Immunosuppression: An overview of infection risk
2026-03-01
Immununosuppression:
An Overview of Infection Risk
Prof. Russell E. Lewis
Department of Molecular Medicine
University of Padua
russelledward.lewis@unipd.it
https://github.com/Russlewisbo
slides available at: www.padovaid.com
 |
Defining net state of immunosuppression
“Father” of transplant infectious diseases”

“Composite of host factors, underlying disease, treatment, and other factors contributing to infection risk”
SOT Recipients
- 6% died from infection within first year (Swiss cohort) (Delden et al., 2020)
- 55% had infections in first year (German renal cohort) (Sommerer et al., 2022)
- Half occurred in first 3 months
- Bacteria: 66%, Viruses: 29%, Fungi: 5%
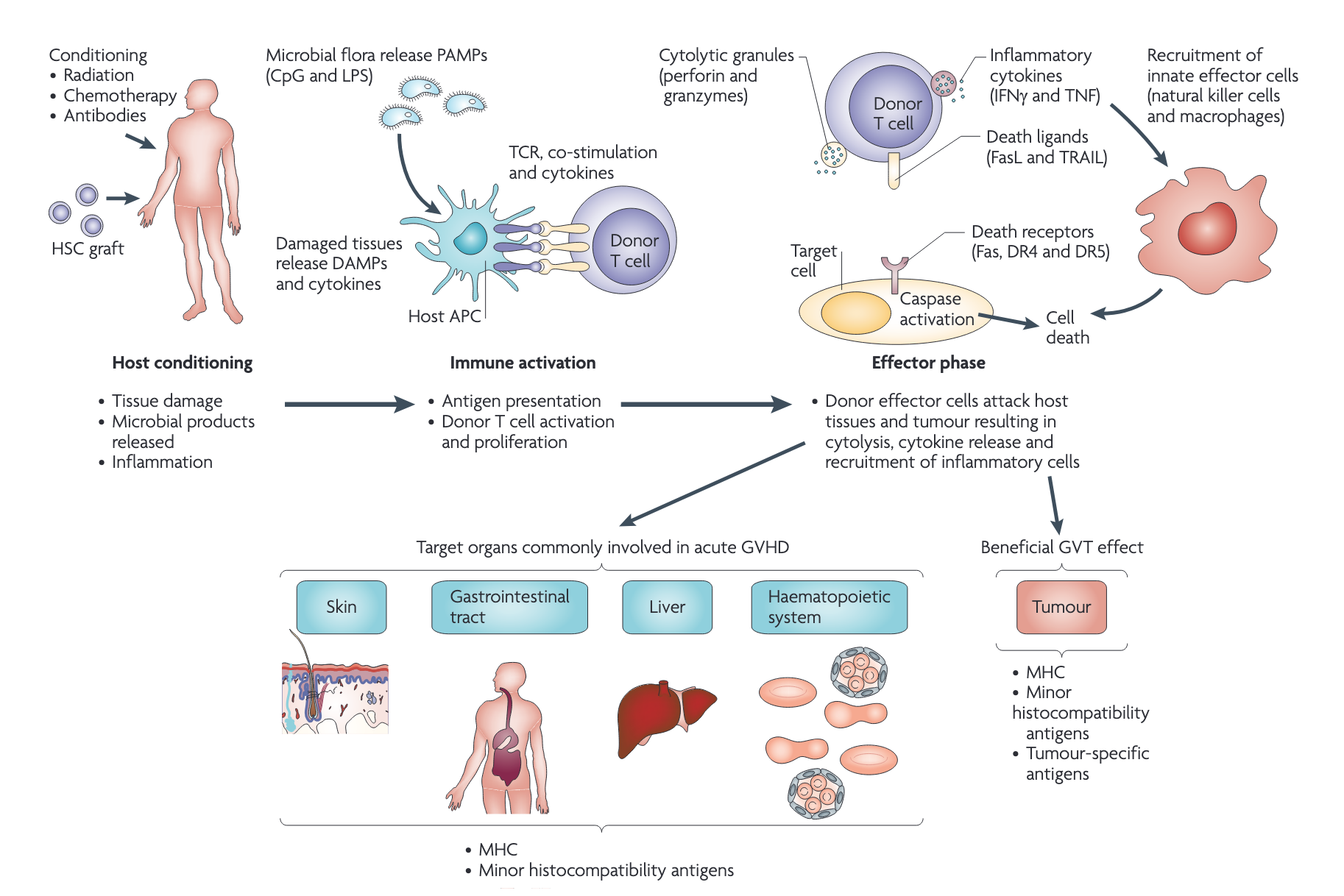
Allogeneic hematopoetic stem cell
transplantation (HSCT) recipients
What is CAR-T therapy?
%20T%20Cell%20Therapy_%20Vein-to-Vein%20Process.png)
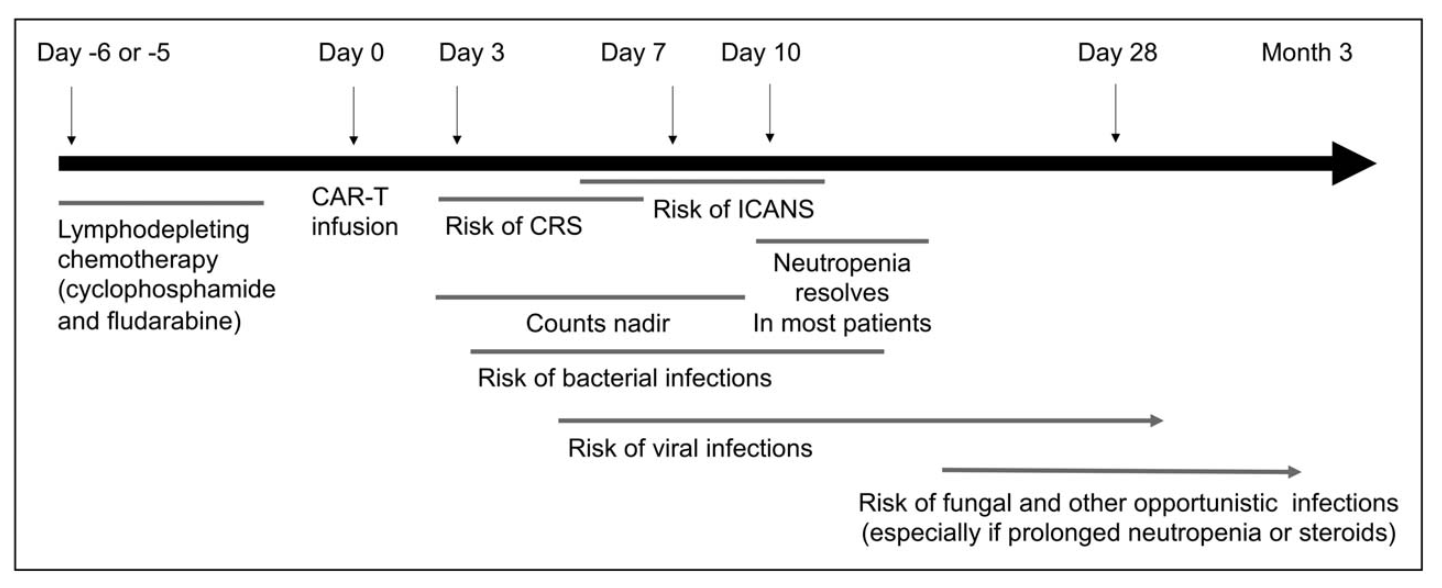
Immunosuppression timeline with CAR-T
Emerging biomarkers
- Viral reactivation (EBV, CMV, TTV, BK) → correlates with immunosuppression
- QuantiFERON Monitor → may identify over-immunosuppression
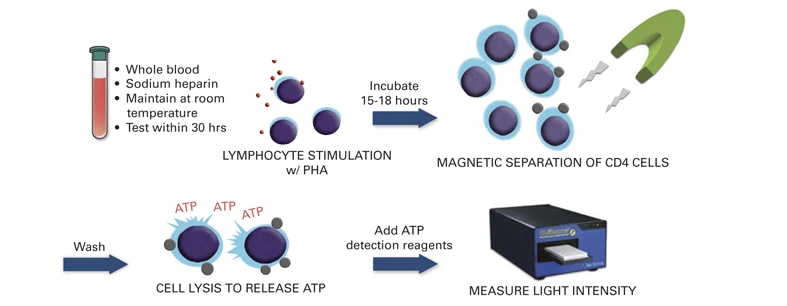
- ImmuKnow assay → correlates with infection/rejection risk
- Traditional markers (ESR, CRP, procalcitonin) → NOT predictive
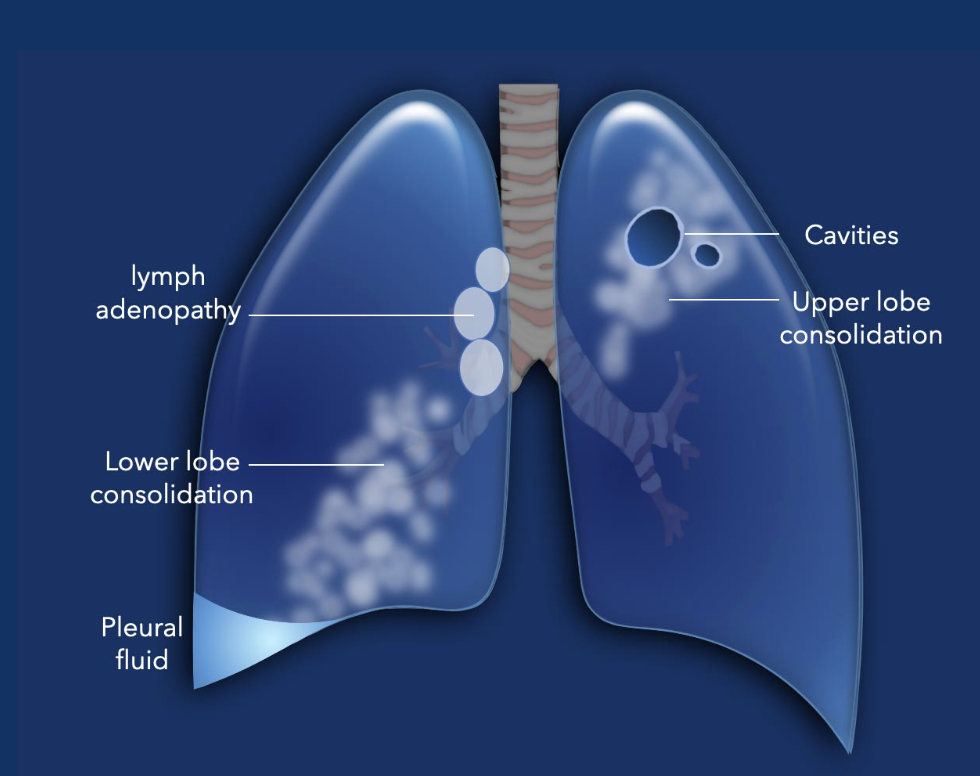
Reactivation of latent infections
Key pathogens to screen for and monitor:
- Mycobacterium tuberculosis
- Strongyloides
- Hepatitis B
- Coccidioides, Histoplasma
- Trypanosoma cruzi (Chagas)
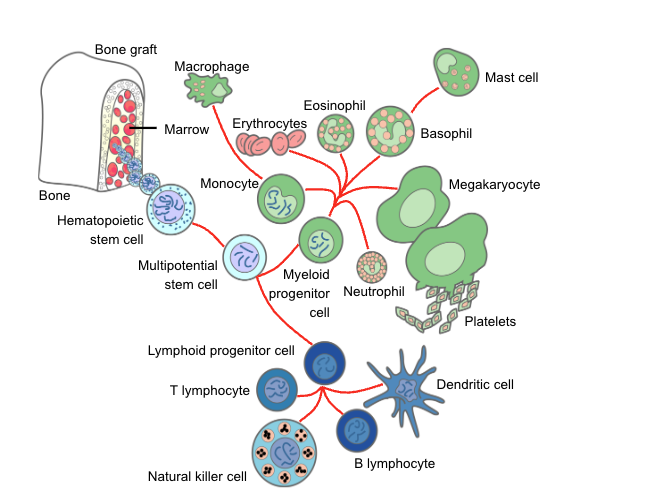
Granulocytes (neutrophils)
Chemotherapy & radiation → neutropenia
Duration: 3-4 weeks or longer
Primary risk factor for infection
Risk increases with:
- Depth of neutropenia
- Duration of neutropenia
Concurrent organ dysfunction
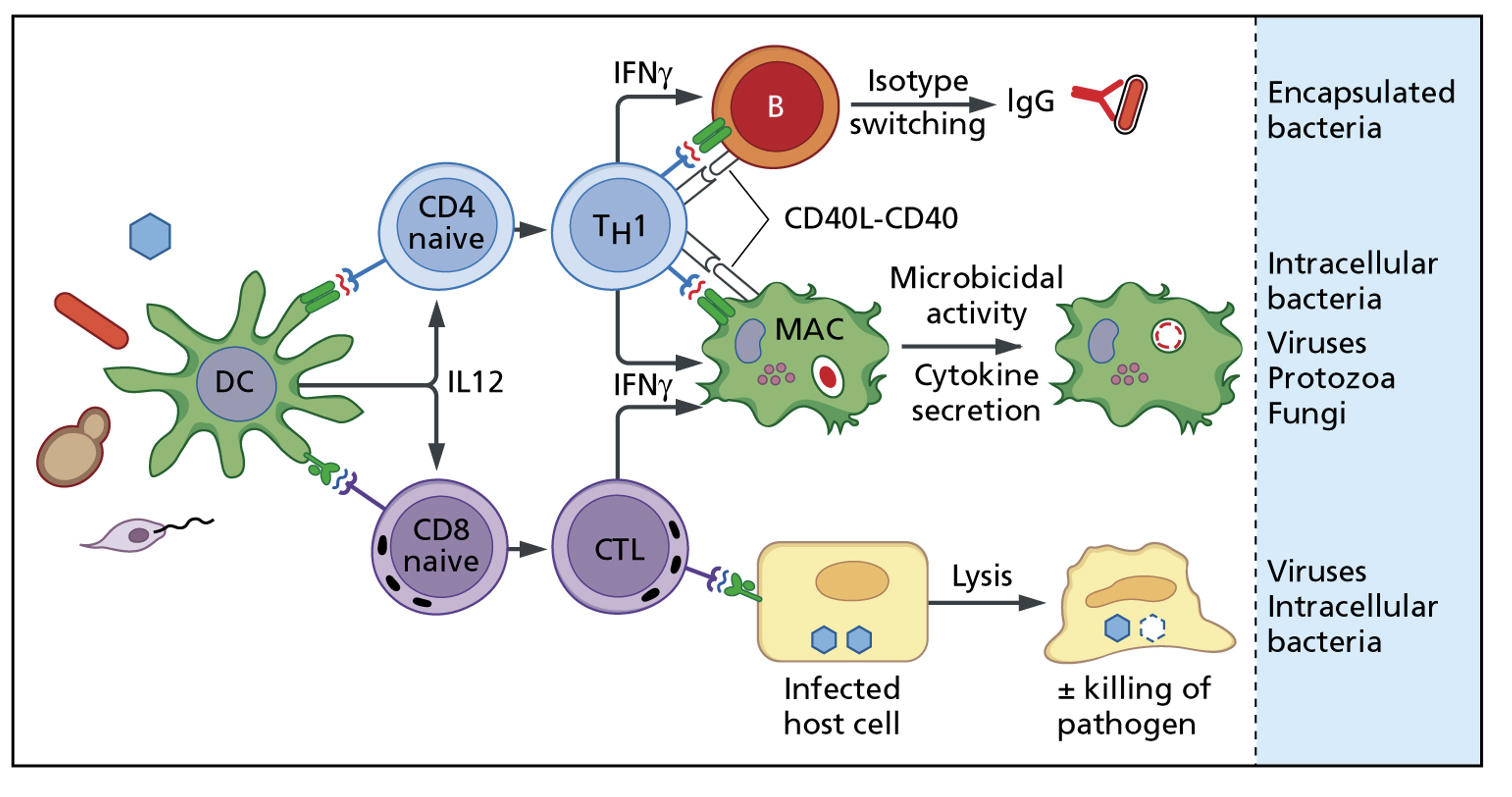
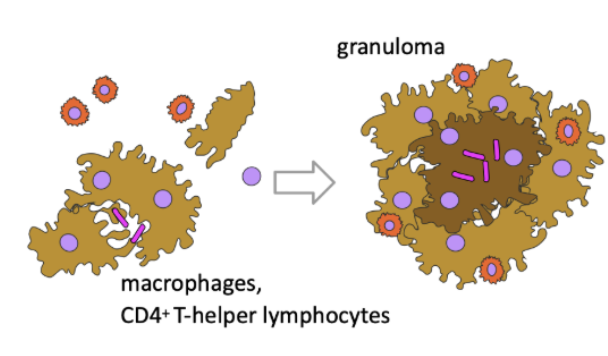
Specific cell-mediated immune defects:
Th1 and CTL-driven immunity
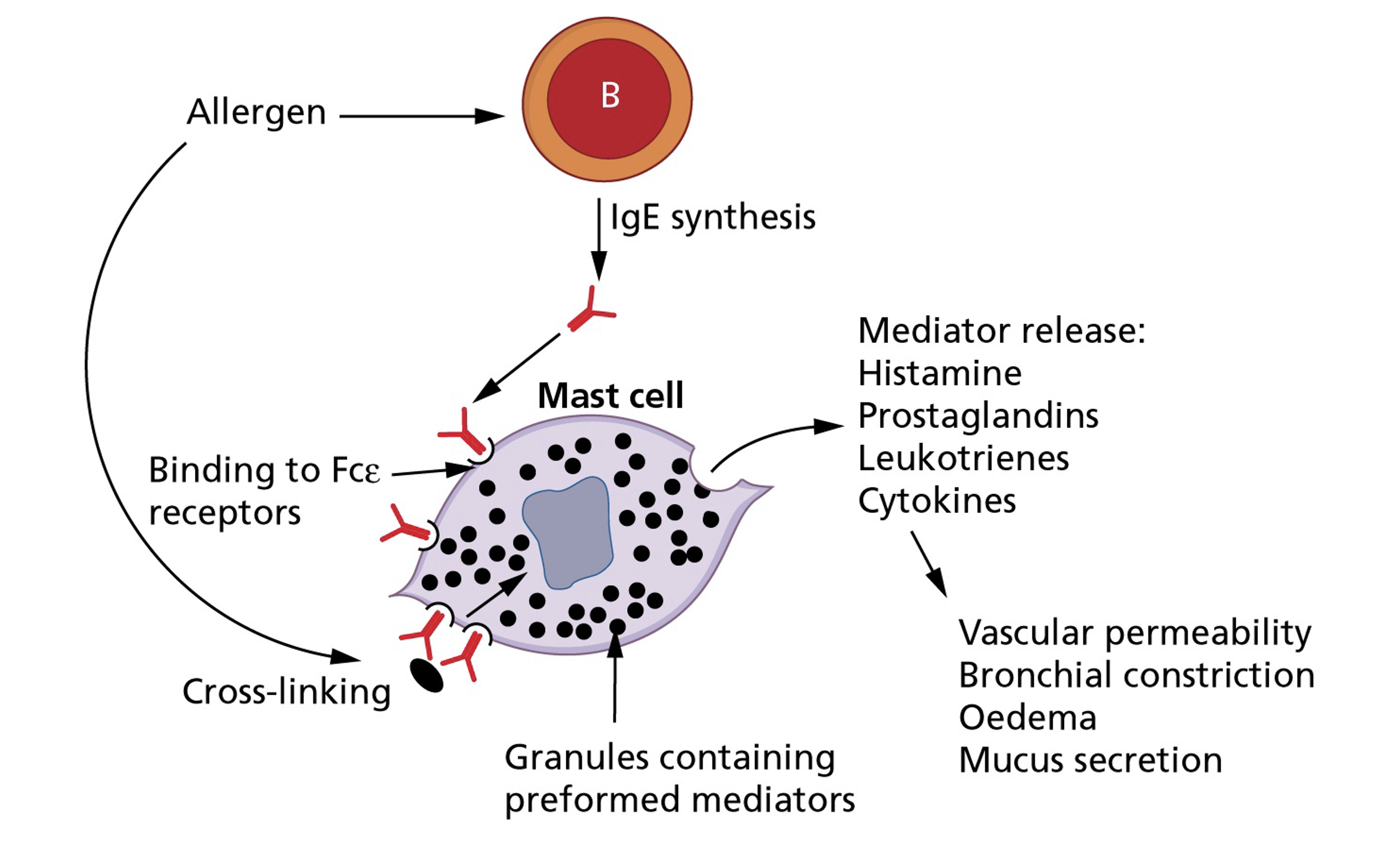
Specific cell-mediated immune defects:
Th2 and CTL-driven immunity
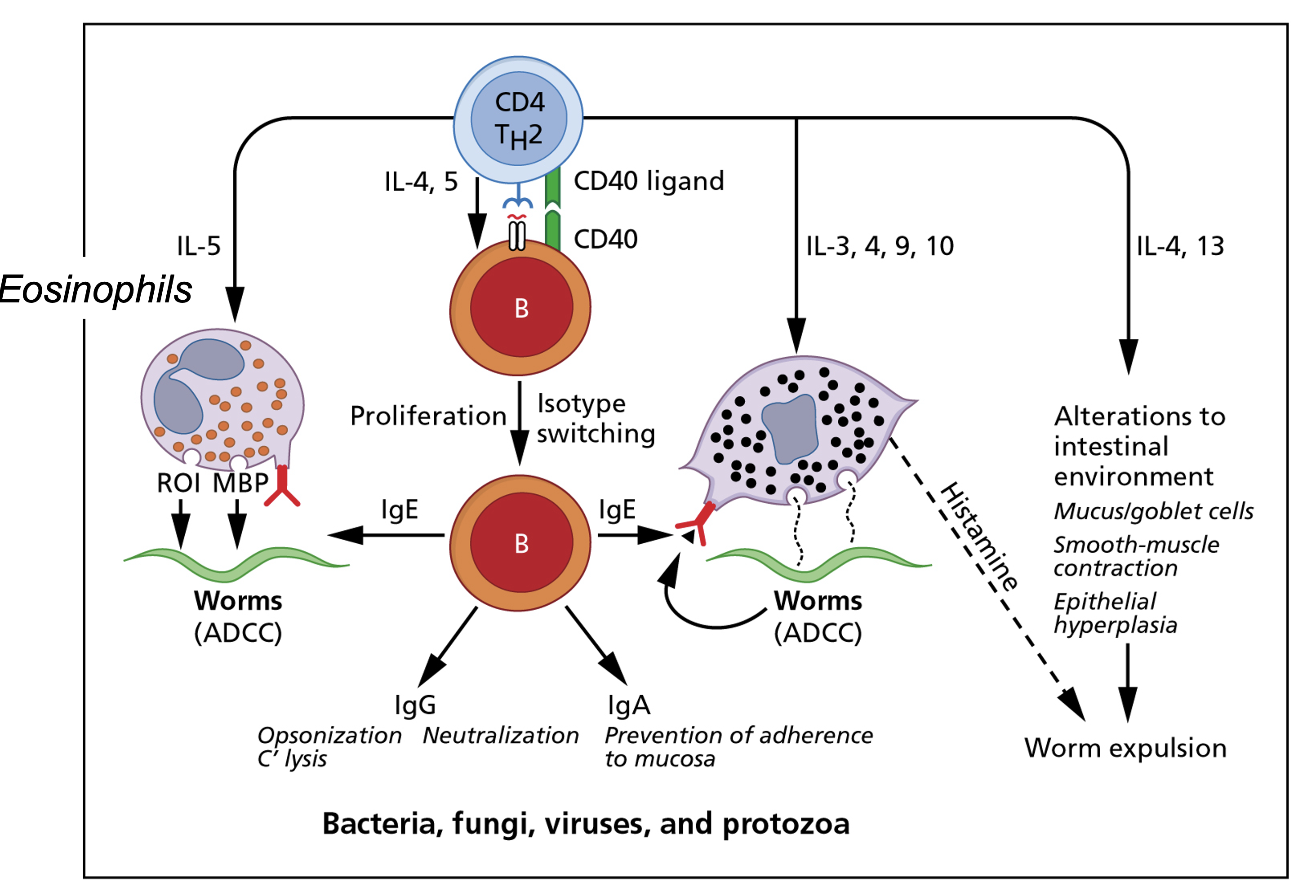
Cell-mediated driven allergy
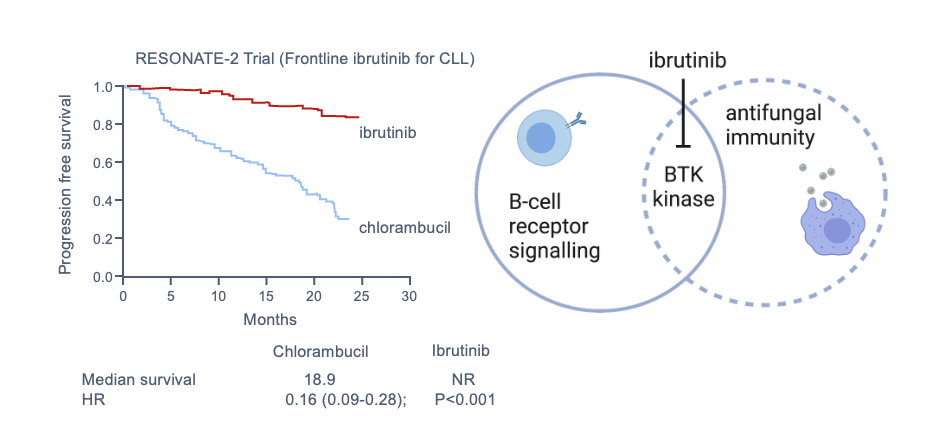
Ibrutinib
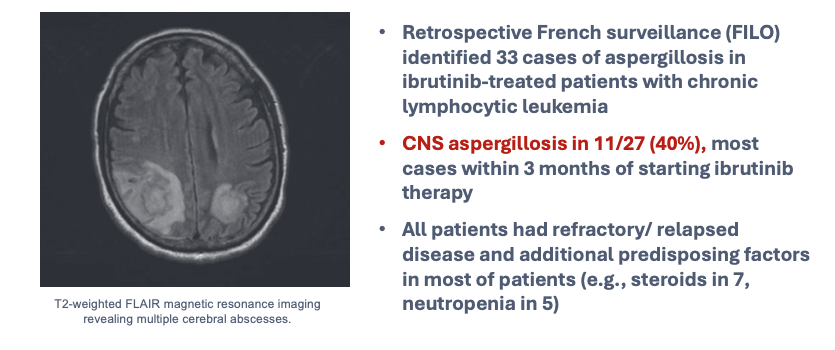
Unexpected fungal infections
The Integument
Skin:
- Chemotherapy → hair loss, dryness
- Catheters → direct microbial access
- Broken skin → S. aureus, gram-negatives
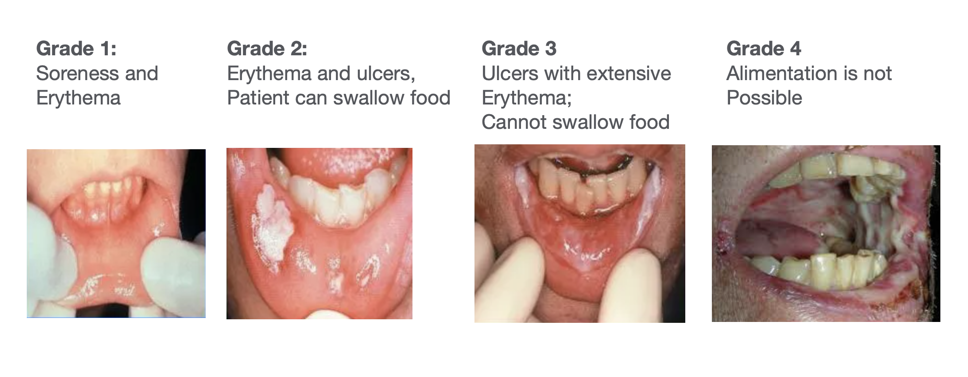
Oropharynx:
- Xerostomia + antibiotics → thrush, bacterial overgrowth

Alimentary Tract
- Microbiome disruption with antibiotics→ C. difficile
- Mucosal barrier injury from chemotherapy
- Facilitates bacterial translocation
- With concomitant neutropenia allows progression to sepsis
Impaired cellular immunity
Bacteria/Mycobacteria:
Listeria monocytogenes
Nocardia spp.
M. tuberculosis
Nontuberculous mycobacteria
Fungi/Parasites:
P. jirovecii
Aspergillus spp.
Cryptococcus spp.
Toxoplasma gondii
Impaired cellular immunity (viruses)
- Herpesviruses (HSV, VZV, CMV, EBV)
- Respiratory viruses
- Polyomaviruses (BK, JC)
- Human papillomavirus
Impaired humoral immunity
- Streptococcus pneumoniae
- Haemophilus influenzae
- Neisseria meningitidis
- Norovirus
- Hepatitis B virus
