Antibiotics in Advanced Development
2026-05-19
Antibiotics for MDR Pathogens in Advanced Stages
of Clinical Development
Russell E. Lewis, Pharm.D., FCCP
Associate Professor of Infectious Diseases

russelledward.lewis@unipd.it
Slides and course materials: www.idpadovaid.com
Part 1: The AMR Crisis
and Priority Pathogens
Antibiotic development vs. resistance

The antimicrobial resistance crisis
Current impact:
- 700,000 deaths annually attributed to AMR
- MDR organisms have limited treatment options
- Resistance detected after every new antibiotic introduction
Projected impact:
- 10 million deaths/year by 2050 if unchecked
- Economic burden estimated at $100 trillion
Legislative efforts:
The GAIN Act (2012) in US and Italian Progress
Generating Antibiotic Incentives Now Act (2010-2020) provided “push incentives” →17 new systemic antibiotics approved, including agents targeting CRE and MRSA
| Incentive | Mechanism |
|---|---|
| Extended exclusivity | Additional 5 years market protection |
| Fast track designation | Accelerated development pathway |
| Priority review | 6-month vs. 10-month FDA review |
Push incentives– Attempted to delink company revenue from antibiotic sales volume, thereby encouraging development of new antimicrobials-i.e. Netflix models
Italy (Legge di Bilancio 2025) Article 49 - allowed certain WHO AWaRe “Reserve” antibiotics targeting multidrug-resistant organisms to access the national Innovative Medicines Fund
Created access to up to €100 million annually for qualifying reserve antibiotics- privileged reimbursement and protection from hospital budget disincentives
Linked reimbursement to therapeutic innovativeness and stewardship monitoring
The Plazomicin case study: A cautionary tale

Timeline:
- FDA approval obtained for new aminoglycoside targeting resistant gram-negatives
- Drug reserved as “last resort” therapy (appropriate stewardship)
- Low sales volume due to targeted use
- Company could not sustain itself financially
- The lesson: Push incentives support development but fail to ensure post-approval sustainability
- New focus: Pull incentives (subscription models) that reward societal value rather than sales volume
WHO Priority Pathogens List (2024 Update)
Assessment criteria (MCDA framework):
- Mortality & non-fatal burden
- Incidence & 10-year resistance trends
- Transmissibility & preventability
- Treatability & antibacterial pipeline
Key changes from 2017:
- Rifampicin-resistant M. tuberculosis added to critical tier
- Salmonella Typhi & Shigella spp. elevated to high priority
- P. aeruginosa reclassified from critical → high
- H. pylori, Campylobacter spp. removed
Critical priority pathogens
| Pathogen | Resistance pattern |
|---|---|
| Acinetobacter baumannii | Carbapenem-resistant (CRAB) |
| Enterobacterales (K. pneumoniae, E. coli, others) | Carbapenem-resistant (CRE) |
| Enterobacterales (K. pneumoniae, E. coli, others) | 3rd-generation cephalosporin-resistant (ESBL) |
| Mycobacterium tuberculosis | Rifampicin-resistant |
Novel agents covered in this lecture: Sulbactam-durlobactam (CRAB), multiple BL/BLI combinations & oral carbapenems (CRE/ESBL)
High priority pathogens
| Pathogen | Resistance pattern |
|---|---|
| Salmonella enterica serotype Typhi | Fluoroquinolone-resistant |
| Shigella spp. | Fluoroquinolone-resistant |
| Enterococcus faecium | Vancomycin-resistant (VRE) |
| Pseudomonas aeruginosa | Carbapenem-resistant |
| Non-typhoidal Salmonella | Fluoroquinolone-resistant |
| Neisseria gonorrhoeae | 3rd-gen cephalosporin- and/or FQ-resistant |
| Staphylococcus aureus | Methicillin-resistant (MRSA) |
Novel agents covered: Ceftobiprole (MRSA), Gepotidacin & Zoliflodacin (N. gonorrhoeae)
Medium priority pathogens
| Pathogen | Resistance pattern |
|---|---|
| Group A streptococci | Macrolide-resistant |
| Streptococcus pneumoniae | Macrolide-resistant |
| Haemophilus influenzae | Ampicillin-resistant |
| Group B streptococci | Penicillin-resistant |
These pathogens have a disproportionate impact on infants, young adults,
and older adults, especially in resource-limited settings.
β-Lactamase classification: Ambler system
| Class | Type | Examples | Inhibited by |
|---|---|---|---|
| A | Serine | KPC, CTX-M, TEM, SHV | Avibactam, Vaborbactam, Xeruborbactam |
| B | Metallo (MBL) | NDM, VIM, IMP | Aztreonam stability only; Xeruborbactam, Taniborbactam |
| C | Serine (AmpC) | AmpC | Avibactam, Xeruborbactam |
| D | Serine (OXA) | OXA-23, OXA-48 | Durlobactam, Avibactam (limited), Xeruborbactam |
Critical Point
Class B MBLs remain the greatest challenge - no approved inhibitor exists, but taniborbactam and xeruborbactam are in development
Novel β-Lactamase inhibitor classes
Diazabicyclooctanes (DBOs):
- Avibactam
- Relebactam
- Durlobactam (OXA activity!)
- Zidebactam
Mechanism: Covalent, reversible binding to serine β-lactamases
Boronates:
- Vaborbactam
- Taniborbactam (MBL activity!)
- Xeruborbactam (ultra-broad spectrum!)
Mechanism: Reversible binding, broader spectrum including some MBLs
Key Innovation
Taniborbactam and xeruborbactam are the first inhibitors with activity against Class B metallo-β-lactamases (NDM, VIM); xeruborbactam also inhibits IMP
Lecture roadmap: Agents we’ll cover
🔵 β-Lactam/BLI
- Sulbactam-Durlobactam
- Aztreonam-Avibactam
- Cefepime-Enmetazobactam
- Cefepime-Taniborbactam
- Cefepime-Zidebactam
- Meropenem-Xeruborbactam
🟡 Oral Carbapenems
- Tebipenem
- Sulopenem
🟣 Gram-Positive
- Ceftobiprole
- Contezolid
- Afabicin
🟢 Topoisomerase
- Gepotidacin
- Zoliflodacin
Part 2: β-Lactam/
β-Lactamase Inhibitor Combinations
Sulbactam-Durlobactam (Xacduro™)
FDA Approved: May 2023 for HABP/VABP due to A. baumannii-calcoaceticus complex. Not approved in Italy (yet) but can be requested by emergency authorization.
Sulbactam:
- Historically a β-lactamase inhibitor
- Intrinsic activity against A. baumannii
- Binds PBP 1a/1b and PBP3
- Limited by contemporary resistance by class A,C and D enzymes
Durlobactam:
- Novel DBO inhibitor
- Inhibits Class A, C, and D enzymes
- Unique OXA family activity
- Direct antibacterial activity via PBP2
Why This Matters
OXA-type carbapenemases (OXA-23, OXA-24/40) are the predominant resistance mechanism in A. baumannii worldwide
SUL-DUR: Mechanism of action
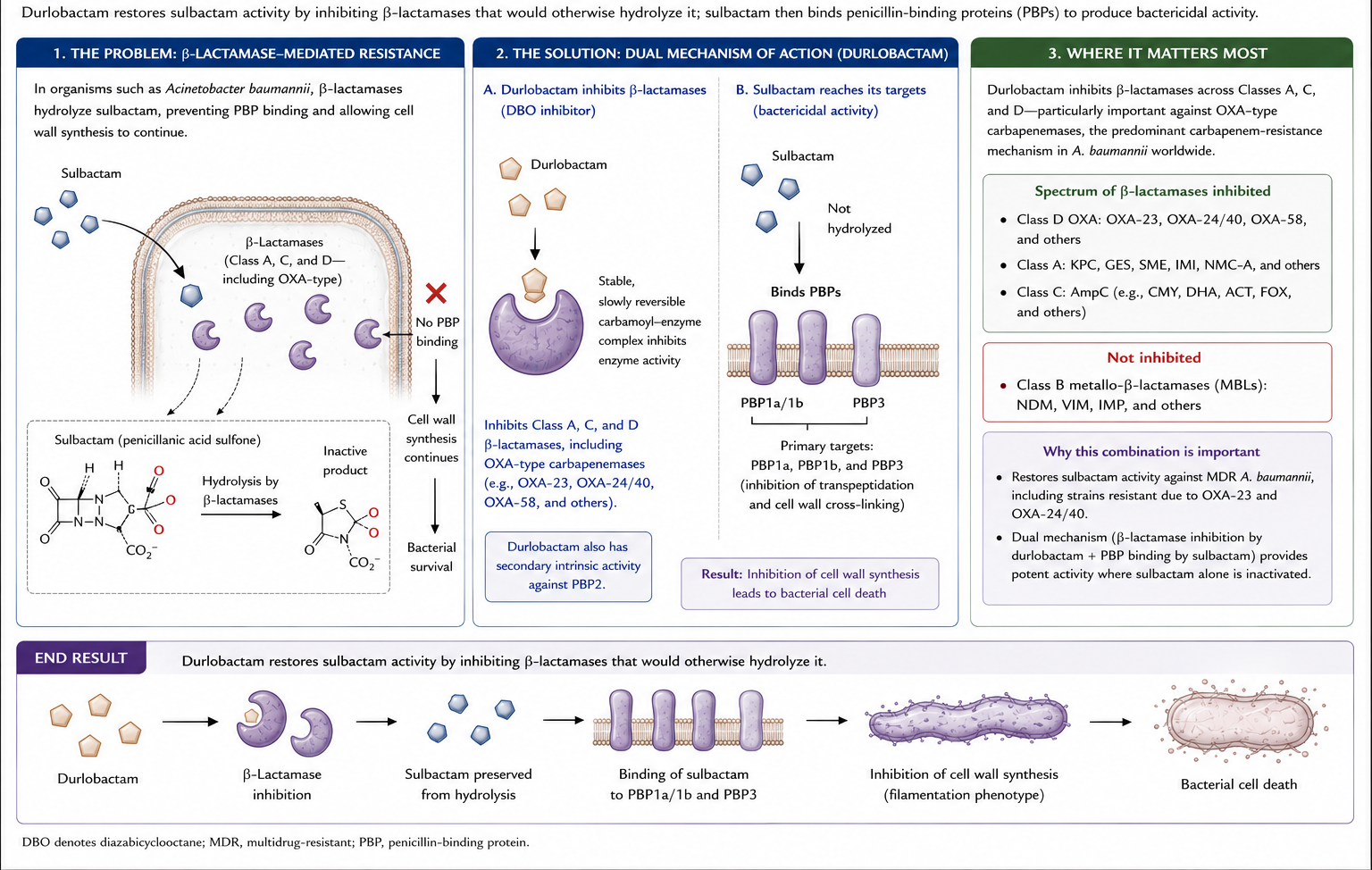
Result: Durlobactam restores sulbactam activity by inhibiting the β-lactamases that would otherwise hydrolyze it
SUL-DUR: In vitro activity
Global surveillance: 5,032 A. baumannii clinical isolates
| Agent | MIC50 | MIC90 |
|---|---|---|
| Sulbactam-Durlobactam | 1 mg/L | 2 mg/L |
| Sulbactam alone | 8 mg/L | 64 mg/L |
| Imipenem | >8 mg/L | >8 mg/L |
| Colistin | 1 mg/L | 2 mg/L |
Susceptibility breakpoint
FDA/CLSI susceptibility: ≤4/4 mg/L for SUL-DUR
32-fold reduction in MIC90 with durlobactam addition
SUL-DUR: Pharmacokinetics and dosing
Phase 1 PK data (healthy adults):
- Linear, dose-proportional pharmacokinetics
- Primary clearance: Renal excretion
- Half-life: 1.4–3.6 hours
- Minimal accumulation with multiple dosing
Recommended Dosing
Sulbactam-Durlobactam 2 g (1 g + 1 g)
- 3-hour IV infusion
- Every 6 hours
- Renal dose adjustment required for CrCl <90 mL/min
SUL-DUR: ATTACK trial design
Phase 3, Two-part registrational trial
Randomized, controlled comparison
- Population: HABP, VABP, BSI due to CRAB
- Intervention: SUL-DUR 2g (1g-1g) q6h over 3h
- Comparator: Colistin 2.5 mg/kg q12h over 30 min
- Background: Imipenem-cilastatin 1g-1g q6h (both arms)
- Primary endpoint: 28-day all-cause mortality
Supportive open-label study
- Patients with colistin-resistant A. baumannii
- Or polymyxin-intolerant patients
- Multiple infection types: HABP, VABP, BSI, cUTI, AP, wound infections
SUL-DUR: ATTACK trial results
Part A: m-MITT Population (n = 64 per arm)
| Outcome | SUL-DUR | Colistin | Difference |
|---|---|---|---|
| 28-day mortality | 19.0% | 32.3% | −13.2% |
| Clinical cure | 61.9% | 40.3% | +21.6% |
| Drug-related AEs | 12.3% | 30.2% | −17.9% |
| Nephrotoxicity (RIFLE) | 13.2% | 37.6% | −24.4%* |
*P = 0.0002
Key Finding
Noninferiority achieved with numerically better mortality, clinical cure, AND reduced nephrotoxicity
SUL-DUR: Clinical summary
Key points:
✓ First agent specifically developed for CRAB
✓ Novel OXA-family inhibition
✓ Mortality benefit suggested vs. colistin
✓ Significantly reduced nephrotoxicity
✓ FDA approved May 2023
Limitations:
- Limited to A. baumannii
- No activity against MBL-producers
- Requires IV administration
- Background imipenem in trials
Clinical Pearl
SUL-DUR represents a paradigm shift in CRAB treatment - from toxic colistin-based regimens to a more effective, safer β-lactam approach
Aztreonam-avibactam: The MBL solution
Under development for MDR gram-negative infections including MBL-producers
The problem:
- MBLs (NDM, VIM, IMP) hydrolyze all β-lactams
- No approved MBL inhibitor exists
- MBL-producers often co-produce serine β-lactamases
The solution:
- Aztreonam is intrinsically stable to MBLs
- Avibactam inhibits co-produced serine enzymes
- Combination restores aztreonam activity
ATM-AVI: In vitro activity
Enterobacterales surveillance (2019-2021): 27,834 isolates
| Population | ATM-AVI Susceptibility |
|---|---|
| All Enterobacterales | >99.9% at ≤8 mg/L |
| CRE (n = 261) | 99.6% |
| MBL-producers (n = 33) | 100% |
Important limitation
ATM-AVI has limited activity against P. aeruginosa including MBL-producing strains → it has limited ability to penetrate the outer membrane and is readily effluxed
MIC50/90: 0.25/0.5 mg/L for Enterobacterales
ATM-AVI: Dosing strategy
Based on Phase 1 PK-PD modeling:
Recommended Regimen
Loading dose: ATM-AVI 500-167 mg
Maintenance: ATM-AVI 1500-500 mg
- 3-hour IV infusion
- Every 6 hours
- Target: ƒT > MIC of 60% up to MIC 8 mg/L
Rationale for loading dose:
- Achieves steady-state exposure rapidly
- Critical for severe infections
- Compensates for renal clearance of both agents
ATM-AVI: Clinical development status
Open-label comparison in cIAI, HABP, VABP:
- ATM-AVI ± metronidazole vs. meropenem ± colistin
- Results support efficacy
| Indication | ATM-AVI Mortality | Comparator Mortality |
|---|---|---|
| cIAI | 1.9% (4/208) | 2.9% (3/104) |
| HABP/VABP | 10.8% (8/74) | 19.4% (7/36) |
MBL-producing infections specifically:
- Terminated early (15/60 planned patients enrolled)
- Enrollment extremely difficult
- TOC results: 5/12 (41.7%) ATM-AVI cured vs. 0/3 best available therapy
Current status
FDA approval in February 2025. Available in Italy but drug shortages in 2026 have limited supply.Considered a “critical-reserve” antibiotic
Cefepime-enmetazobactam (Exblifep®)
FDA approved: February 2024 for cUTI including acute pyelonephritis
Enmetazobactam:
- N-methyl derivative of tazobactam
- Net-neutral zwitterion
- Enhanced cell wall penetration
- Class A enzyme inhibition
Activity:
- CTX-M, TEM, SHV variants
- NOT serine carbapenemases (KPC)
- No advantages for P. aeruginosa
Target population:
| Target organisms | Proportion |
|---|---|
| ESBL-producers | ~70% |
| AmpC | ~20% |
| Other | ~10% |
Primarily ESBL-producing Enterobacterales
FEP-ENM: ALLIUM trial results
Phase 3, Randomized, Double-Blind Noninferiority Trial (cUTI/AP)
Primary Analysis (n = 678):
| Outcome | FEP-ENM | PIP-TAZ |
|---|---|---|
| Composite cure | 79.1% | 58.9% |
Δ = 21.2% (95% CI: 14.3-27.9%)
- Noninferiority achieved ✓
- Hierarchical superiority achieved ✓
ESBL Subset:
- FEP-ENM: 73.7%
- PIP-TAZ: 51.5%
Where FEP-ENM shines
Important
Not just noninferior - statistically superior to piperacillin-tazobactam
Cefepime-taniborbactam
In development for CRE and MBL-producing infections
Taniborbactam:
- Bicyclic boronate inhibitor
- Class A, C, D serine enzymes
- Class B MBL activity:
- VIM: Yes ✓
- Most NDM: Yes ✓
- IMP: Limited
- MDR P.aeruginosa PDC and PER-1/2
Dosing:
- 2.5 g (2 g + 500 mg)
- Every 8 hours
- 2-hour infusion
CERTAIN-1 Trial:
Phase 3 in cUTI/AP showed superiority to meropenem
Why this matters
If approved, FEP-TAN would be the first single agent effective against both serine carbapenemases AND most MBLs
Cefepime-zidebactam
In development for XDR gram-negative infections
Zidebactam - Unique mechanism:
β-Lactam Enhancer:
Inhibits class A and C ß-lactamases
Strong PBP2 binding
Complements cefepime’s PBP3, PBP1a/1b binding
Synergistic cell wall disruption
Spectrum:
- Enterobacterales (including CRE)
- XDR P. aeruginosa (including MBL) despite lack of activity against Class B enzymes
- A. baumannii complex
Dosing: 3 g (2 g + 1 g) q8h over 3 hours
Compassionate Use
Successful outcomes reported for NDM-producing P. aeruginosa infection
Meropenem-Xeruborbactam (MER-XER)
In development for CRE, MBL, and CRAB infections
Xeruborbactam:
- Tricyclic boronate inhibitor
- Ultra-broad spectrum BLI:
- Class A (KPC, CTX-M, TEM, SHV) ✓
- Class B MBLs (NDM, VIM, IMP) ✓
- Class C (AmpC) ✓
- Class D (OXA-23, OXA-48) ✓
- Broadest BLI spectrum in development
Dosing:
- 2-1 g q8h
- 3-hour infusion
- Renal dose adjustment required
Key Trials:
- Phase 3 in cUTI/AP and HABP/VABP
- Targets CRE, MBL-producers, and CRAB
Why this matters
MER-XER is the only combination in development with activity across all four Ambler classes including IMP-type MBLs, potentially covering CRE, MBL-producers, and CRAB with a single agent
BL/BLI Combinations: Comparative Summary
| Agent | Class A | Class B (MBL) | Class C | Class D | Target Pathogens |
|---|---|---|---|---|---|
| SUL-DUR | ✓ | ✗ | ✓ | ✓✓ | CRAB |
| ATM-AVI | ✓ | Stable* | ✓ | ± | MBL-Enterobacterales |
| FEP-ENM | ✓ | ✗ | ✗ | ✗ | ESBL |
| FEP-TAN | ✓ | VIM, NDM | ✓ | ✓ | CRE, MBL |
| FEP-ZID | ✓ | Enhanced | ✓ | ✓ | XDR-PA, CRE |
| MER-XER | ✓ | NDM, VIM, IMP | ✓ | ✓ | CRE, MBL, CRAB |
*Aztreonam stable to MBLs; avibactam covers serine enzymes
Selection Guide
- CRAB → Sulbactam-durlobactam or MER-XER (when available) - MBL-Enterobacterales → ATM-AVI, FEP-TAN, or MER-XER (when available) - ESBL → Cefepime-enmetazobactam - XDR Pseudomonas → Cefepime-zidebactam (when available)
Part 3: Oral Carbapenems and
Other Novel Agents
Oral carbapenems: Addressing the IV-to-PO gap
The clinical need:
- Patients stable on IV carbapenems
- Need oral step-down therapy
- Current options limited for MDR gram-negatives
Two agents in development:
| Agent | Status | Primary Indication |
|---|---|---|
| Tebipenem | Likely approval in 2026 | cUTI/AP |
| Sulopenem | FDA Approved | uUTI |
Tebipenem
Oral carbapenem prodrug (pivoxil hydrobromide)
Spectrum:
- MDR Enterobacterales
- ESBL-producers
- Selected gram-positives
- NOT carbapenemase-producers
ADAPT-PO Trial:
- Tebipenem 600 mg PO q8h
- vs. ertapenem 1 g IV daily
- Noninferiority achieved
- Similar safety profile
Current Status
Initial NDA insufficient for FDA approval - PIVOT-PO trial (vs. IV imipenem) ongoing
Sulopenem (Orlynvah)
FDA approved for uncomplicated UTI → Currently no EMA authorization
Spectrum:
- MDR Enterobacterales
- ESBL-producers
- AmpC-producers
- NOT carbapenemase-producers
Development Path:
- Initial Phase 3: Variable results
- REASSURE Trial: Noninferiority to amoxicillin-clavulanate achieved
- NDA resubmitted 2024
Clinical Niche
Sulopenem offers an oral option for patients with MDR gram-negative uUTI who have limited other oral alternatives
Ceftobiprole (Zevtera/Mabelio):
Fifth-generation cephalosporin
FDA Approved for multiple MRSA indications
Mechanism:
- Inhibits PBPs including PBP2a
- Active against MRSA
- Broad gram-positive/gram-negative activity
Approved Indications:
- S. aureus bacteremia
- Right-sided endocarditis
- ABSSSI
- Community-acquired pneumonia
- Role in HAP/VAP- higher mortality than comparator
Dosing:
- 500 mg IV over 2 hours
- Every 6-8 hours
- Renal adjustment required
ERADICATE Trial:
Noninferior to daptomycin for complicated S. aureus bacteremia
Contezolid: Safer oxazolidinone?
Novel oxazolidinone in development
Design Goal:
Reduce myelosuppression and serotonergic effects
seen with linezolid/tedizolid
Spectrum:
- MRSA
- VRE
- Penicillin-resistant S. pneumoniae
Phase 3 (cSSTI):
Noninferior to linezolid with potentially better safety
Availability:
- IV and oral formulations
- Global trial for diabetic foot infection ongoing
Afabicin: Selective anti-staphylococcal agent
Novel FabI inhibitor with unique selectivity
Mechanism:
- Enoyl-acyl carrier protein reductase (FabI) inhibitor
- Targets fatty acid synthesis
- Highly selective for S. aureus
Not active against:
- Other gram-positives
- Gram-negatives
Clinical Development:
- Phase 2: Noninferior to vancomycin/linezolid for staphylococcal ABSSSI
- Planned: Bone and joint infection trials
Advantages:
- Narrow spectrum = antimicrobial stewardship friendly
- Novel MOA
Gepotidacin: Novel topoisomerase inhibitor
First-in-class triazaacenaphthylene for uUTI and gonorrhea
Mechanism:
- Inhibits DNA gyrase AND topoisomerase IV
- Distinct binding site from fluoroquinolones
- Active against FQ-resistant strains
Spectrum:
- Gram-positives
- Gram-negatives including MDR E. coli
- MDR N. gonorrhoeae
Dosing (oral):
- uUTI: 1500 mg BID × 5 days
- Gonorrhea: 3000 mg × 2 doses (10-12h apart)
Phase 3 Results:
- Noninferior to nitrofurantoin (uUTI)
- Noninferior to ceftriaxone + azithromycin (gonorrhea)
Addressing a Critical Need
Gepotidacin provides an oral option for gonorrhea - crucial as resistance to ceftriaxone emerges
Zoliflodacin: Single-dose gonorrhea treatment
First-in-class spiropyrimidinetrione for N. gonorrhoeae
Mechanism:
- Type II topoisomerase inhibitor
- Unique binding sites on DNA gyrase
- Distinct from fluoroquinolones
Key advantage:
Active against strains resistant to:
- Cephalosporins
- Fluoroquinolones
- Other drug classes
Phase 3 Results:
Single 3-g oral dose:
- Noninferior to IM ceftriaxone + oral azithromycin
- High cure rates for urogenital/rectal infection
- Lower efficacy for pharyngeal infection
Clinical Pearl
Single-dose oral therapy dramatically improves treatment adherence - critical for STI management
Other Agents: Brief overview
- Broad-spectrum (gram-pos/gram-neg)
- ZEUS trial: Noninferior to pip-tazo for cUTI/AP
- Oral form available in US, IV and oral in ITaly
Ridinilazole:
- Bibenzidamole disrupting cell division
- Targeted activity against C. difficile
- “Microbiome sparing”
- Pivotal Ri-CoDIFy 1 and 2 Phase 3 trials, ridinilazole failed to demonstrate superiority to oral vancomycin on sustained clinical response, missing the primary endpoint needed for approval.
Ibezapolstat:
- DNA polymerase IIIC inhibitor
- Also targets C. difficile
- Microbiome sparing
- Awaiting phase III trials
- First-in-class LeuRS inhibitor
- An aminoacyl-tRNA synthetase required for protein synthesis. Mechanistically it uses the so-called OBORT mechanism (oxaborole tRNA trapping)
- In development for NTM infections. Repurposed after rapid development of resistance in gram-negatives
- Activity against MAC and M. abscessus
- Available outside US for decades
- Narrow spectrum (staphylococci)
- Usually adjunctive therapy
Part 4: Summary and Conclusions
Novel agents summary table
| Agent | Target | Key Indications | Status |
|---|---|---|---|
| SUL-DUR | CRAB | HABP/VABP | FDA approved, AIFA waiting |
| ATM-AVI | MBL-Enterobacterales | cIAI, HABP/VABP | Late development |
| FEP-ENM | ESBL | cUTI/AP | FDA approved, No AIFA approval |
| FEP-TAN | CRE, MBL | cUTI/AP | Phase 3 complete |
| FEP-ZID | XDR-PA, CRE | cUTI/AP | Phase 3 |
| MER-XER | CRE, MBL, CRAB | cUTI/AP, HABP/VABP | Phase 3 |
| Sulopenem | MDR Enterobacterales | uUTI | FDA approved |
| Ceftobiprole | MRSA | Bacteremia, ABSSSI, CABP | FDA, AIFA approved |
| Gepotidacin | MDR E. coli, N. gonorrhoeae | uUTI, gonorrhea | FDA approved, AIFA waiting |
| Zoliflodacin | MDR N. gonorrhoeae | Gonorrhea | FDA approved, AIFA waiting |
Key takeaways
The AMR challenge is growing - MDR organisms continue to emerge faster than new treatments
Critical priority pathogens (CRAB, CRE) now have improved treatment options with novel BL/BLI combinations
MBL-producing organisms - ATM-AVI and FEP-TAN address this previously untreatable gap
Oral options expanding - Sulopenem, tebipenem, gepotidacin (Ross et al., 2025; Wagenlehner et al., 2024)
Economic sustainability remains a challenge - pull incentives needed alongside push incentives
Antimicrobial stewardship essential - new agents should be reserved for appropriate indications
Clinical decision framework
or MER-XER
FEP-TAN, or MER-XER
FEP-TAN, or MER-XER
(when available)
options
or existing options
Zoliflodacin
(when available)
Looking Forward
Promising developments:
- Multiple agents in Phase 3 trials
- First MBL-active inhibitors approaching market
- Oral options for MDR infections expanding
Ongoing challenges:
- Post-approval sustainability for manufacturers
- Appropriate use and stewardship
- Continued emergence of novel resistance mechanisms
Final Thought
New antibiotics are necessary but not sufficient - stewardship, infection prevention, and diagnostics must work together to combat AMR
Supplementary: Dosing Quick Reference
| Agent | Dose | Frequency | Infusion | Renal Adjustment |
|---|---|---|---|---|
| SUL-DUR | 2 g (1g-1g) | q6h | 3 hours | Yes |
| ATM-AVI | 1500-500 mg* | q6h | 3 hours | Yes |
| FEP-ENM | 2-0.5 g | q8h | 2 hours | Yes |
| FEP-TAN | 2.5 g (2g-500mg) | q8h | 2 hours | Yes |
| FEP-ZID | 3 g (2g-1g) | q8h | 3 hours | Yes |
| MER-XER | 2-1 g | q8h | 3 hours | Yes |
| Ceftobiprole | 500 mg | q6-8h | 2 hours | Yes |
*Loading dose: 500-167 mg
Clinical Pearl
Extended infusions optimize time above MIC for these β-lactam agents