Intra-abdominal Infections
Appendicitis & Infections of the Liver and Biliary System
2026-03-01
Intraabdominal Infections, Part 2
Prof. Russell E. Lewis
Department of Molecular Medicine
University of Padua
russelledward.lewis@unipd.it
https://github.com/Russlewisbo
slides available at: www.padovaid.com
 |
What is appendicitis?
- Acute inflammation of the vermiform appendix
- Often related to obstruction
- Complicated by polymicrobial infection
- Complications: perforation, peritonitis, intra-abdominal abscesses
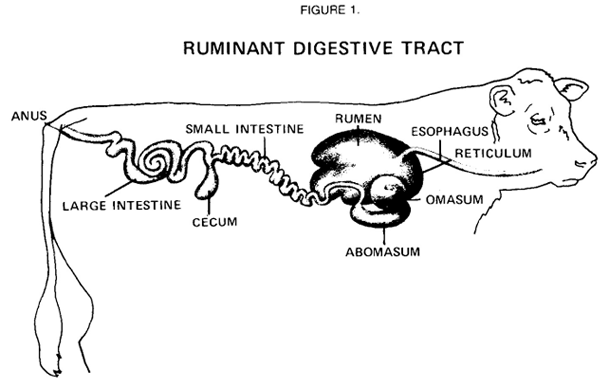
Anatomy of the appendix
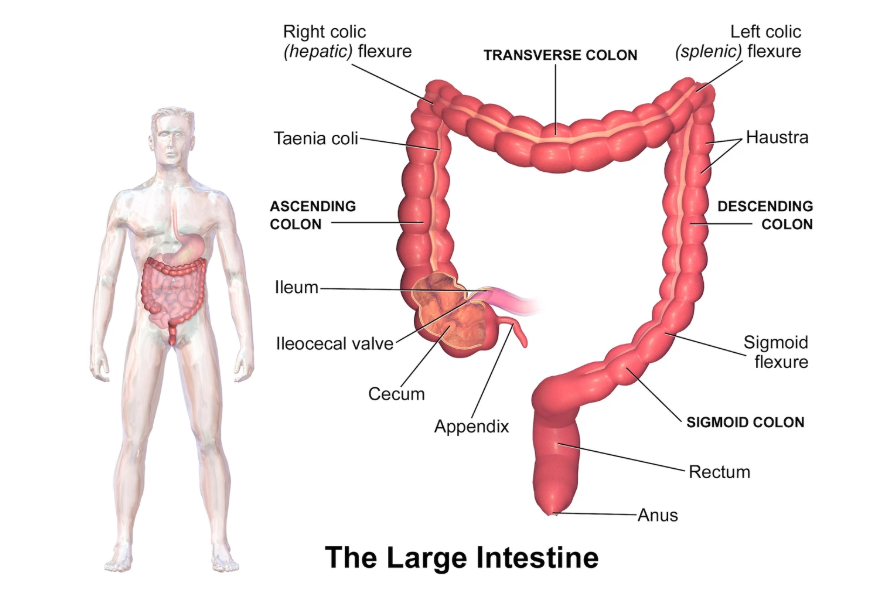
- Tube-shaped structure, 5–10 cm long
- Arises 2–3 cm below terminal ileum
- Medial posterior wall of cecum
- Common atypical positions: descending pelvic, transverse retrocecal, ascending postileal
The Appendix: Not just vestigial
- Contributes to gut microbiome homeostasis
- Mucus-rich biofilm houses resident bacteria
- Acts as a microbial “sanctuary”
- Repopulates gut after diarrheal illness
- Sheds bacteria at 2–3 mL/day
Epidemiology: By the Numbers
- Lifetime risk: 8.6% in men, 6.7% in women
- 0.2% of Italian population (120,000 cases per year)
- 36,980 appendectomies per year in Italy (2023)
- Historically > 90% underwent appendectomy- 42% decrease in appendectomies since 2011
- Mortality <1% (but ≥5% in elderly)
Classic pathogenesis model
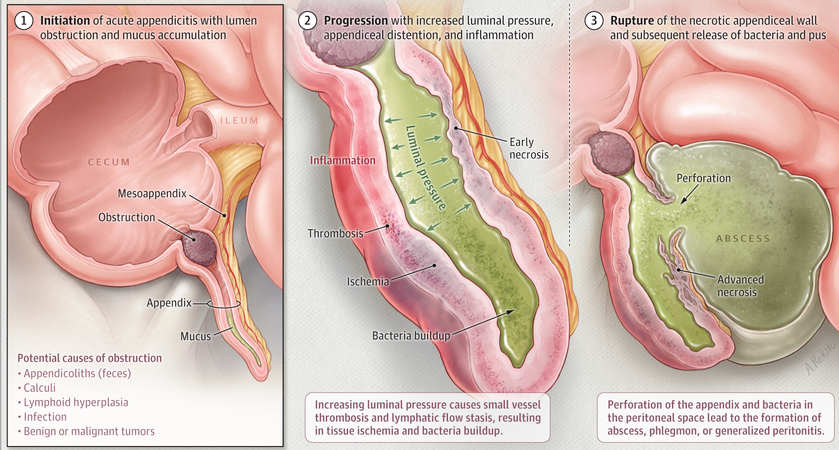
- Luminal obstruction (fecaliths, foreign bodies, tumor)
- Mucus accumulation → increased intraluminal pressure
- Lymphatic/vascular compression
- Ischemic mucosal damage
- Microbial invasion and inflammation
- Gangrene → perforation (if untreated)
Challenging the classic pathology model

- Fecaliths found in only a minority of cases
- Medical (antibiotic) treatment alone is effective in many patients
- Alternative etiologies proposed:
- Infectious agents
- Dietary fiber deficiency
- Microbiome dysbiosis
- Genetic susceptibility
- Environmental factors
The dietary fiber hypothesis

- Short’s observation (early 20th century): UK vs. Africa comparison
- Burkitt’s hypothesis: fiber as bulking agent reduces risk
- Fiber prevents fecalith formation and impaction
- Microbiome influenced by dietary fiber content
- Interest in diet–microbiome–appendicitis axis growing
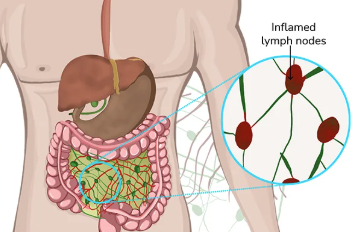
Mimics of appendicitis: Mesenteric adenitis
Classic clinical presentation
- Early: Colicky, visceral periumbilical pain
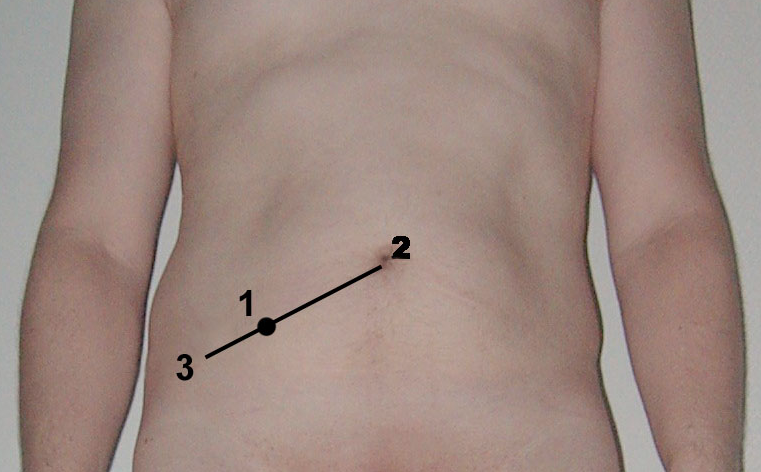
- 6–24 hours: Migration to RLQ (somatic pain)
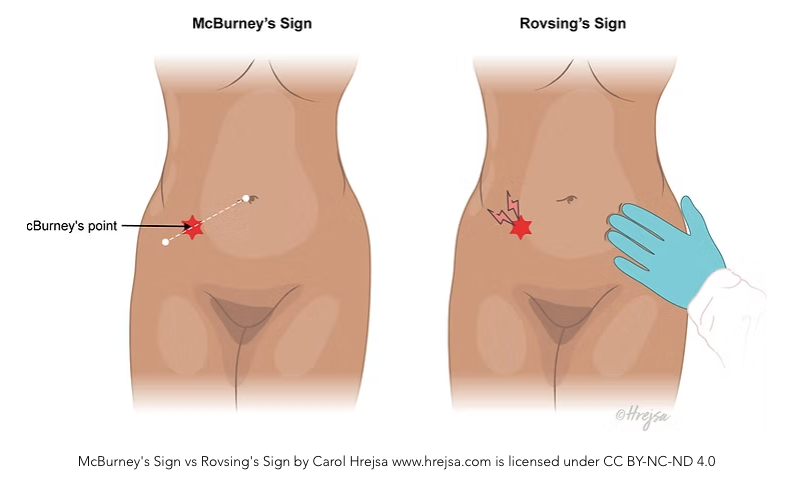
- Pain at McBurney point (anterior appendix)
- Associated: low-grade fever, anorexia, nausea, vomiting
Rovsing sign
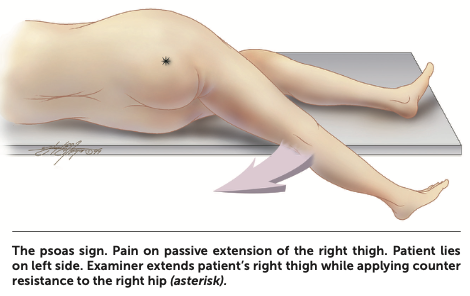
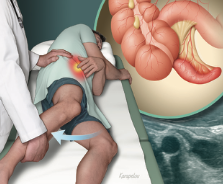
Psoas sign
 |
 |
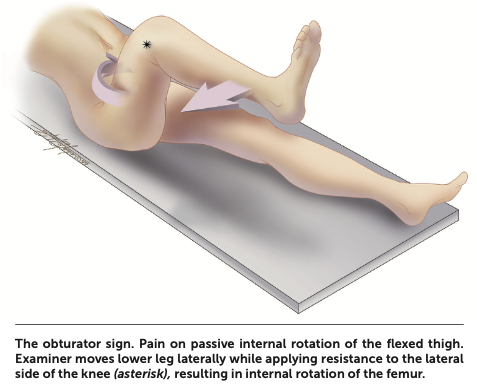
Obturator sign
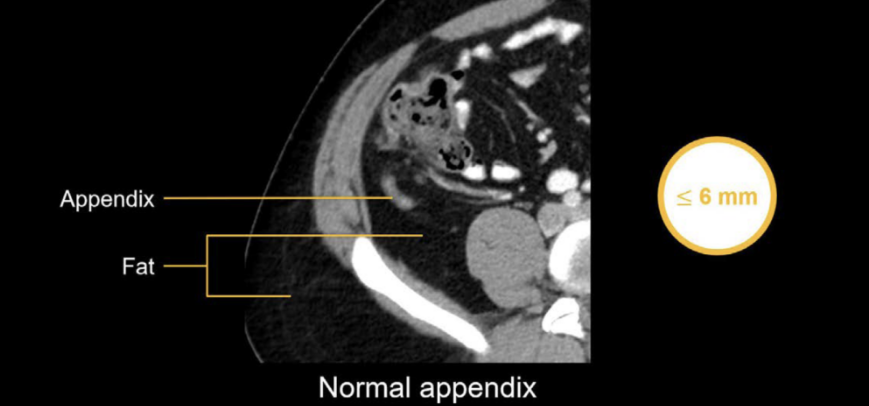
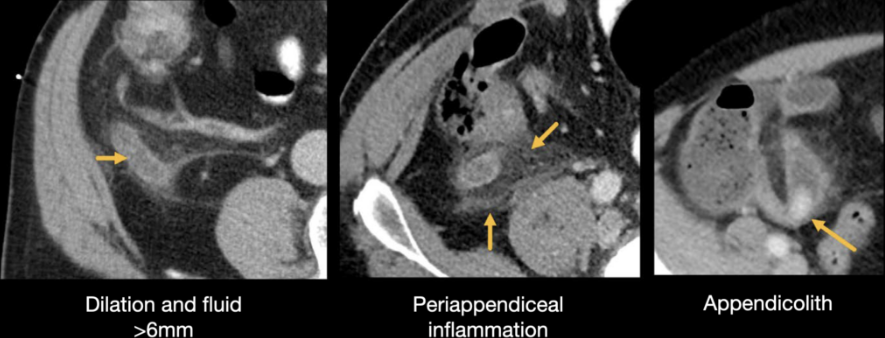
CT Imaging: Normal vs. abnormal
Treatment: Surgical
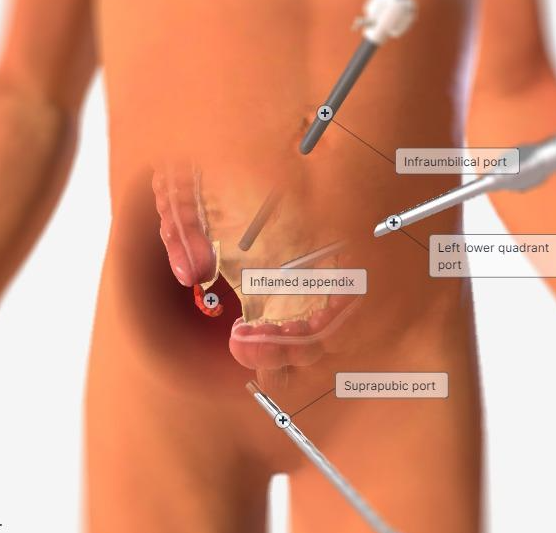
- Laparoscopic appendectomy:
standard of care- Shorter hospital stay
- Less postoperative pain
- Lower wound infection rates
- Open appendectomy: reserved for complex cases
- Interval appendectomy: considered after initial conservative management of appendiceal abscess
An uncomplicated surgery?

E. histolytica vs. E. dispar
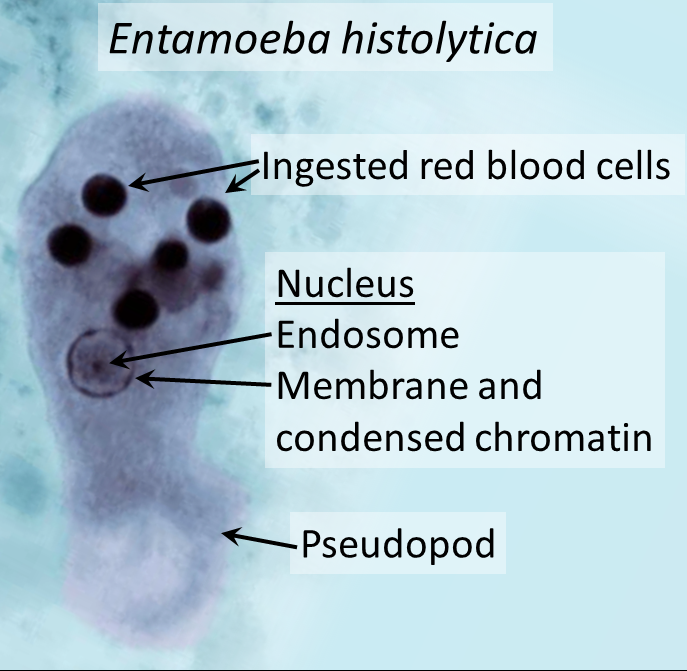
- E. dispar: nonpathogenic, colonizes 5–25% of persons
- E. dispar has no propensity for invasive disease
- Cannot distinguish by microscopy
- In industrialized countries: most Entamoeba = E. dispar
- In endemic regions: E. histolytica may predominate
Pathogenesis: Amebic liver abscess
- Ingestion of E. histolytica cysts
- Excystation in intestinal lumen
- Trophozoites migrate to colon
- Adhere via Gal/GalNAc lectin
- ~10% develop symptomatic colitis
- Portal spread to liver in <1% of cases
- Apoptosis of hepatocytes → abscess formation
.svg)
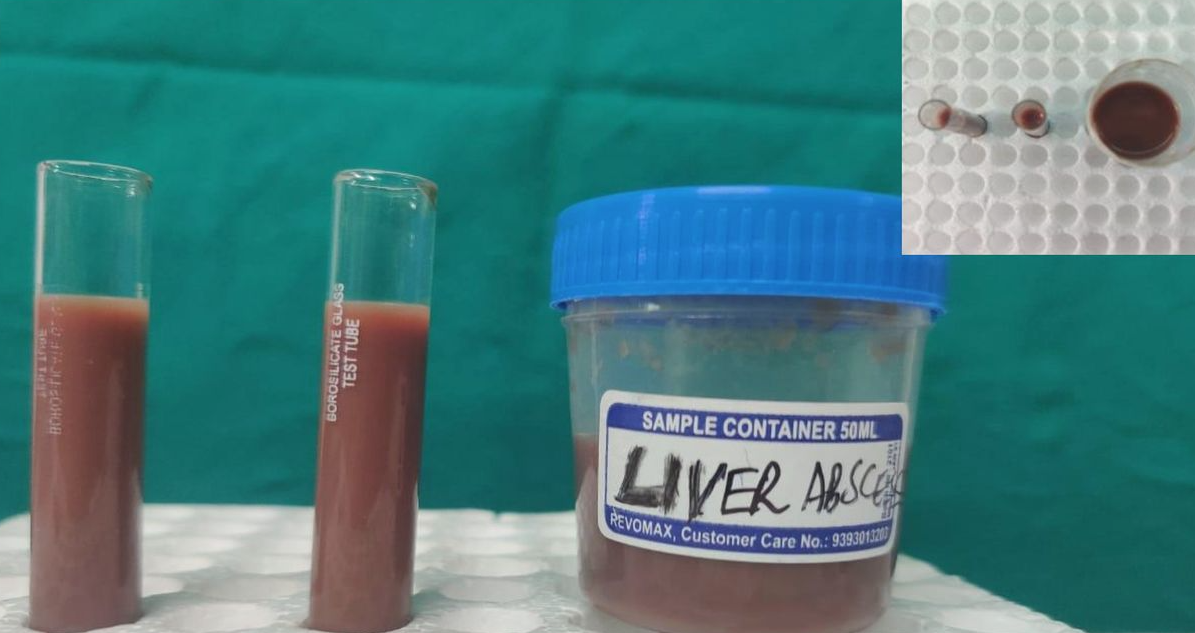
“Anchovy paste” from liver abscess
Epidemic Klebsiella pneumoniae liver abscess
First noted in Taiwan in mid-1980s
Monomicrobial, often in diabetics
No biliary tract disease
Now accounts for 80% of cases in Asia
- Spreading globally - Capsular serotypes K1 and K2

Mucoid phenotype demonstrated by loop test
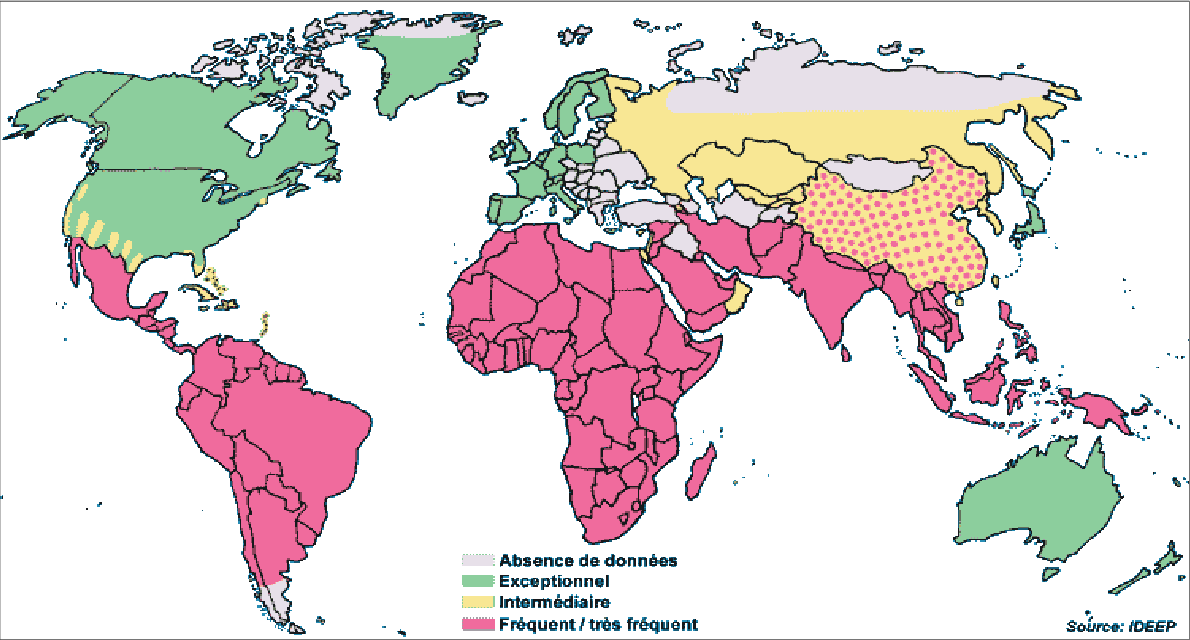
Endemic areas for amebic liver abscess
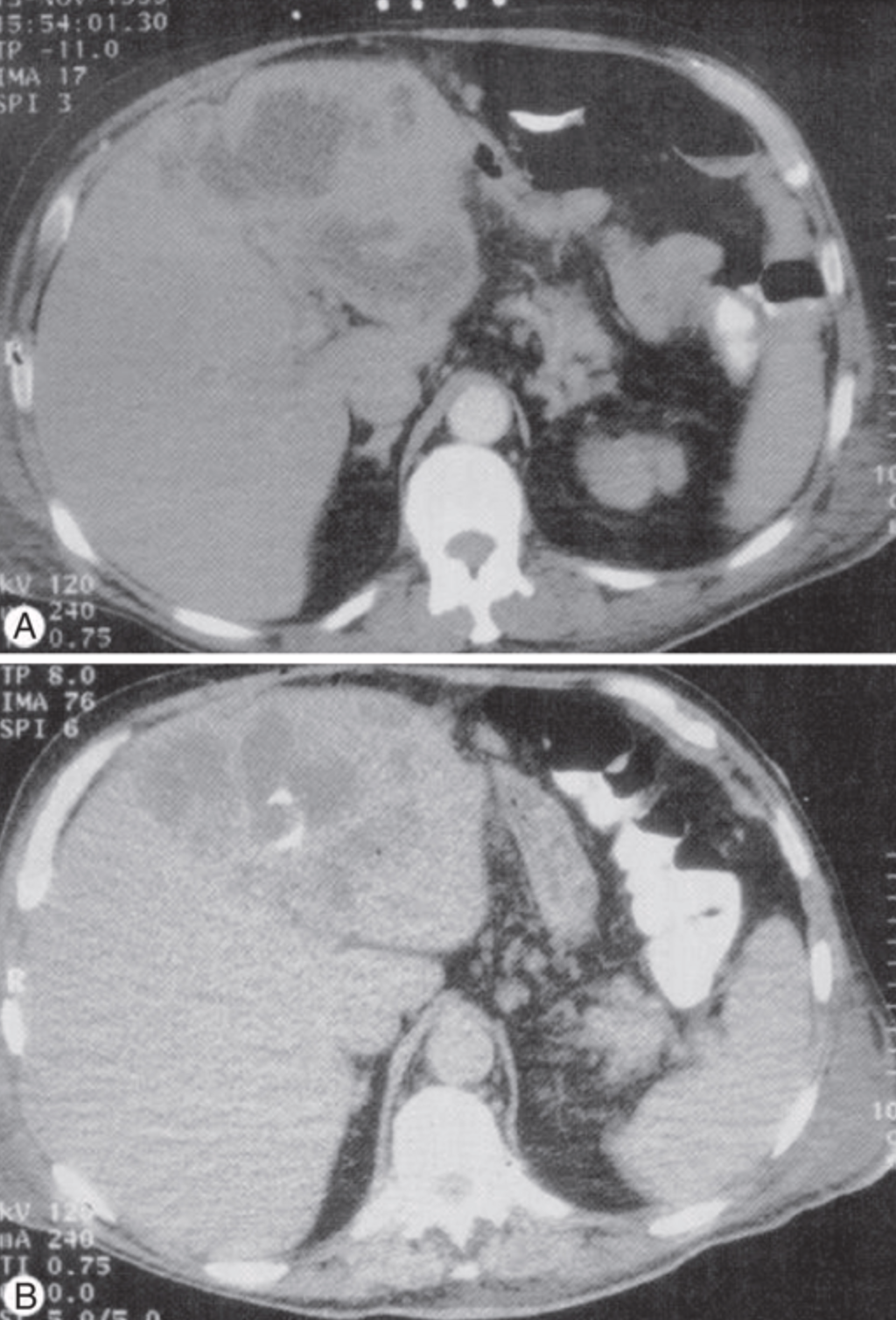
Diagnosis CT imaging
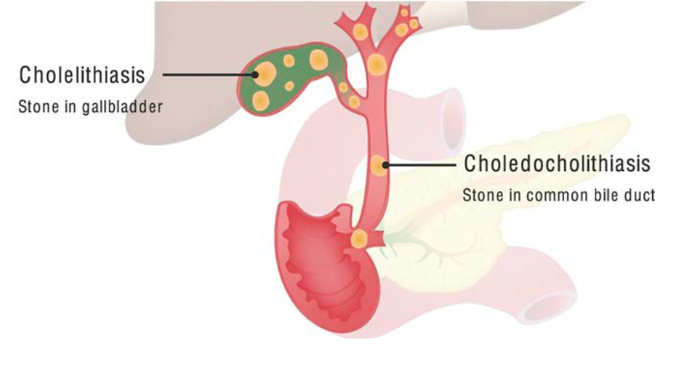
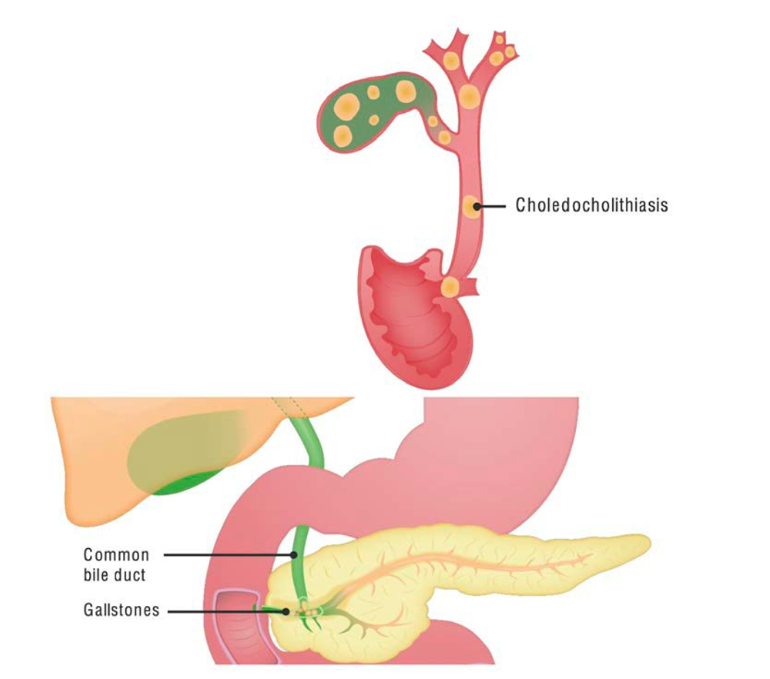
Biliary system infections: Overview
Infections associated with
obstruction to bile flowGallstones: common and usually asymptomatic
1% to 4% complicated by acute cholecystitis
Over 100,000 cholecystectomies per year in Italy
2–15% of cases are acalculous cholecystitis
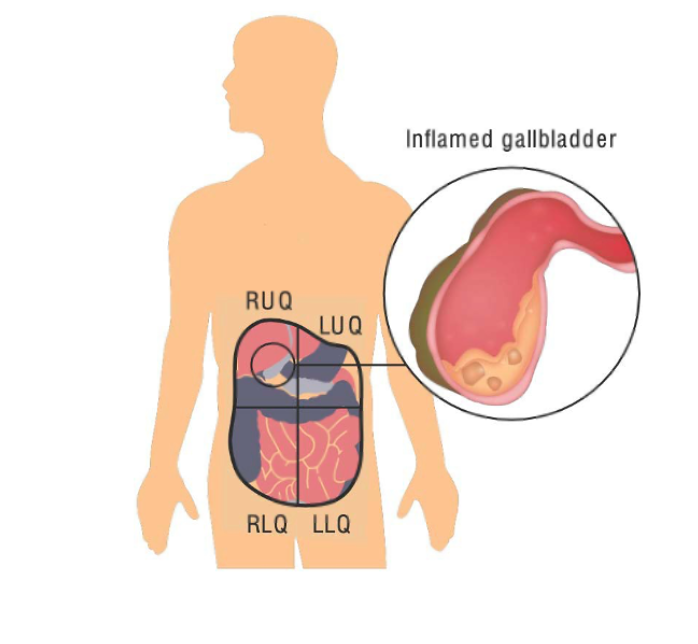
Cholecystitis: Key points
- Inflammation/bacterial infection of the gallbladder
- Usually from obstructing gallstones
- Acalculous cholecystitis: similar process without stones
- Treatment: cholecystectomy + antibiotics
- Mortality higher in acalculous cases
Cholangitis: Key points
- Inflammation/infection of the bile ducts
- Charcot triad: fever, jaundice, RUQ pain
- Reynolds pentad: Charcot triad + hypotension + altered mental status (sepsis)
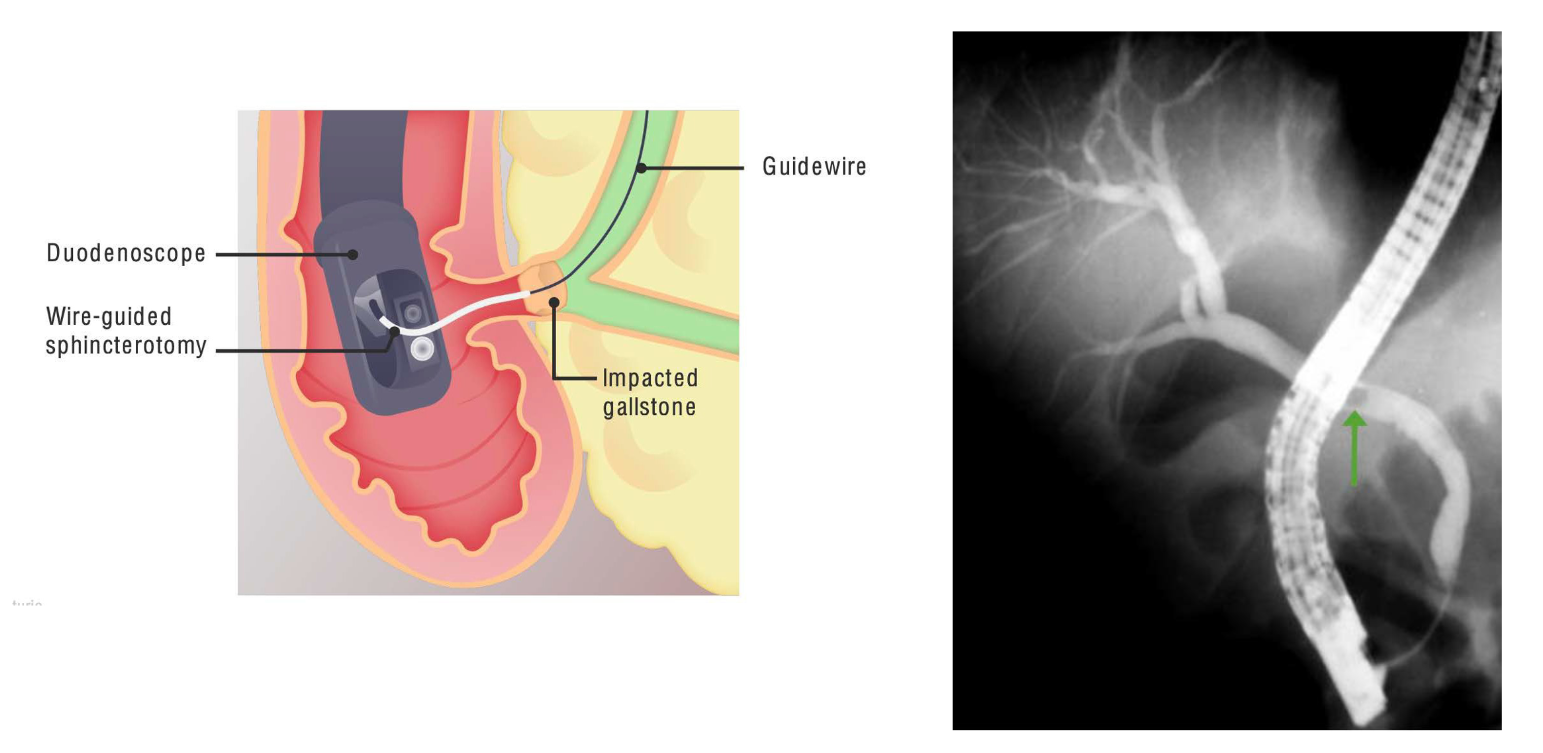
- Life-threatening emergency requiring urgent biliary decompression
not an encapsulated infection and will spill over to abdomen and bloodstream - Mortality: 5–10% with treatment; up to 90% without surgical and antibiotic treatment
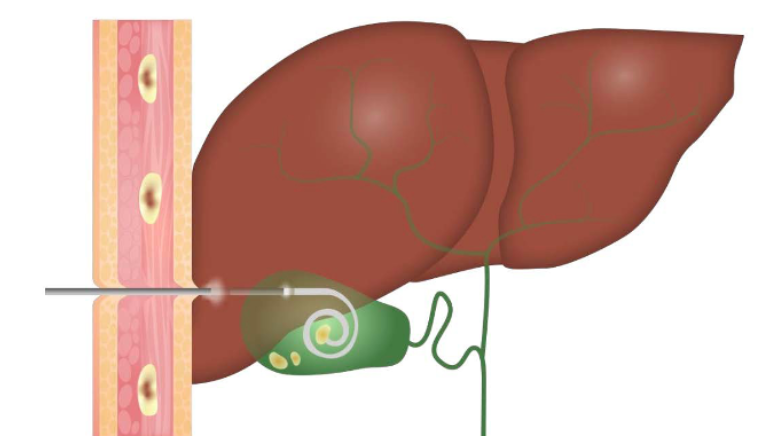
ERCP or percutaneous transhepatic drainage