Macrolides, Ketolides, and Clindamycin
2026-07-07
Macrolides, Ketolides and Clindamycin
Russell E. Lewis, Pharm.D
Associate Professor of Infectious Diseases (MEDS-10/B)

russelledward.lewis@unipd.it
https://github.com/Russlewisbo
Slides and course materials: www.idpadova.com
Outline
- Chemistry, mechanism of action, and the 50S ribosome
- The three resistance mechanisms (and why MLSB matters)
- Pharmacology of erythromycin, clarithromycin, azithromycin
- Cardiac safety — what Ray et al. taught us
- Antimicrobial spectrum and key clinical uses
- Ketolides — telithromycin and the solithromycin story
- Clindamycin — anaerobes, MRSA, and toxin suppression
- Practical pearls for the consult service
Chemistry & Mechanism
The Macrolide family
- 14-member ring: erythromycin, clarithromycin, roxithromycin
- 15-member ring (azalide): azithromycin — nitrogen inserted into the lactone
- 16-member ring: spiramycin, josamycin, tylosin (veterinary)
- Ketolides: 14-member macrolactone with a 3-keto group instead of L-cladinose at C-3
- Telithromycin, solithromycin
- Lincosamides: not macrolides chemically (no macrolactone) but share the ribosomal target — clindamycin, lincomycin
Mechanism of action
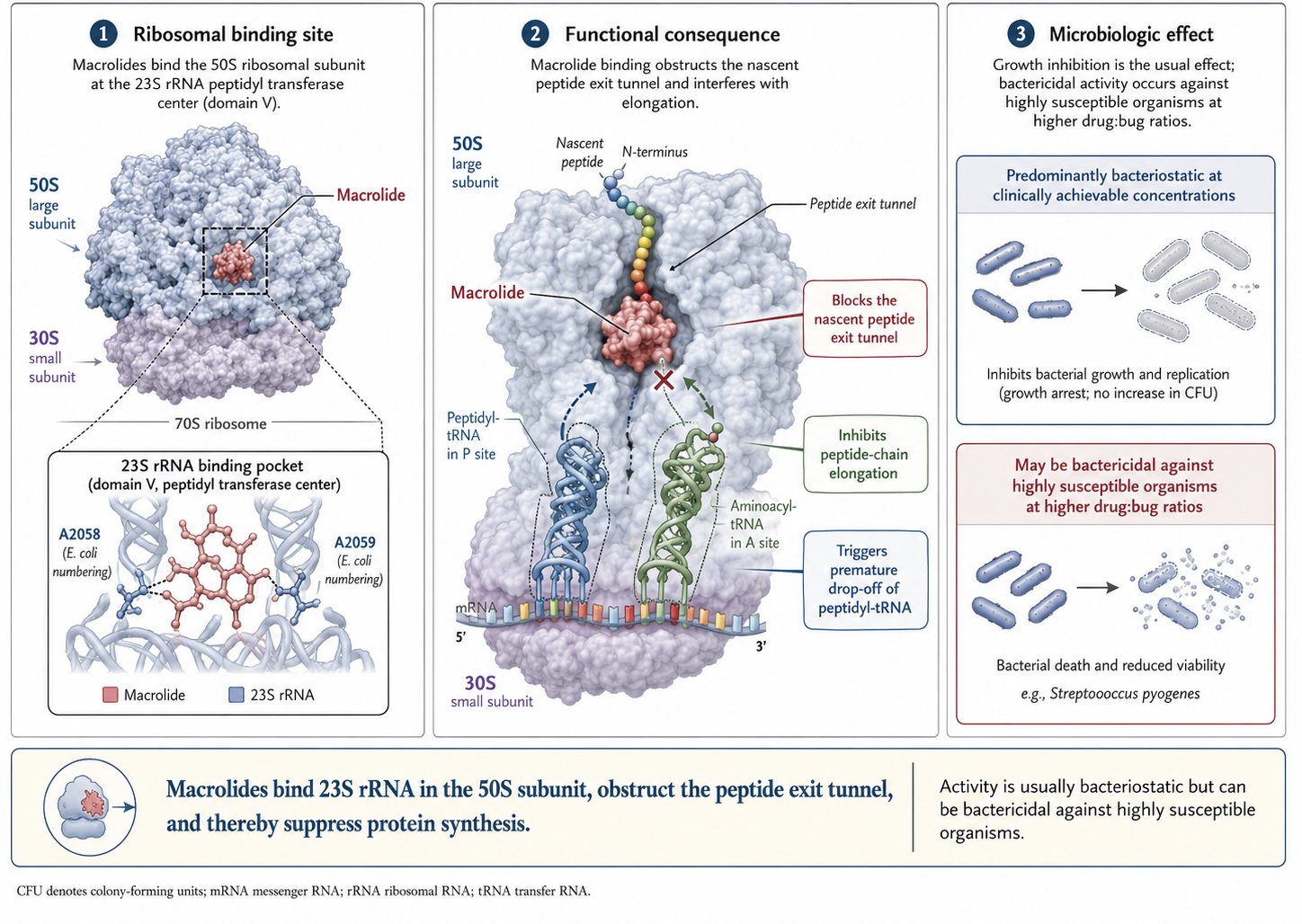
Bacteriostatic vs. bactericidal
- All four agents (erythromycin, clarithromycin, azithromycin, clindamycin) are protein-synthesis inhibitors → classically bacteriostatic
- Become bactericidal under specific conditions:
- High drug concentration relative to MIC
- Organisms in active growth phase
- Low inoculum
- Clinical relevance: avoid as monotherapy for endocarditis, neutropenic infections, meningitis (with rare specific exceptions)
- However, perception of less effective “static” activity may actually be a consequence of macrolide PK- (large Vd, low bloodstream concentrations)
Resistance Mechanisms
Three resistance mechanisms — Overview
| Mechanism | Effect | Cross-resistance |
|---|---|---|
| Target site modification (Erm methylation, ribosomal mutation) | 23S A2058 methylated/mutated | Full MLSB (macrolides + lincosamides + streptogramin B) |
| Efflux (Mef, Msr) | Drug pumped out of cell | Macrolides only (M phenotype) — clindamycin spared |
| Enzymatic inactivation (esterases, phosphotransferases) | Drug destroyed | Variable; uncommon clinically |
Target methylation — the erm Genes
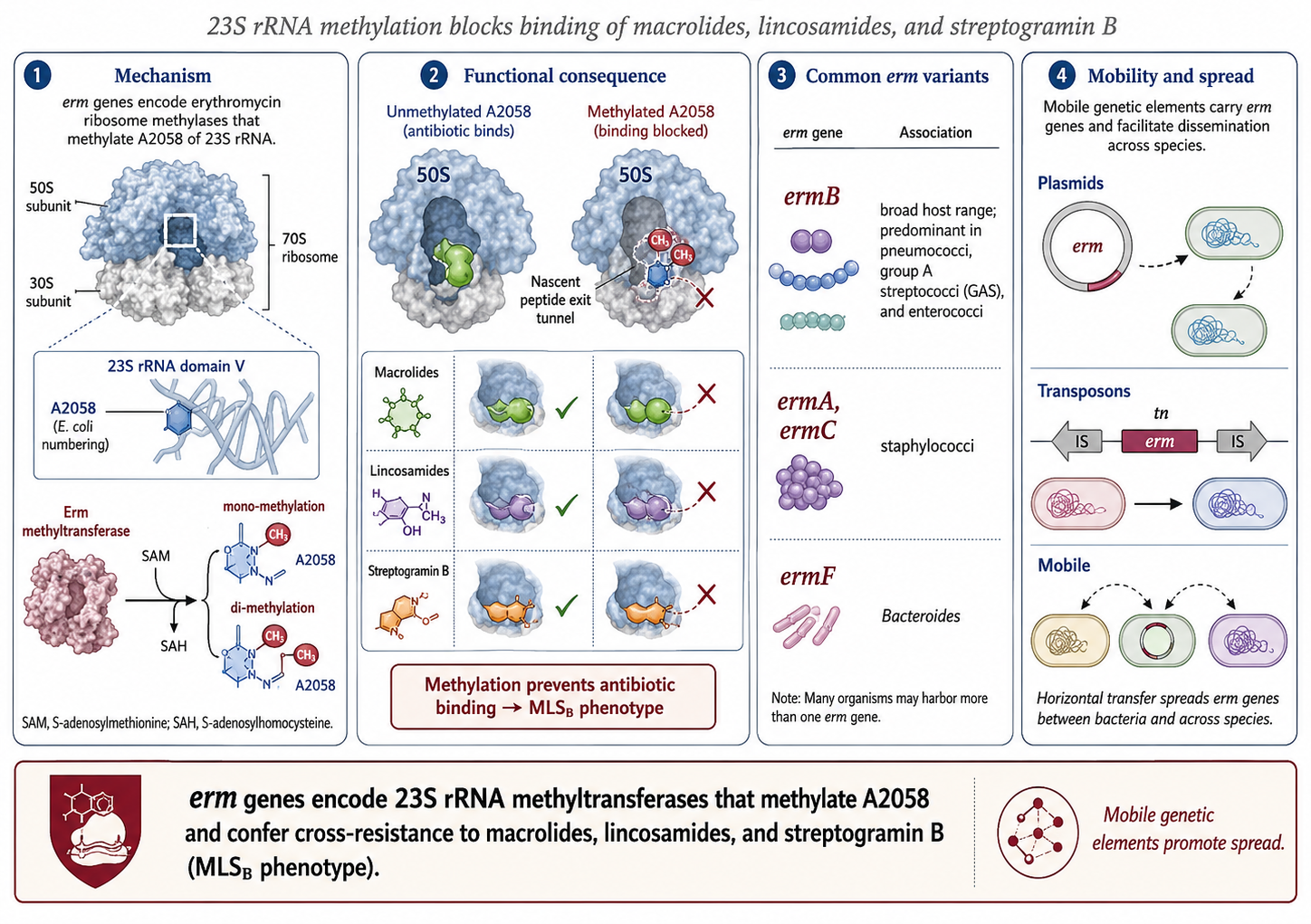
Constitutive vs. inducible MLSB
- Constitutive (cMLSB): erm expressed all the time → resistant to erythromycin AND clindamycin on initial testing
- Inducible (iMLSB): erm transcript untranslated until a macrolide (or partial agonist) is encountered → appears erythromycin-resistant, clindamycin-susceptible on AST
- Risk: if you treat an iMLSB isolate with clindamycin, erm gets induced → emergent resistance and clinical failure
The D-test
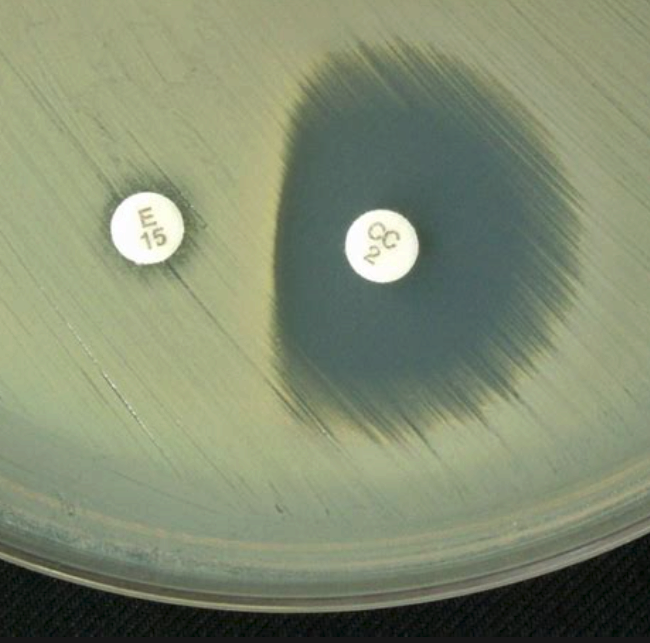
- Disk-diffusion screen for inducible clindamycin resistance
- Erythromycin disk placed adjacent to clindamycin disk on the plate
- If erythromycin induces erm expression, the zone of clindamycin inhibition gets flattened on the side facing the erythromycin disk — forming a “D” shape
- D-test positive → report clindamycin as resistant despite the susceptible-looking MIC
- Routine in clinical micro labs for staphylococci and group A strep
Efflux — mef and msr
- mefA / mefE (Streptococcus, found in pneumococci): pumps 14- and 15-member macrolides out of the cell
- msrA (Staphylococcus): ATP-binding cassette pump; efflux of macrolides and streptogramin B
- M phenotype: erythromycin/azithromycin-resistant but clindamycin- and 16-member macrolide-susceptible
- Usually lower-level resistance than MLSB — high inocula can overwhelm the pump
Ribosomal mutations and atypicals
- Single-step point mutations at 23S rRNA A2058 / A2059 confer high-level macrolide resistance
- Particularly relevant for organisms with few rRNA operons (1–2 copies), where a single mutation knocks out most ribosomes:
- Mycoplasma pneumoniae — A2058G/C mutations driving outbreaks across Asia (>90% in parts of China/Japan), now spreading in Europe
- Mycobacterium avium complex — 23S mutations under clarithromycin monotherapy
- Neisseria gonorrhoeae — 23S rRNA mutations and mtr efflux
- Helicobacter pylori — A2143G is the dominant driver of clarithromycin failure
Pharmacology
Erythromycin — preparations
| Preparation | Notes | Typical adult dose |
|---|---|---|
| Base | Acid-labile; enteric-coated | 250–500 mg PO q6–12h |
| Stearate | Acid-stable salt | Similar |
| Ethylsuccinate | Suspension/pediatric | 400–800 mg PO q6–12h |
| Lactobionate | IV form | 15–20 mg/kg/day divided q6h, max 4 g |
| Estolate | Highest bioavailability; hepatotoxicity risk | Largely abandoned |
Erythromycin — pharmacokinetics
- Oral absorption: variable, reduced by food and gastric acid
- Half-life: 1.5–2 hours — frequent dosing required
- Distribution: broad except poor CNS penetration
- Metabolism: hepatic via CYP3A4 (substrate and potent inhibitor)
- Elimination: primarily biliary; minimal renal — no renal-failure adjustment
- Hepatic dysfunction: caution; reduce dose
Erythromycin — Adverse effects
- GI: dose-related nausea, vomiting, diarrhea (mediated by motilin receptor agonism — basis for use as prokinetic)
- Hepatobiliary: cholestatic hepatitis (estolate > other forms)
- Ototoxicity: reversible high-tone hearing loss with high IV doses or renal failure
- Cardiac: QTc prolongation, torsades de pointes — ↑ with renal dysfunction, drug interactions
- Hypertrophic pyloric stenosis in neonates exposed in early infancy
Drug interactions — The statin story
- Erythromycin and clarithromycin ↑↑↑ simvastatin and lovastatin exposure (5–10× AUC)
- Documented fatal rhabdomyolysis with simvastatin + clarithromycin co-prescription
- US FDA: avoid concurrent simvastatin > 20 mg or lovastatin > 20 mg with these macrolides
- Atorvastatin less affected but still ↑ AUC by ~80%
- Rosuvastatin, pravastatin, fluvastatin — not significant CYP3A4 substrates, safer pairings
- Azithromycin — minimal effect; preferred macrolide when statin therapy must continue
Macrolides in pregnancy
- Azithromycin and erythromycin: Category B / consensus-safe — extensive human pregnancy data
- Clarithromycin: Category C — animal teratogenicity; avoid in 1st trimester if alternatives exist
- Pertussis treatment in pregnancy → azithromycin
- Chlamydia in pregnancy → azithromycin single dose
- Erythromycin estolate avoided — cholestatic hepatitis in pregnancy
- Spiramycin (Europe) for gestational toxoplasmosis to prevent vertical transmission
Erythromycin — Drug interactions
Potent CYP3A4 inhibitor — many clinically important interactions:
- Warfarin — INR rises
- Statins (especially simvastatin, lovastatin) — rhabdomyolysis
- Calcineurin inhibitors (cyclosporine, tacrolimus) — toxic levels
- Theophylline — toxicity
- Carbamazepine — toxicity
- Colchicine — fatal toxicity reported- myopathy, neuromyopathy, bone marrow suppression, and potentially multi-organ failure
- QT-prolonging drugs (amiodarone, sotalol, fluoroquinolones, antipsychotics) — additive arrhythmia risk
Clarithromycin
- Better-tolerated GI profile than erythromycin; acid-stable
- Half-life ~3–7 hours (parent) and ~5–9 hours (active 14-OH metabolite)
- Active metabolite (14-OH-clarithromycin): independently potent against H. influenzae
- CYP3A4 inhibitor — interaction profile similar to erythromycin
- Renal elimination is significant — reduce dose if CrCl <30 mL/min
- Twice-daily standard; once-daily extended-release available
Azithromycin — the outlier
- 15-member azalide ring (nitrogen substitution) — explains unique properties
- Half-life: 40–68 hours in serum, 2–4 days in tissue
- Massive tissue concentrations — accumulates in macrophages, fibroblasts, neutrophils (1000× plasma)
- Tissue >> plasma → unreliable for bacteremia, but ideal for intracellular pathogens
- Not a significant CYP3A4 inhibitor — far fewer drug interactions
- Predominantly biliary elimination — no renal dose adjustment
PK/PD Principles
- Macrolides are protein-synthesis inhibitors → AUC/MIC is the primary PK/PD index
- Azithromycin’s prolonged post-antibiotic effect supports once-daily and even single-dose regimens
- Erythromycin and clarithromycin are more time-dependent — need frequent dosing to maintain trough levels
- High tissue/plasma ratios for azithromycin mean serum concentrations underestimate target-site exposure
- For intracellular pathogens (Legionella, Chlamydia), tissue concentration is what matters
Comparing the three — Quick reference
| Property | Erythromycin | Clarithromycin | Azithromycin |
|---|---|---|---|
| Half-life | 1.5–2 h | 3–7 h | 40–68 h |
| Active metabolite | No | 14-OH (active) | No |
| CYP3A4 inhibitor | Strong | Strong | Minimal |
| Renal adjustment | No | Yes (CrCl <30) | No |
| Tissue penetration | Modest | Good | Exceptional (intracellular) |
| Frequency | q6h | q12h | q24h (or single dose) |
Cardiac Safety
QT Prolongation — Mechanism
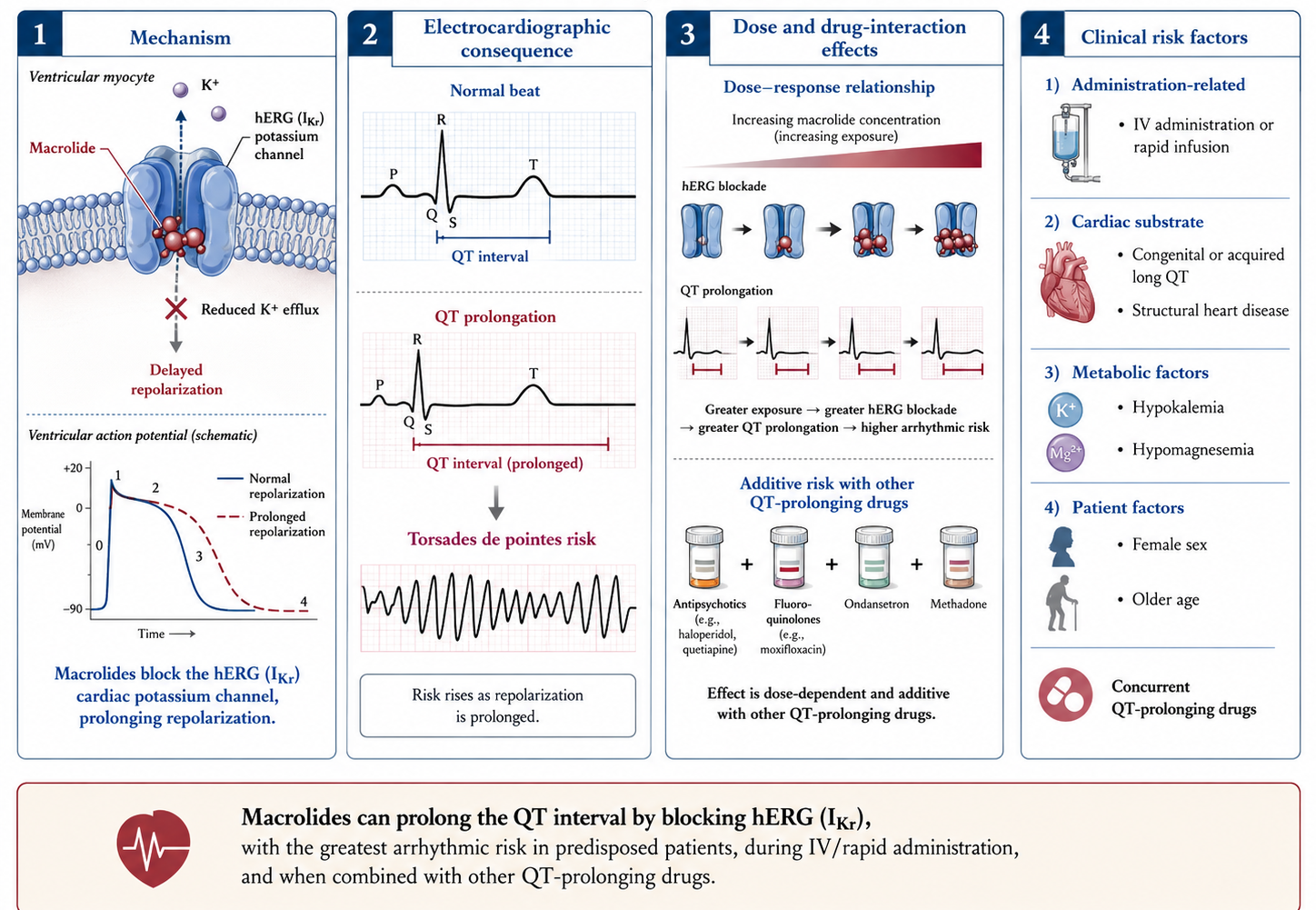
Ray et al. — the NEJM Data
- Ray 2004 (NEJM): Oral erythromycin was associated with a 5× increase in sudden cardiac death; risk further amplified by CYP3A4 inhibitors (verapamil, diltiazem)
- Ray 2012 (NEJM): During 5-day azithromycin courses, +47 cardiovascular deaths per million courses vs. amoxicillin; concentrated in patients at highest baseline cardiovascular risk
- Albert 2014 (AJRCCM): Class-level synthesis — risk is real but small in absolute terms; restrict in high-risk patients
Allergy and hypersensitivity
- True macrolide allergy is uncommon (~0.4–3% in surveys)
- IgE-mediated immediate reactions rare; most are delayed mild rashes
- Cross-reactivity within the class is variable — a patient with documented azithromycin urticaria often tolerates clarithromycin, and vice versa
- No cross-reactivity between macrolides and lincosamides (clindamycin) — clindamycin remains an option
- Stevens-Johnson syndrome rare but reported with all macrolides
- Skin testing not standardized; rechallenge under observation often diagnostic
Practical risk stratification
- Low risk: young, structurally normal heart, no QT drugs → proceed
- Moderate risk: older, mild electrolyte derangement, single QT drug → consider alternatives (doxycycline often serves)
- High risk: known long QT, QT >500 ms, recent torsades, multiple QT drugs → avoid macrolides
- Check ECG and correct K+ / Mg++ before IV erythromycin in critically ill patients
Spectrum & Clinical Use
Spectrum — Macrolides at a glance
- Excellent: atypicals (Mycoplasma, Chlamydia, Legionella), Bordetella, Helicobacter, Treponema pallidum (allergy backup), Borrelia (children), MAC, Toxoplasma (cyst killing)
- Good (where susceptible): GAS, pneumococcus, group B strep
- Variable: Haemophilus influenzae (clarithromycin metabolite, azithromycin OK; erythromycin poor)
- None or unreliable: Enterobacterales (except limited GI use), Pseudomonas, Acinetobacter, anaerobes (variable), enterococci, MRSA
- Mycobacterial: active against MAC, M. leprae; M. tuberculosis is intrinsically resistant
M. tuberculosis — Intrinsic resistance
- M. tuberculosis is intrinsically macrolide-resistant despite being a mycobacterium
- Mechanism: chromosomally encoded Erm(37) rRNA methyltransferase
- A positive AFB smear that is macrolide-resistant is not necessarily MDR-TB — it could simply be M. tuberculosis
- Conversely, MAC and most NTM are macrolide-susceptible — species identification matters before therapy
- Do not include a macrolide in an “expanded TB regimen” — no benefit
Macrolides — Less common pathogens
- Bartonella spp. — azithromycin or doxycycline (cat-scratch disease, bacillary angiomatosis)
- Brucella spp. — macrolides not first-line; reserved for combinations in specific settings
- Whipple disease (Tropheryma whipplei) — doxycycline + hydroxychloroquine first-line; macrolides limited role
- Rhodococcus equi — azithromycin combined with rifampin ± aminoglycoside in immunocompromised
- Mycoplasma genitalium — extended-course azithromycin; rising macrolide resistance worldwide
Geographic resistance snapshot
- Macrolide resistance varies dramatically by region — driven by background prescribing intensity
- S. pneumoniae (invasive isolates, recent surveillance):
- North America: ~30–40% (mostly mef-mediated, lower MICs)
- Europe: 20–30% overall, higher in Mediterranean / Italy (mostly ermB-mediated, high MICs)
- East Asia: 50–80% (very high, predominantly ermB)
- M. pneumoniae macrolide resistance: <10% in most of Europe, 70–95% in parts of China and Japan
- Practical: when traveling or treating recent immigrants from high-resistance regions, mentally adjust empiric coverage
Pneumococcal susceptibility — the Italian Picture
- Macrolide resistance in S. pneumoniae is high in Southern Europe
- Italy: pneumococcal macrolide resistance ~25–35% in invasive isolates (recent surveillance)
- Dominant mechanism in Europe: ermB (MLSB) → high MICs, also clindamycin-R
- US: more mef-mediated efflux → lower-level resistance
- Clinical implication: azithromycin monotherapy is inadequate empiric coverage for bacteremic pneumococcal pneumonia in Italy
Clinical Uses — Respiratory
Community-acquired pneumonia
- 2019 ATS/IDSA guideline: macrolide monotherapy reserved for outpatients with low resistance prevalence (<25%); otherwise β-lactam + macrolide combination or respiratory fluoroquinolone
- Role: covers atypicals (Mycoplasma, Chlamydia, Legionella) that β-lactams miss
- Inpatient CAP: ceftriaxone + azithromycin remains a standard regimen
- Italy: pneumococcal resistance generally exceeds the 25% threshold — guideline favors β-lactam + macrolide
Atypical pneumonia
- Mycoplasma pneumoniae — azithromycin or doxycycline; rising macrolide resistance in adolescents/young adults
- Chlamydia pneumoniae — azithromycin, clarithromycin, doxycycline
- Legionella pneumophila — azithromycin or fluoroquinolone (levofloxacin preferred for severe disease)
- Mycoplasma macrolide resistance is a particular issue in pediatric cases — consider doxycycline if no response after 48 h of macrolide
Pertussis
- Treatment of choice: azithromycin (5-day course) or clarithromycin (7-day course); erythromycin is alternative but worse tolerated
- Post-exposure prophylaxis: same regimens for close contacts within 21 days of cough onset
- Infants <1 month: azithromycin preferred — erythromycin estolate has been linked to hypertrophic pyloric stenosis
- Antibiotic eliminates carriage and reduces transmission but does not shorten illness once paroxysmal phase begins
Mycobacterium avium Complex (MAC)
- Pulmonary MAC: macrolide-based triple regimen (clarithromycin or azithromycin + ethambutol + rifampin / rifabutin) per 2020 ATS/ERS/ESCMID/IDSA guideline
- Disseminated MAC (AIDS, severe immunosuppression): same combination, longer duration
- Resistance prevention: never use macrolide monotherapy — 23S rRNA mutations emerge rapidly
- Azithromycin: weekly 1200 mg for primary prophylaxis in AIDS patients with CD4 <50 (largely obsolete since modern ART)
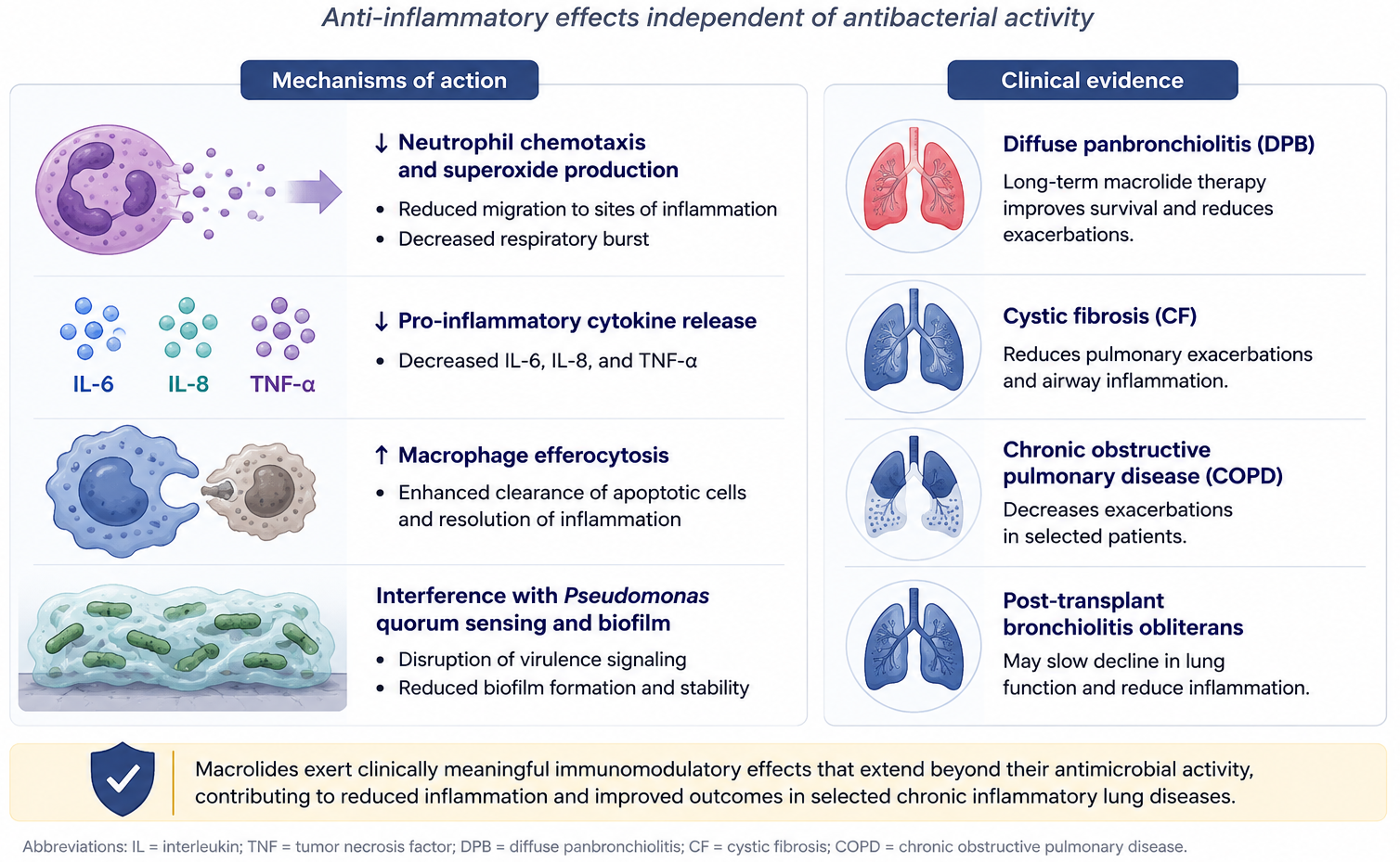
Diffuse panbronchiolitis and chronic airway disease
- Diffuse panbronchiolitis (largely Japanese cohort): low-dose erythromycin transformed survival from <50% at 5 years to >90% (Kudoh 1998) — an early demonstration of macrolide immunomodulation
- Cystic fibrosis with chronic P. aeruginosa colonization: azithromycin 3×/week improves lung function, reduces exacerbations
- Non-CF bronchiectasis: azithromycin reduces exacerbations
- COPD (Albert 2011, NEJM): azithromycin 250 mg daily reduced acute exacerbations — but hearing loss and arrhythmias limit chronic use
Clinical uses — Non-Respiratory
Helicobacter pylori
- Clarithromycin-based triple therapy (PPI + clarithromycin + amoxicillin or metronidazole) was first-line — but rising clarithromycin resistance (~30%+ in many populations) is reducing efficacy
- Maastricht VI / European consensus now favors bismuth quadruple therapy as first-line where clarithromycin resistance exceeds 15%
- Macrolide resistance driven by A2143G mutation in 23S rRNA
- Consider testing for susceptibility before retreatment
Chlamydia trachomatis — Urogenital and Rectal
- Urogenital chlamydia: azithromycin 1 g single dose or doxycycline 100 mg BID × 7 days
- Geisler 2015 (NEJM): doxycycline non-inferior to azithromycin overall but superior in men with urethritis (~3% failure with doxy vs. 5% with azithro)
- Rectal chlamydia (MSM): azithromycin clearly inferior to doxycycline — Lau 2021 (NEJM) microbiologic cure 76% azithro vs. 100% doxy
- Current US/European guideline: doxycycline 7 days is first-line; azithromycin reserved for adherence concerns or pregnancy
Trachoma and mass drug administration
- WHO trachoma elimination strategy (SAFE): annual single-dose azithromycin to entire endemic communities (mass drug administration, MDA)
- Bailey 1993 RCT established single-dose azithromycin equivalent to 6 weeks of tetracycline ointment
- MORDOR trial (Keenan 2018 NEJM): biannual azithromycin MDA in sub-Saharan Africa reduced all-cause childhood mortality by ~14%
- MORDOR II (Keenan 2019): benefit persists but growing concern about resistance selection — including macrolide-R S. pneumoniae, E. coli, S. aureus
Neisseria gonorrhoeae — Don’t use azithromycin!
- Azithromycin has been abandoned for gonorrhea due to widespread resistance
- 2021 CDC update: ceftriaxone 500 mg IM × 1 alone (no longer dual therapy with azithromycin)
- European guideline (IUSTI 2020): ceftriaxone 1 g + azithromycin 2 g — but actively under revision
- Macrolide resistance driven by 23S rRNA mutations and mtr efflux upregulation
- Solithromycin tested in Phase 3 — efficacy demonstrated but FDA rejected the drug on safety grounds
Toxoplasmosis and pregnancy
- Spiramycin (Europe; not FDA-approved in US): standard prophylaxis for T. gondii seroconversion during pregnancy — reduces fetal transmission
- Azithromycin and clarithromycin have in vitro and in vivo activity against tachyzoites and cyst stages
- Azithromycin + pyrimethamine — alternative to sulfadiazine + pyrimethamine in sulfa-allergic patients with cerebral toxoplasmosis (less data than clindamycin-based regimen — see clindamycin section)
Syphilis — A cautionary tale
- Single-dose oral azithromycin (2 g) was once an attractive alternative for penicillin-allergic syphilis
- Treatment failures emerged rapidly in San Francisco, Ireland, and elsewhere in the 2000s
- Resistance driven by the A2058G mutation in 23S rRNA of Treponema pallidum (the same residue as in Mycoplasma)
- US CDC guideline 2021: azithromycin no longer recommended for syphilis — desensitization to penicillin preferred for allergy
- Illustrative of how rapidly macrolide resistance can emerge in slow-growing pathogens
Babesiosis
- Standard regimen: atovaquone + azithromycin × 7–10 days (mild–moderate disease); IDSA 2020 guideline preferred over clindamycin + quinine in non-severe cases due to better tolerability
- Severe babesiosis or immunocompromised host: clindamycin + quinine (IV) or atovaquone + azithromycin combined with exchange transfusion when high parasitemia
- Immunocompromised patients (asplenic, B-cell lymphoma, anti-CD20 therapy) require prolonged courses (≥6 weeks)
Macrolide Immunomodulation
Macrolides as immunomodulators
Ketolides
Ketolides — Designed to overcome MLSB
- Semi-synthetic 14-member macrolides with a 3-keto group replacing the L-cladinose sugar
- Designed to bind both A2058 and A752 of 23S rRNA — second binding site maintains activity against MLSB isolates
- Telithromycin — first ketolide approved (2004); now severely restricted
- Solithromycin — second-generation; FDA rejected 2016
Telithromycin (Ketek)
- Approved 2004 for CABP, acute sinusitis, AECB
- Hepatotoxicity signal emerged post-marketing — including acute liver failure and deaths
- Also linked to visual disturbances, syncope, and exacerbation of myasthenia gravis (reports of fatal MG crises)
- FDA 2007: indications restricted to CABP only; black-box warnings added
- Now rarely used; not available in many European markets
Solithromycin — Promise and fall
- Demonstrated activity against MLSB-resistant pneumococci, macrolide-resistant M. genitalium and N. gonorrhoeae
- Two successful phase 3 CABP trials (oral and IV–to-oral) — non-inferior to moxifloxacin
- 2016 FDA Antimicrobial Drugs Advisory Committee: voted against approval due to hepatotoxicity signal (transaminase elevations in ~9% of patients) — given the telithromycin precedent
- Cempra’s resubmission and additional trials did not satisfy FDA; drug never approved in US or EU
- Gonorrhea phase 3 (Fernandes 2019, Lancet ID) — efficacy demonstrated but moot
Lefamulin — A Cousin, not a ketolide
- Pleuromutilin class — binds the 50S ribosome at the peptidyl transferase center, but at a distinct site from macrolides/ketolides
- Maintains activity against most MLSB-resistant pneumococci, S. aureus, atypicals
- FDA-approved 2019 for CABP (LEAP 1 and LEAP 2 trials — non-inferior to moxifloxacin)
- IV and oral formulations
- Adverse effects: QTc prolongation (CYP3A4 substrate and inhibitor — interactions matter)
- Conceptual placeholder for the gap solithromycin would have filled
Newer ketolides
- Nafithromycin (Wockhardt) — Indian-developed ketolide; phase 3 completed for CABP; approval pending in India
- Cethromycin — never reached market; failed phase 3
- The ketolide pipeline has stalled — investment moved to oxazolidinones and lefamulin instead
Clindamycin
Clindamycin — Origins
- Lincomycin isolated 1962 from Streptomyces lincolnensis (Nebraska soil sample)
- Clindamycin = 7(S)-chloro-7-deoxy-lincomycin (semi-synthetic, 1966)
- Improved oral absorption, GI tolerability, and antimicrobial potency vs. parent
- Not a macrolide — but binds the same 23S rRNA site, hence MLSB cross-resistance
Clindamycin — pharmacology
- Oral bioavailability ~90% (clindamycin HCl capsule) — can switch IV→PO 1:1
- Half-life: ~2.5 hours; q6–8h dosing
- Distribution: excellent into bone, joint, lung, abscess; poor CNS penetration even with inflamed meninges
- Metabolism: hepatic; no renal adjustment needed
- Active metabolites contribute to bactericidal activity in some settings
- Excellent intracellular concentrations (macrophages, PMNs)
Clindamycin — spectrum
- Excellent: Gram-positive aerobes (streptococci, methicillin-susceptible and many CA-MRSA staph), most anaerobes (including Bacteroides historically, though resistance is rising)
- Good: T. gondii, P. jirovecii (with primaquine), Plasmodium (with quinine), Babesia (with quinine), some atypical mycobacteria
- None or poor: enterococci, Listeria, Gram-negative aerobes, most Mycobacteria
- MRSA: depends on local epidemiology; CA-MRSA often susceptible, HA-MRSA more often resistant
Clindamycin — Resistance concerns
MLSB (constitutive or inducible) — covered earlier; check D-test for staph and GAS
Bacteroides fragilis resistance rising — current European rates 25–50% (varies); empiric reliance for intraabdominal infection has been abandoned
Resistance in Clostridioides difficile irrelevant to therapy because clindamycin causes rather than treats CDI
Lnu nucleotidyltransferase genes — emerging in streptococci
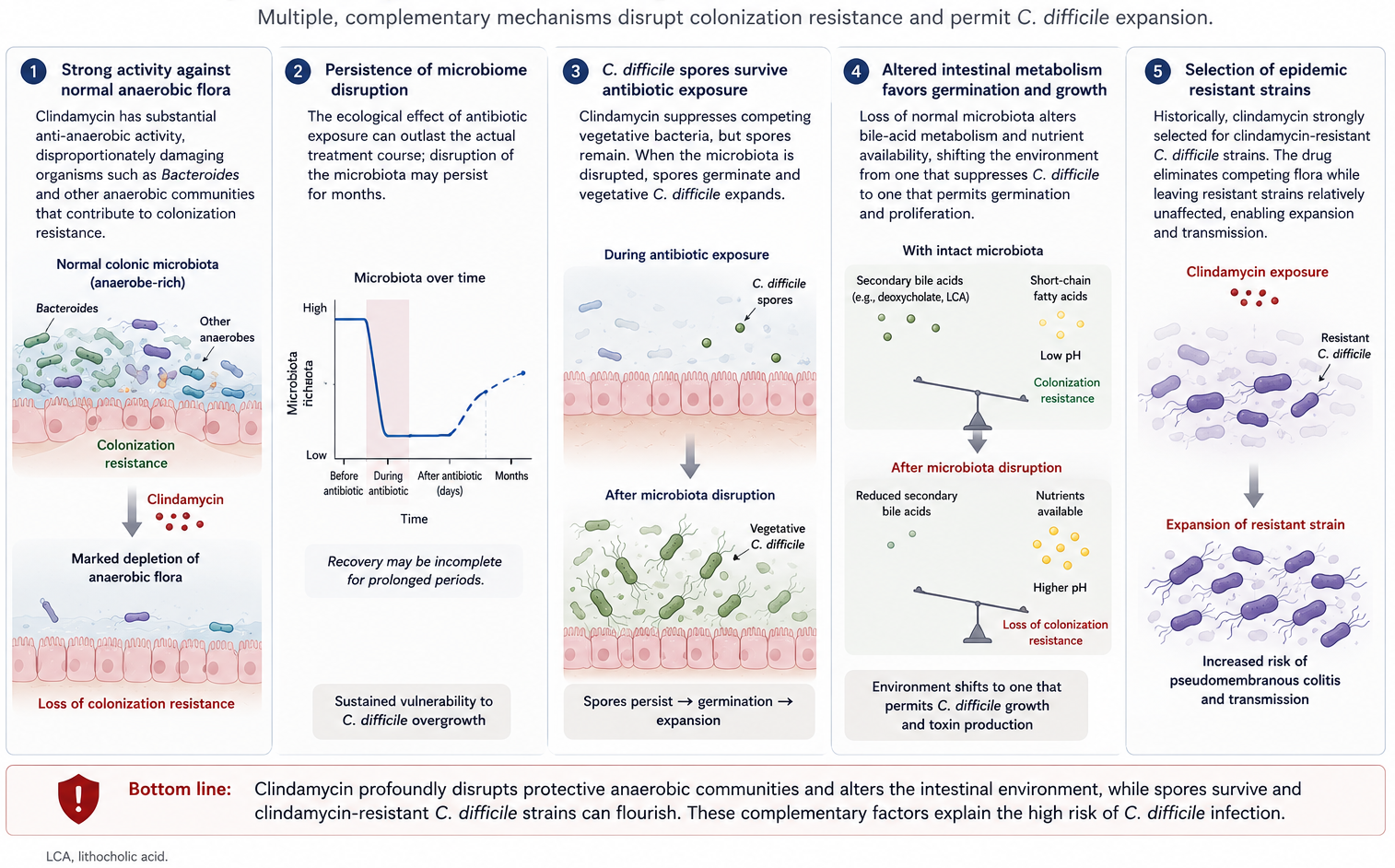
Clostridioides difficile — The cardinal adverse effect
Clindamycin has the highest relative risk of CDI among commonly used antibiotics in many epidemiologic studies
Disrupts colonic anaerobic flora → permissive environment for C. difficile
Risk persists for weeks to months after exposure
All forms (oral, IV, topical, even vaginal cream) implicated
Practical: don’t reach for clindamycin reflexively if a narrower or safer alternative exists in elderly, hospitalized, or recently antibiotic-exposed patients
Why is clindamycin uniquely good at selecting C. difficile?
More theoretical than real-life?
(ECCMID 2026 Late breakers)
The SNAP trial’s adjunctive clindamycin domain (5 days of clindamycin vs. no adjunctive antibiotic in S. aureus bacteraemia) found no mortality benefit and a signal of possible harm — the ICU subgroup had a 96% posterior probability of higher mortality.
C. difficile risk was not increased: CDI diarrhea was low and essentially identical in both arms (1.9% each), reassuring given this is likely the largest-ever RCT of clindamycin — though all-cause diarrhoea was higher in the clindamycin arm.
The suspected mechanism of harm is gut-microbiome/anaerobe disruption (loss of “colonization resistance”), not CDI specifically.
- The anti-toxin rationale (clindamycin inhibits ribosomal protein synthesis → less exotoxin production) was mechanistic only; outcome by clindamycin susceptibility/MIC was pre-specified but not yet analyzed, and the presenter expected it wouldn’t change the result.
Clindamycin — Clinical uses
Anaerobic infections
- Classic role: above-the-diaphragm anaerobes — aspiration pneumonia, lung abscess, dental infections, head and neck space infections
- Below-the-diaphragm: historically used for intraabdominal infection (B. fragilis); now superseded by metronidazole, β-lactam/inhibitor combinations due to rising resistance
- Necrotizing soft tissue infection: part of empiric broad-spectrum coverage (synergy plus toxin suppression)
Aspiration pneumonia and lung abscess
- Polymicrobial — oral aerobes + anaerobes (Prevotella, Fusobacterium, Peptostreptococcus)
- Clindamycin remains a reasonable monotherapy for community-acquired aspiration pneumonia with abscess
- Alternative: β-lactam/β-lactamase inhibitor (amoxicillin-clavulanate, ampicillin-sulbactam)
- Duration typically 3–6 weeks based on imaging and clinical response
CA-MRSA skin and soft tissue infection
- Clindamycin is a reasonable oral option for CA-MRSA SSTI if the isolate is susceptible AND D-test negative
- Pre-treatment: lab D-test on the isolate; if D-test positive, do not use clindamycin
- Useful particularly in children, pregnancy (TMP/SMX and doxycycline often relatively contraindicated)
- Penetrates abscess cavities and skin/soft tissue well
The Eagle effect — Why penicillin alone fails
- Eagle effect (Harry Eagle, 1948): paradoxical loss of β-lactam efficacy at very high inocula or in stationary-phase organisms
- In overwhelming GAS infection, the bacteria are not dividing rapidly → penicillin-binding proteins not actively engaged → killing slows
- Protein synthesis inhibitors (clindamycin, linezolid) are not growth-phase dependent — they suppress toxin production and slow viable bacterial replication independently
- Direct evidence in necrotizing fasciitis mouse models
- Justifies adjunctive clindamycin in invasive GAS even when isolate is susceptible to penicillin
Necrotizing fasciitis and invasive GAS
- Adjunctive clindamycin added to penicillin (or carbapenem) for invasive group A streptococcal infection
- Mechanism — three independent benefits:
- Toxin suppression — protein synthesis inhibitor reduces M protein, streptolysin O, SpeA, SpeB production
- Eagle effect mitigation — clindamycin not affected by stationary-phase bacterial density
- Anti-inflammatory — reduces cytokine release
- Stevens 2007: dramatic reduction in toxin gene expression by clindamycin in MSSA and GAS in vitro
- IDSA SSTI guideline: add clindamycin for invasive GAS or staphylococcal TSS
Streptococcal and staphylococcal TSS
- Streptococcal toxic shock syndrome (M protein-mediated, superantigen): clindamycin + β-lactam mandatory
- Staphylococcal TSS (TSST-1, enterotoxin-mediated): clindamycin + β-lactam (oxacillin for MSSA; vancomycin or linezolid + clindamycin for MRSA)
- IVIG considered in fulminant disease, particularly streptococcal TSS
- Clindamycin should be added even if the isolate’s susceptibility hasn’t returned
Clostridium perfringens and gas gangrene
- Penicillin + clindamycin remains standard for myonecrosis
- Stevens 1987 demonstrated reduced α-toxin and θ-toxin production with clindamycin exposure
- Same principle as GAS: kill (penicillin) + toxin suppression (clindamycin)
- Surgical debridement is the dominant therapeutic intervention
Bone and joint infections
- Clindamycin penetrates bone well
- Reasonable option for osteomyelitis caused by susceptible MSSA, CA-MRSA, streptococci
- Long-course oral therapy possible after IV induction — high oral bioavailability supports outpatient regimens
- Check D-test for staphylococci before committing to a prolonged clindamycin course
Pneumocystis jirovecii Pneumonia
- Clindamycin + primaquine is a salvage regimen for mild-moderate PCP in sulfa-allergic or TMP/SMX-failing patients
- Benfield 2008: clindamycin–primaquine appears more effective than pentamidine for second-line therapy
- Primaquine requires G6PD screening before initiation
- Not first-line — TMP/SMX remains preferred for severe disease
Cerebral toxoplasmosis
- Pyrimethamine + sulfadiazine + leucovorin is first-line
- Pyrimethamine + clindamycin + leucovorin is the preferred sulfa-allergic alternative
- Dannemann 1992: comparable efficacy of pyrimethamine + clindamycin vs. pyrimethamine + sulfadiazine for acute TE in AIDS patients
- Maintenance therapy until immune reconstitution (CD4 >200 for ≥6 months on ART)
Bacterial vaginosis
- Oral metronidazole 500 mg BID × 7 days — first-line
- Topical clindamycin 2% cream × 7 days — equivalent efficacy, often better tolerated
- Oral clindamycin 300 mg BID × 7 days — alternative
- Treatment during pregnancy may reduce preterm delivery risk in selected populations (controversial)
- Topical clindamycin cream → reports of CDI (Meadowcroft 1998)
Malaria — Clindamycin’s antiparasitic Role
- Quinine + clindamycin is recommended treatment for uncomplicated P. falciparum malaria in pregnancy (1st trimester) and in young children when ACT is not appropriate
- Mechanism: clindamycin inhibits apicoplast ribosomal protein synthesis (residual prokaryotic organelle) — delayed-death effect over 2 parasite cycles
- WHO regimen: quinine 10 mg/kg PO q8h + clindamycin 10 mg/kg PO q12h × 7 days
- Artesunate + clindamycin also evaluated
Severe babesiosis
- For severe babesiosis (high parasitemia, immunocompromise, asplenia, hemodynamic compromise): clindamycin + quinine IV is the historical regimen
- IDSA 2020 guideline now also accepts atovaquone + azithromycin as initial therapy even in severe cases, given better tolerability
- Exchange transfusion considered if parasitemia >10% or end-organ dysfunction
- Immunocompromised patients require prolonged therapy (≥6 weeks); confirmed clearance by smear and PCR
Practical Pearls
What you should remember — Macrolides
- A2058 is the keystone — every resistance mechanism converges there
- MLSB cross-resistance means erm methylation knocks out clindamycin too
- D-test inducible MLSB in staph and GAS — check it before using clindamycin
- Azithromycin is the macrolide with long half-life, tissue residence, and minimal CYP3A4 interactions
- QT prolongation is real — risk-stratify before prescribing in older, polypharmacy, or cardiac patients
- Italian pneumococcal resistance is high — macrolide monotherapy is not adequate for bacteremic CAP locally
What you should remember — Ketolides
- Designed to overcome MLSB — and biochemically they do
- Telithromycin → hepatotoxicity and MG exacerbation; severely restricted
- Solithromycin → never approved, despite successful CABP and gonorrhea trials, because of liver-signal concerns
- Nafithromycin may emerge in Indian and Asian markets
- For now, the ketolide class is essentially clinically unavailable in Europe
What you should remember— Clindamycin
- 90% oral bioavailability — uniquely friendly for IV→PO and OPAT
- Toxin suppression is the reason we add it to penicillin in invasive GAS and to oxacillin/vanco in TSS
- C. difficile risk is real and durable — don’t reach for it reflexively
- Useful in PCP salvage (with primaquine), cerebral toxoplasmosis (with pyrimethamine), severe babesiosis (with quinine), falciparum malaria in pregnancy
- The MLSB trap — D-test before committing to a long course in MRSA
Macrolides and COVID-19 — A Caution Tale
- Early 2020: azithromycin promoted (with hydroxychloroquine) for COVID-19 based on small open-label studies
- Mechanism rationale: anti-inflammatory effects + putative antiviral activity
- RECOVERY trial (Lancet 2021): no mortality benefit in hospitalized COVID-19 (n>7,700 patients)
- PRINCIPLE trial (Lancet 2021): no benefit in early outpatient COVID-19
- Net effect: contributed to short-term azithromycin overprescribing → measurable rises in macrolide resistance in some regions
- Lesson: enthusiasm without RCT data can drive unintended antimicrobial selection pressure
Pediatric considerations
- Azithromycin preferred in infants and young children — better tolerated, single daily dose
- Erythromycin estolate avoided in infants — pyloric stenosis risk in first 6 weeks
- Pediatric SSTI: clindamycin is a workhorse oral option (palatability is poor — flavored suspensions help)
- Clarithromycin dosed pediatrically for MAC, H. pylori, and pertussis
- Macrolide-resistant M. pneumoniae now common in pediatric outbreaks — consider doxycycline or fluoroquinolone for non-responders >8 years old
Antimicrobial stewardship implications
- Macrolides are among the most prescribed antibiotics globally — outpatient respiratory and STI indications
- Heavy use drives resistance in S. pneumoniae, GAS, H. pylori, N. gonorrhoeae, M. genitalium, M. pneumoniae
- Stewardship targets:
- Avoid azithromycin monotherapy for sinusitis, bronchitis, otitis when viral or self-limited
- De-escalate from broad combinations once pathogen identified
- Audit prolonged maintenance courses (CF, COPD) — defined indication, monitor for hearing/QT
- Substitute doxycycline for chlamydia in non-pregnant patients
- Reducing macrolide pressure has reduced pneumococcal resistance in Finland, Belgium, US ambulatory settings