with proven or suspected central nervous system infections. International Journal of Antimicrobial Agents 2014;44:409–15. https://doi.org/10.1016/j.ijantimicag.2014.07.001.
Mendes RE, Deshpande L, Streit JM, et al. ZAAPS programme results for 2016: An activity and spectrum analysis of linezolid using clinical isolates from medical centres in 42 countries. Journal of Antimicrobial Chemotherapy 2018;73:1880–7. https://doi.org/10.1093/jac/dky099.
Merck & Co., Inc. Sivextro® (tedizolid) [Package Insert] 2021.
Mirzayev F, Viney K, Linh NN, et al. World Health Organization recommendations on the treatment of drug-resistant tuberculosis, 2020 update. European Respiratory Journal 2021;57:2003300. https://doi.org/10.1183/13993003.03300-2020.
Moellering RC. Linezolid: The first oxazolidinone antimicrobial. Annals of Internal Medicine 2003;138:135–42. https://doi.org/10.7326/0003-4819-138-2-200301210-00015.
Moran GJ, Fang E, Corey GR, et al. Tedizolid for 6 days versus linezolid for 10 days for acute bacterial skin and skin-structure infections (ESTABLISH-2): A randomised, double-blind, phase 3, non-inferiority trial. The Lancet Infectious Diseases 2014;14:696–705. https://doi.org/10.1016/S1473-3099(14)70737-6.
Narita M, Tsuji BT, Yu VL. Linezolid-associated peripheral and optic neuropathy, lactic acidosis, and serotonin syndrome. Pharmacotherapy 2007;27:1189–97. https://doi.org/10.1592/phco.27.8.1189.
Obach RS. Linezolid metabolism is catalyzed by cytochrome P450 2J2, 4F2, and 1B1. Drug Metabolism and Disposition 2022;50:413–21. https://doi.org/10.1124/dmd.121.000776.
Pea F, Viale P, Cojutti P, et al. Therapeutic drug monitoring may improve safety outcomes of long-term treatment with linezolid in adult patients. Journal of Antimicrobial Chemotherapy 2012;67:2034–42. https://doi.org/10.1093/jac/dks153.
Pharmacia and Upjohn Company. Zyvox® (linezolid) [Package Insert] 2021.
Pogue JM, Paterson DL, Pasculle W, et al. Determination of risk factors associated with isolation of linezolid-resistant strains of vancomycin-resistant Enterococcus. Infection Control and Hospital Epidemiology 2007;28:1382–8. https://doi.org/10.1086/523276.
Prokocimer P, De Anda C, Fang E, et al. Tedizolid phosphate vs linezolid for treatment of acute bacterial skin and skin structure infections: The ESTABLISH-1 randomized trial. JAMA 2013;309:559–69. https://doi.org/10.1001/jama.2013.241.
Rao GG, Konicki R, Cattaneo D, et al. Therapeutic drug monitoring can improve linezolid dosing regimens in current clinical practice: A review of linezolid pharmacokinetics and pharmacodynamics. Therapeutic Drug Monitoring 2020;42:83–92. https://doi.org/10.1097/FTD.0000000000000710.
Roger C, Roberts JA, Muller L. Clinical pharmacokinetics and pharmacodynamics of oxazolidinones. Clinical Pharmacokinetics 2018;57:559–75. https://doi.org/10.1007/s40262-017-0601-x.
Rybak JM, Roberts K. Tedizolid phosphate: A next-generation oxazolidinone. Infectious Diseases and Therapy 2015;4:1–14. https://doi.org/10.1007/s40121-015-0060-3.
Santini A, Ronchi D, Garbellini M, et al. Linezolid-induced lactic acidosis: The thin line between bacterial and mitochondrial ribosomes. Expert Opinion on Drug Safety 2017;16:833–43. https://doi.org/10.1080/14740338.2017.1335305.
Shoen C, DeStefano M, Hafkin B, et al. In vitro and in vivo activities of contezolid (MRX-I) against Mycobacterium tuberculosis. Antimicrobial Agents and Chemotherapy 2018;62:e00493–18. https://doi.org/10.1128/AAC.00493-18.
Slee AM, Wuonola MA, McRipley RJ, et al. Oxazolidinones, a new class of synthetic antibacterial agents: In vitro and in vivo activities of DuP 105 and DuP 721. Antimicrobial Agents and Chemotherapy 1987;31:1791–7. https://doi.org/10.1128/AAC.31.11.1791.
Stevens DL, Bisno AL, Chambers HF, et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clinical Infectious Diseases 2014;59:e10–52. https://doi.org/10.1093/cid/ciu444.
Traver EC, Heil EL, Schmalzle SA. A cross-sectional analysis of linezolid in combination with methadone or buprenorphine as a cause of serotonin toxicity. Open Forum Infectious Diseases 2022;9:ofac331. https://doi.org/10.1093/ofid/ofac331.
Villani P, Regazzi MG, Marubbi F, et al. Cerebrospinal fluid linezolid concentrations in postneurosurgical central nervous system infections. Antimicrobial Agents and Chemotherapy 2002;46:936–7. https://doi.org/10.1128/AAC.46.3.936-937.2002.
Viswanathan P, Iarikov D, Wassel R, et al. Hypoglycemia in patients treated with linezolid. Clinical Infectious Diseases 2014;59:e93–5. https://doi.org/10.1093/cid/ciu487.
Wald-Dickler N, Holtom P, Spellberg B. Busting the myth of “static vs cidal”: A systematic literature review. Clinical Infectious Diseases 2018;66:1470–4. https://doi.org/10.1093/cid/cix1127.
Wang S, Cai C, Shen Y, et al. In vitro activity of contezolid against methicillin-resistant Staphylococcus aureus, vancomycin-resistant Enterococcus, and strains with linezolid resistance genes from china. Frontiers in Microbiology 2021;12:729900. https://doi.org/10.3389/fmicb.2021.729900.
Wang Y, Lv Y, Cai J, et al. A novel gene, optrA, that confers transferable resistance to oxazolidinones and phenicols and its presence in Enterococcus faecalis and Enterococcus faecium of human and animal origin. Journal of Antimicrobial Chemotherapy 2015;70:2182–90. https://doi.org/10.1093/jac/dkv116.
Wilcox MH, Tack KJ, Bouza E, et al. Complicated skin and skin-structure infections and catheter-related bloodstream infections: Noninferiority of linezolid in a phase 3 study. Clinical Infectious Diseases 2009;48:203–12. https://doi.org/10.1086/595686.
Willekens R, Puig-Asensio M, Ruiz-Camps I, et al. Early oral switch to linezolid for low-risk patients with Staphylococcus aureus bloodstream infections: A propensity-matched cohort study. Clinical Infectious Diseases 2019;69:381–7. https://doi.org/10.1093/cid/ciy916.
Wunderink RG, Niederman MS, Kollef MH, et al. Linezolid in methicillin-resistant Staphylococcus aureus nosocomial pneumonia: A randomized, controlled study. Clinical Infectious Diseases 2012;54:621–9. https://doi.org/10.1093/cid/cir895.
Wunderink RG, Rello J, Cammarata SK, et al. Linezolid vs vancomycin: Analysis of two double-blind studies of patients with methicillin-resistant Staphylococcus aureus nosocomial pneumonia. Chest 2003;124:1789–97. https://doi.org/10.1378/chest.124.5.1789.
Wunderink RG, Roquilly A, Croce M, et al. A phase 3 randomized, double-blind study comparing tedizolid phosphate and linezolid for treatment of ventilated gram-positive hospital-acquired or ventilator-associated bacterial pneumonia. Clinical Infectious Diseases 2021;73:e710–8. https://doi.org/10.1093/cid/ciab032.
Xiao J, Gill C, Liang L, et al. Use of translational pharmacokinetic/pharmacodynamic infection models to understand the impact of neutropenia on the efficacy of tedizolid phosphate. Antimicrobial Agents and Chemotherapy 2019;63:e00822–18. https://doi.org/10.1128/AAC.00822-18.
Yang C, Lei H, Wang D, et al. In vitro activity of linezolid against clinical isolates of Mycobacterium tuberculosis, including multidrug-resistant and extensively drug-resistant strains from beijing, china. Japanese Journal of Infectious Diseases 2012;65:240–2. https://doi.org/10.7883/yoken.65.240.
Yeager SD, Oliver JE, Shorman MA, et al. Comparison of linezolid step-down therapy to standard parenteral therapy in methicillin-resistant Staphylococcus aureus bloodstream infections. International Journal of Antimicrobial Agents 2021;57:106329. https://doi.org/10.1016/j.ijantimicag.2021.106329.
Yue J, Dong BR, Yang M, et al. Linezolid versus vancomycin for skin and soft tissue infections. Cochrane Database of Systematic Reviews 2016:1–42. https://doi.org/10.1002/14651858.CD008056.pub3.