Glycopeptides and lipopeptides
2026-06-10
Glycopeptide and Lipopeptide Antibiotics
Russell E. Lewis, Pharm.D., FCCP
Associate Professor of Infectious Diseases

russelledward.lewis@unipd.it
Slides and course materials: www.idpadovaid.com
Learning objectives
By the end of this lecture, you should be able to:
- Compare the mechanisms of action of the five glycopeptide / lipoglycopeptide agents and explain how structural differences translate into different spectra
- Recognise the molecular basis of VRE, hVISA, VISA, and VRSA and the clinical implications of each
- Apply AUC-guided vancomycin dosing principles and identify candidates for alternative agents
- Choose appropriately between vancomycin, teicoplanin, and the lipoglycopeptides for specific clinical scenarios
- Anticipate and manage the toxicities and assay-interference of telavancin, dalbavancin, and oritavancin
Class overview
Five agents, one core mechanism
| Vancomycin | Teicoplanin | Telavancin | Dalbavancin | Oritavancin | |
|---|---|---|---|---|---|
| Class | Glycopeptide | Glycopeptide | Lipoglycopeptide | Lipoglycopeptide | Lipoglycopeptide |
| Year approved | 1958 | 1988 (EU) | 2009 | 2014 | 2014 |
| Half-life | 6–12 h | 70–100 h | ~8 h | ~346 h | ~245 h |
| US availability | Yes | No | Yes | Yes | Yes |
| Italy availability | Yes | Yes | No | Yes | Yes |
Mechanism of action
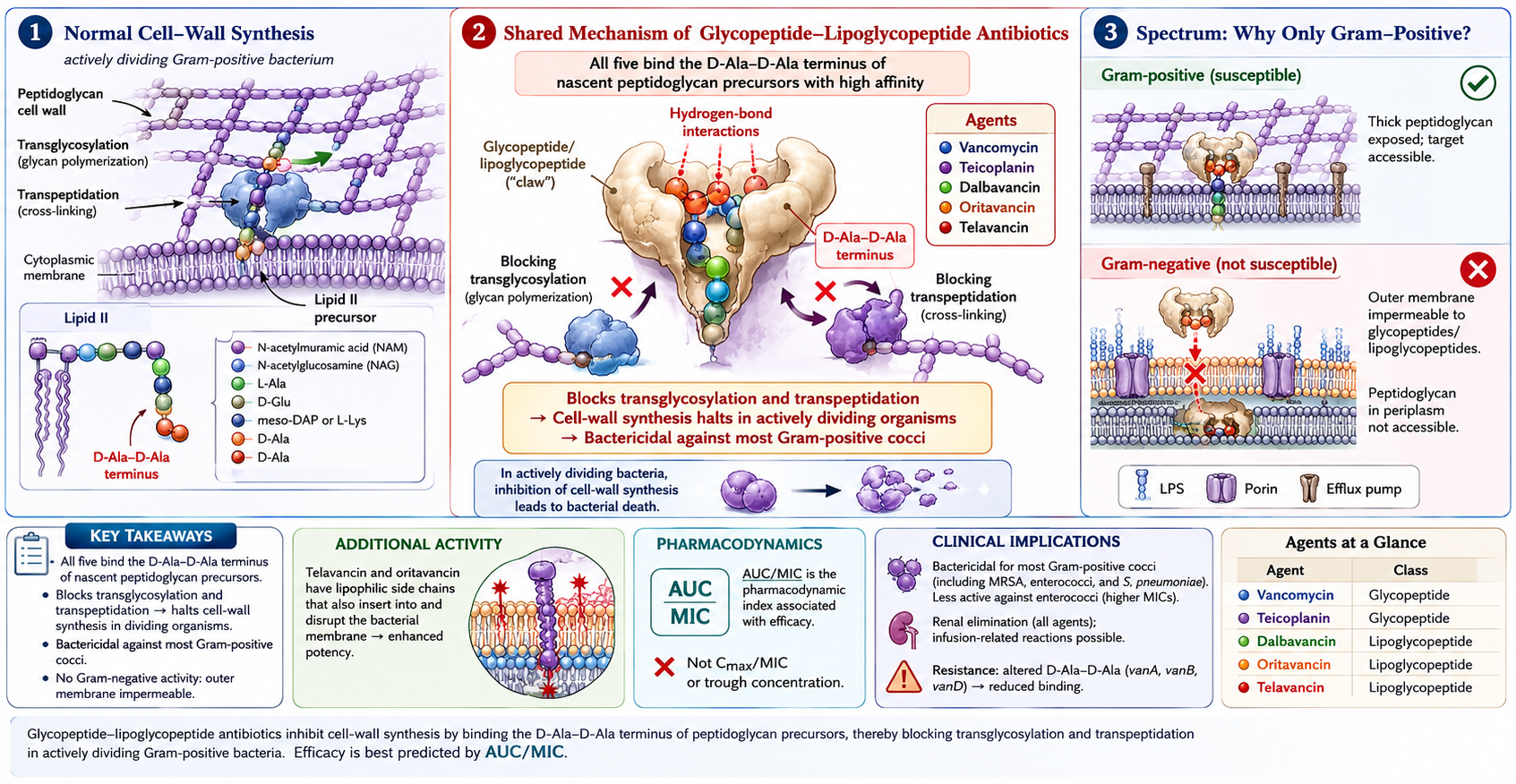
How glycopeptides bind D-Ala-D-Ala
- Five hydrogen bonds between the glycopeptide peptide backbone and the terminal D-Ala-D-Ala carbonyl/amino groups
- Binding affinity: KD ≈ 10⁻⁶ M for vancomycin
- This molecular “lid” sterically blocks transglycosylase and transpeptidase access
- Substitution to D-Ala-D-lactate (VanA, VanB, VanD, VanM) removes one critical H-bond → affinity ↓ ~1000×
- Substitution to D-Ala-D-serine (VanC, VanE, VanG) reduces affinity ~7×
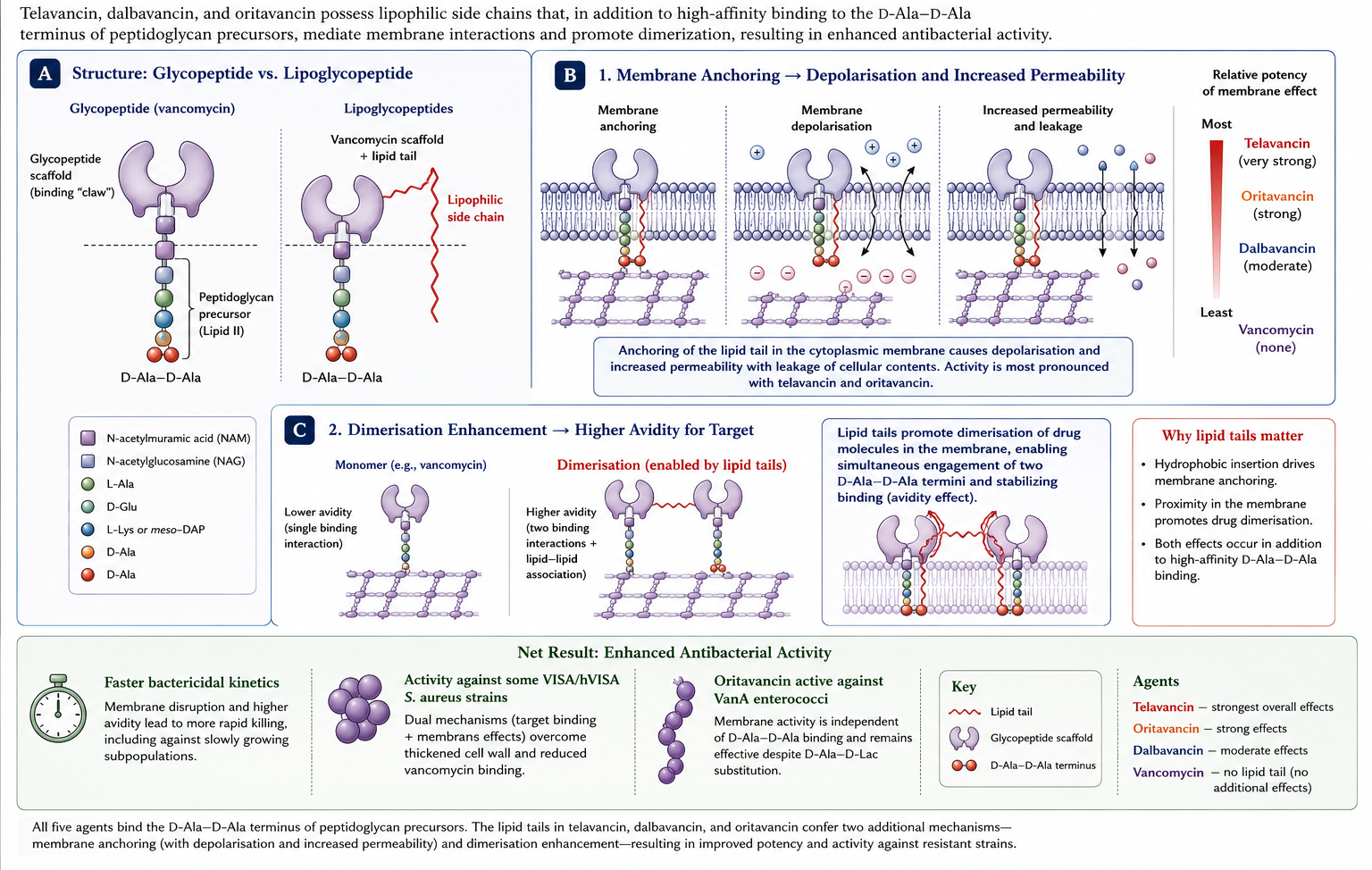
Why lipoglycopeptides act differently
Vancomycin
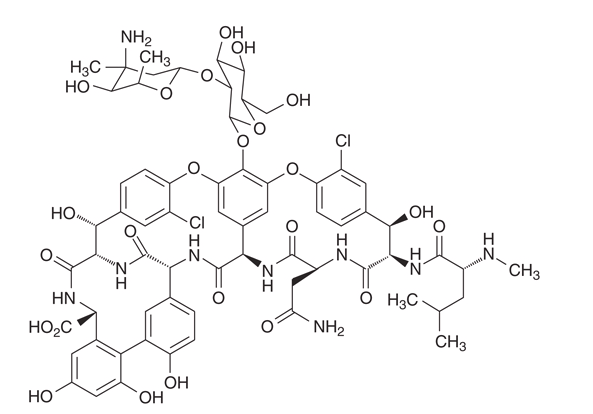
Vancomycin structure
- Tricyclic glycopeptide, MW ~1,449 Da
- Heptapeptide backbone + two attached sugars (vancosamine, glucose)
- Peptide backbone binds D-Ala-D-Ala via five hydrogen bonds
- High-affinity binding defines class activity but limits target flexibility
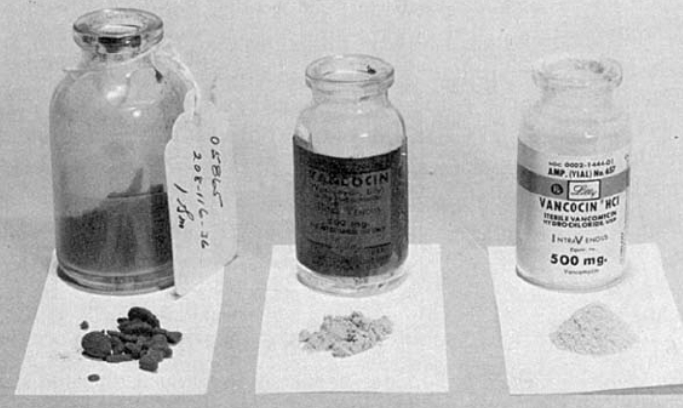
A potted history
- Isolated 1953 from Amycolatopsis orientalis in Borneo soil
- FDA approval 1958 for penicillin-resistant S. aureus
- Early lots: “Mississippi mud” — impurities caused ototoxicity and nephrotoxicity
- Use dropped after methicillin (1960) and the new β-lactams arrived
- Re-emergence in the 1980s with rising MRSA prevalence → use went from ~2 tonnes/yr (1984) to >11 tonnes/yr (1996) in the US alone
Vancomycin spectrum
Active against (gram-positives, dividing):
- Staphylococcus aureus — MSSA, MRSA, hVISA (partially), VISA (reduced)
- Coagulase-negative staphylococci
- Streptococci (groups A–G, S. pneumoniae, viridans)
- Enterococci (susceptible strains; VRE = resistant)
- Listeria monocytogenes, Corynebacterium jeikeium
- Clostridioides difficile, Cutibacterium acnes
Not active: gram-negatives, mycobacteria, fungi
Vancomycin tissue penetration
| Tissue | Penetration | Notes |
|---|---|---|
| Lung epithelial lining fluid | ~20% serum | Lower than linezolid (~415%) |
| Bone | ~10–30% | Variable; consider higher doses |
| CSF (inflamed meninges) | 7–21% | Inadequate without inflammation |
| Vitreous humour | <5% | Need intravitreal for endophthalmitis |
| Synovial fluid | ~70% | Adequate for septic arthritis |
| Skin / soft tissue | ~30–40% | Adequate for typical ABSSSI MICs |
→ Limitations underlie use of adjunctive intraventricular, intraperitoneal, intravitreal routes.
Vancomycin resistance — VRE
VRE epidemiology
- Globally widespread, predominantly VanA and VanB phenotypes in Enterococcus faecium
- NHSN data (US, 2011–2014): VRE accounted for 28% of HAI enterococcal isolates
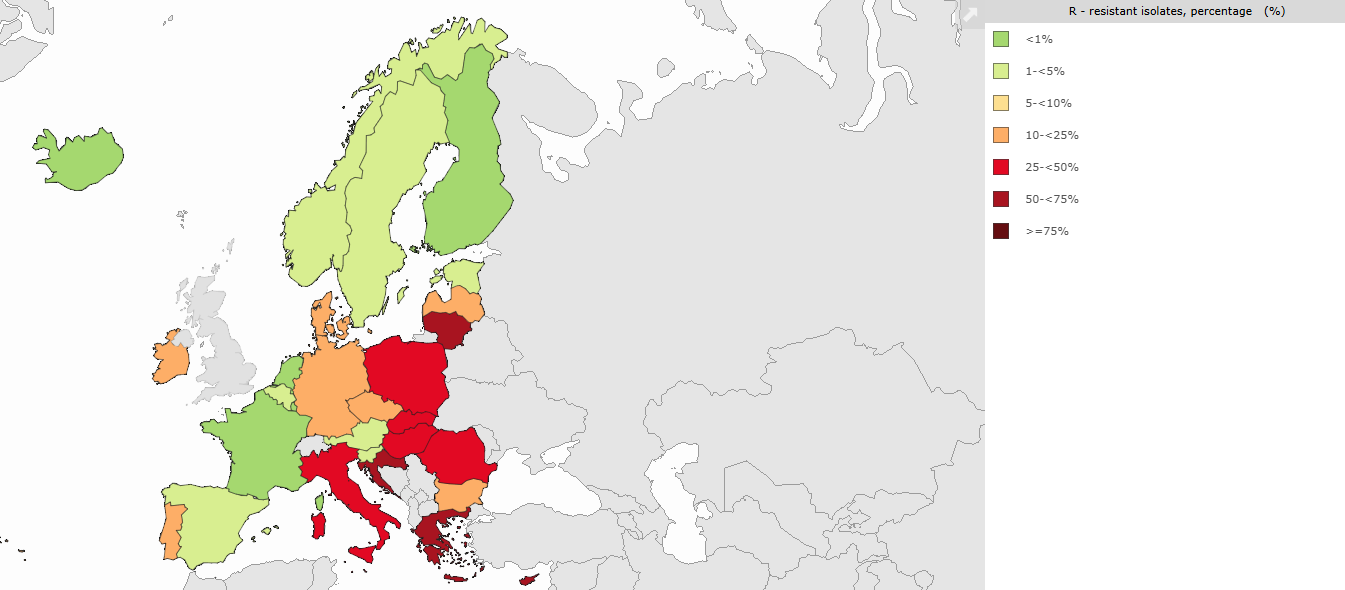
- EARS-Net 2019 (EU): enormous regional variation — <1% (Nordic) to >50% (some Eastern European countries) for E. faecium
- Latin America VENOUS-I cohort: dominant clones differ from US/EU
EARS-Net data
Vancomycin-resistant Enterococci in Europe
VRE mechanisms — the van gene clusters
| Operon | Resistance level | Vancomycin | Teicoplanin | Substrate |
|---|---|---|---|---|
| VanA | High | R | R | D-Ala-D-lactate |
| VanB | Variable | R | S | D-Ala-D-lactate |
| VanC (intrinsic) | Low | R | S | D-Ala-D-serine |
| VanD, VanM | High | R | R | D-Ala-D-lactate |
| VanE, VanG, VanL, VanN | Low | R | S | D-Ala-D-serine |
The key trick: substitution of D-Ala-D-Ala with D-Ala-D-lactate or D-Ala-D-serine at the peptidoglycan terminus reduces vancomycin affinity by ~1000-fold (lactate) or ~7-fold (serine).
VDE — vancomycin-dependent enterococci
- Rare but described: enterococci that require vancomycin to grow
- Mechanism: loss of endogenous D-Ala-D-Ala ligase; rely entirely on vancomycin-induced D-Ala-D-Lac ligase
- Practical impact: undetectable on routine media without vancomycin
- Can revert to vancomycin-independent
Vancomycin resistance — staphylococci
hVISA, VISA, VRSA — the definitions
| Strain | MIC | Mechanism | Frequency |
|---|---|---|---|
| Susceptible | ≤2 μg/mL | Wild type | Majority of S. aureus |
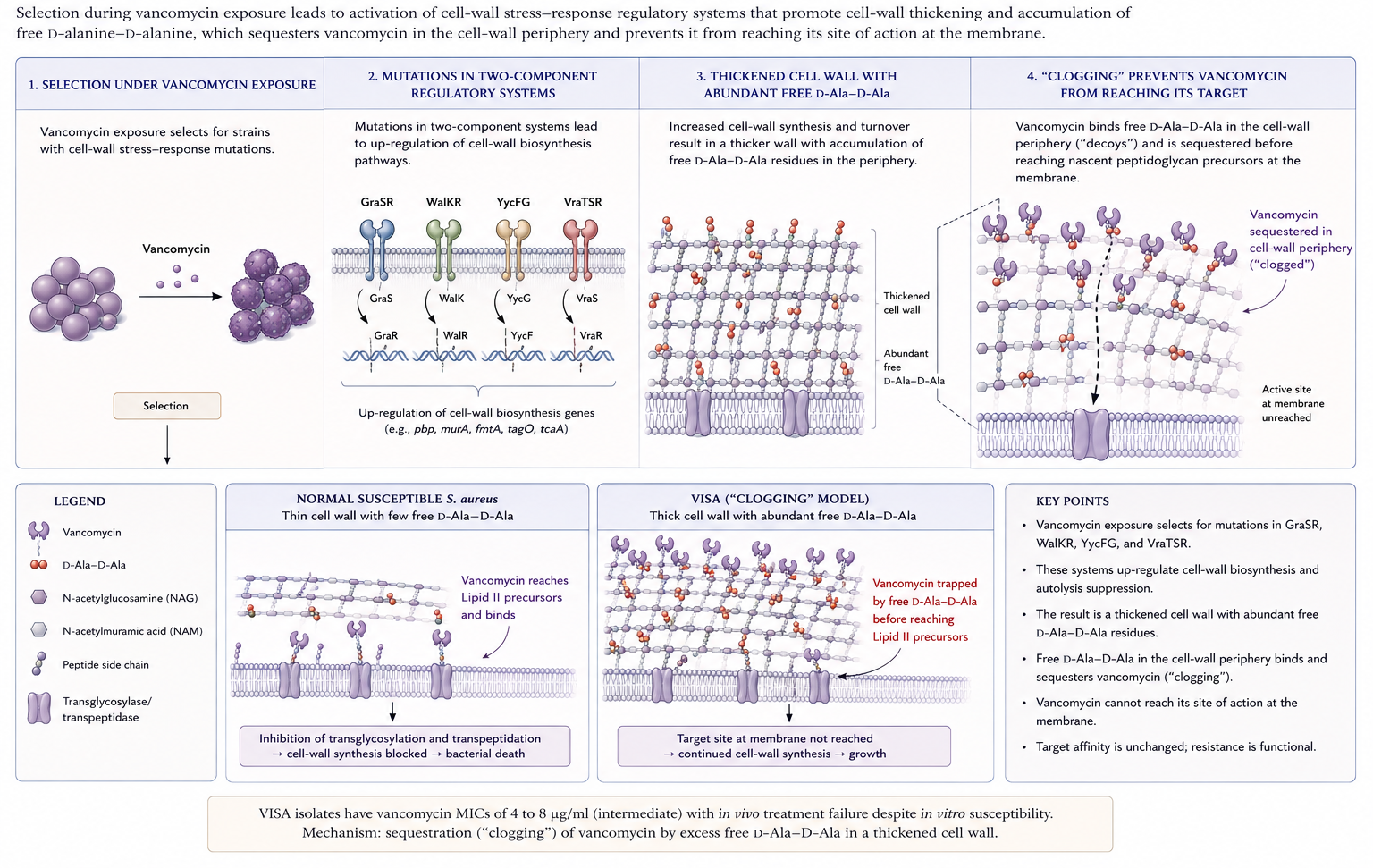
| hVISA | ≤2 (population); 4–8 (subpopulation) | Cell wall thickening; TCS mutations (GraSR, WalKR, VraTSR) | ~6% global pooled prevalence |
| VISA | 4–8 μg/mL | Same as hVISA, more pronounced | <0.5% globally |
| VRSA | ≥16 μg/mL | Acquired vanA operon from VRE | ~16 confirmed cases in US through 2023 |
VISA mechanism — the “clogging” model
VRSA — the rare event
- Acquisition of the enterococcal vanA operon by MRSA, usually in patients with concomitant VRE infection
- Conjugative transfer in vivo demonstrated experimentally and in clinical isolates
- First US case 2002; total ~16 confirmed US cases as of 2023
- No confirmed cases in Italy?
- Most isolates: high-level resistance (MIC ≥32 μg/mL) but susceptible to linezolid, daptomycin, ceftaroline, oritavancin
MIC “creep” and clinical failure
- Multiple cohorts: MRSA bacteraemia with vancomycin MIC at the upper end of susceptibility (1.5–2 μg/mL by Etest) linked to higher failure, persistence, and mortality
- Cochrane meta-analysis confirmed association but emphasised heterogeneity of testing methods
- IDSA 2011 MRSA guidelines: consider alternative agent if persistent bacteraemia despite adequate exposure OR MIC >2 μg/mL
Vancomycin PK/PD
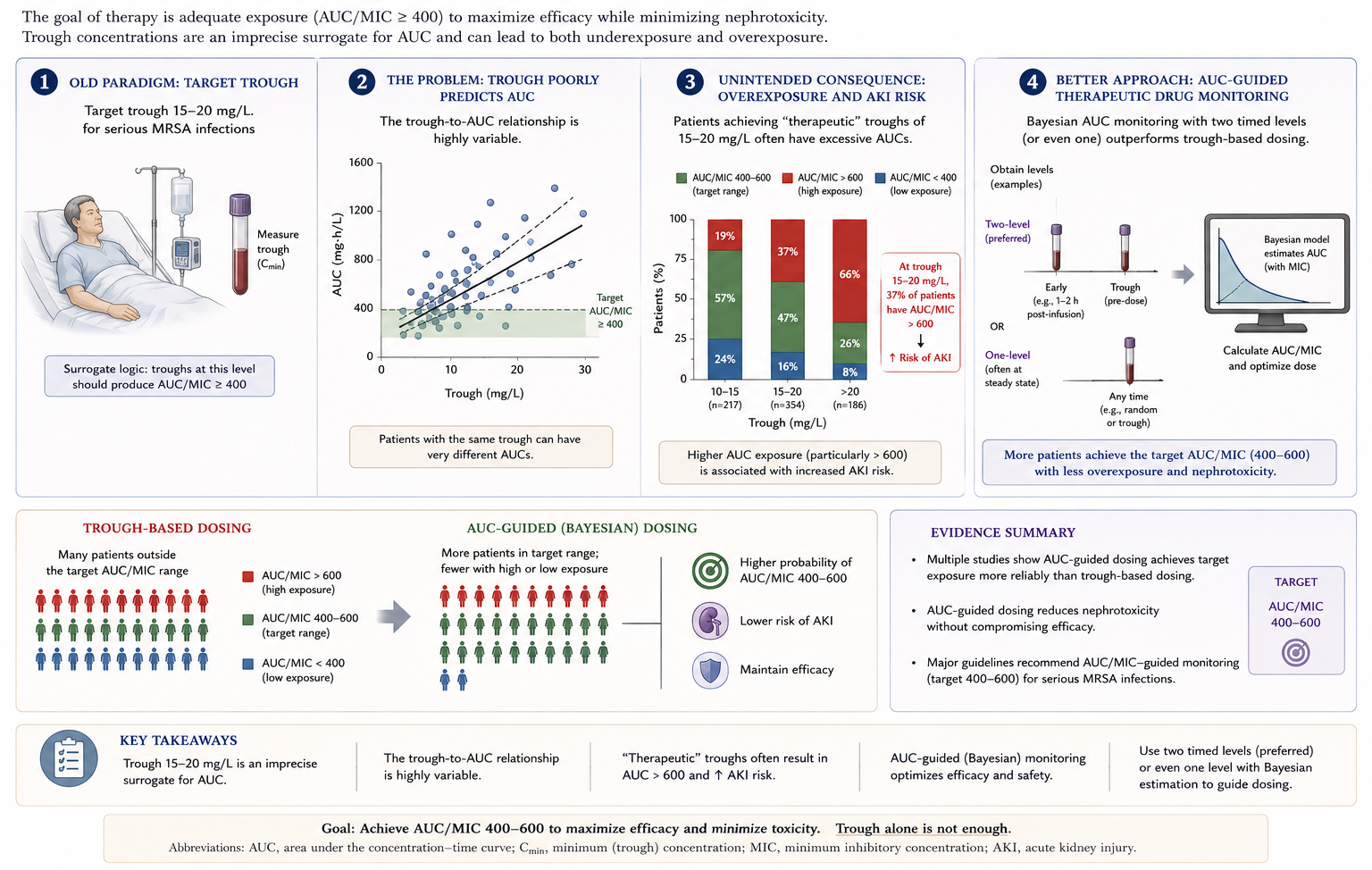
Pharmacodynamic target: AUC/MIC ≥ 400
- In vivo and clinical data: AUC₂₄ / MIC ≥ 400 correlates with clinical response and microbiologic eradication in MRSA
- AUC > 600 mg·h/L correlates with nephrotoxicity
- Therapeutic window for serious MRSA infections: AUC 400–600
Why trough monitoring isn’t enough
2020 ASHP/IDSA/PIDS/SIDP guidelines — key points
- For serious MRSA infections (bacteraemia, endocarditis, pneumonia, meningitis, osteomyelitis):
- AUC₂₄ target 400–600 (assuming MIC ≤1 mg/L by BMD)
- Bayesian-derived AUC preferred; first-order equations from two timed concentrations acceptable
- Loading dose 25–30 mg/kg (actual body weight) for severely ill patients
- For non-serious infections: trough-based monitoring may still be acceptable
Vancomycin in special populations
- Neonates / VLBW infants: weight- and PMA-based dosing; AUC monitoring increasingly available; hearing screening recommended after prolonged courses
- Children: AUC₂₄ target 400–600 for serious MRSA; Bayesian tools especially useful given inter-patient variability
- Pregnancy: category B/C; minimal transplacental passage in ex vivo models; therapeutic fetal concentrations reached in overt amnionitis; no demonstrated teratogenicity in second/third trimester
- Obesity: dose by actual body weight, but cap loading at 3 g; obese patients often achieve higher AUC than non-obese at same mg/kg
- Elderly: heightened nephrotoxicity risk; use lower trough/AUC targets where clinically acceptable
The obesity dosing question comes up a lot. The current consensus is to dose by actual body weight with a cap, then monitor and adjust based on AUC. Older guidelines used adjusted body weight but that under-dosed many patients. Pregnancy data are reassuring for second/third trimester use but data on first-trimester exposure are sparse (Rybak et al., 2020).
Vancomycin dosing summary
| Population | Recommended dose | Comment |
|---|---|---|
| Adult, normal renal function | 15–20 mg/kg q8–12 h | Use actual body weight |
| Severe sepsis / endocarditis / meningitis | Loading 25–30 mg/kg → 15–20 mg/kg q8–12 h | Loading ≤500 mg/h |
| Continuous infusion | 30–40 mg/kg/day after 15 mg/kg loading | Lower AKI; equivalent efficacy |
| HD (after session) | Load 25 mg/kg → 7.5–10 mg/kg (low-perm) or 10–15 mg/kg (high-perm) | Adjust to predialysis level 15–20 mg/L |
| CRRT (CVVH/CVVHD) | Load 20 mg/kg → 500 mg q8h | Increase for effluent >35 mL/kg/h |
| Children | Weight-based; AUC-targeted | Bayesian tools especially useful |
Local administration
- Intraperitoneal (CAPD peritonitis): 15–30 mg/kg in long dwell (≥6 h) every 5–7 days
- Intraventricular (ventriculitis, shunt infection): 5 mg (slit ventricles), 10 mg (normal), 15–20 mg (enlarged); reduce 60% in infants
- Intraocular (endophthalmitis): 1 mg intravitreal
- Oral (C. difficile): 125 mg q6h × 10 days (fulminant: 500 mg q6h + IV metronidazole)
Vancomycin adverse effects
Vancomycin infusion (red-man) syndrome

- Rapid erythematous flushing of head, face, neck, upper trunk during infusion
- Often with pruritus, occasionally hypotension/angioedema
- Mechanism: direct mast cell histamine release — not IgE-mediated
- Incidence 3.4–14% (higher in children, 14%)
- Risk factors: faster infusion rate, higher concentration, concurrent opioids/anaesthetics
- Management: stop infusion, antihistamine, restart at half rate (<10 mg/min)
Nephrotoxicity
Risk factors (additive):
- AUC > 650 mg·h/L (≈ trough ≥ 15 mg/L)
- Concomitant nephrotoxins, possibly piperacillin-tazobactam
- Duration >14 days
- Pre-existing renal disease, advanced age, obesity, sepsis, hypovolaemia
Mechanisms: oxidative tubular injury, immune-mediated interstitial nephritis, intratubular cast obstruction
Other adverse effects
- Ototoxicity: rare with modern preparations; cumulative dose- and duration-related; very-low-birthweight infants at higher risk
- Neutropenia: 1–2% short courses, 12–13% with prolonged therapy
- Thrombocytopenia: rare; can be immune-mediated
- Rash / drug fever: 3% / 2%; DRESS and SJS/TEN rare but reported
- Linear IgA bullous dermatosis: classic vancomycin association
- C. difficile colitis from IV vancomycin (paradoxically reported)
Preventing vancomycin AKI
- AUC-guided dosing with target 400–600 mg·h/L
- Avoid concomitant nephrotoxins (consider avoiding piperacillin-tazobactam — use cefepime or carbapenem if combination needed)
- Maintain euvolaemia; correct hypovolaemia before high-dose courses
- Reassess need for vancomycin daily; de-escalate if MRSA ruled out
- Consider continuous infusion in critically ill patients
- For high-risk patients, consider alternative agent (daptomycin, linezolid, ceftaroline) if MRSA confirmed
Vancomycin clinical uses
MRSA bacteraemia and endocarditis
- Vancomycin remains first-line when daptomycin not appropriate
- AUC-guided dosing; loading dose for severe disease
- Consider alternative agent if:
- Persistent bacteraemia ≥ 7 days despite adequate exposure
- MIC > 2 μg/mL
- Endovascular source not controlled
- Alternatives: daptomycin (high dose ≥8 mg/kg), ceftaroline, daptomycin + ceftaroline, dalbavancin (off-label)
MRSA pneumonia
- Vancomycin and linezolid both recommended first-line in IDSA/ATS HAP/VAP guidelines
- Linezolid: higher epithelial lining fluid concentration; reduced renal toxicity
- Most randomised trials: clinical equivalence
- For necrotising pneumonia or PVL-positive strains, linezolid often preferred (toxin suppression)
Persistent MRSA bacteraemia — alternatives
- Daptomycin ≥ 8 mg/kg (high-dose to reduce resistance emergence)
- Daptomycin + ceftaroline combination — synergy in vitro; observational survival benefit in persistent bacteraemia
- Daptomycin + β-lactam (oxacillin, nafcillin, anti-staphylococcal penicillin) — “seesaw effect”
- Ceftaroline monotherapy — option for daptomycin-non-susceptible
- Linezolid — “bacteriostatic,” generally not first choice for bacteraemia but role in refractory cases
- Investigational: oritavancin or dalbavancin for off-label bacteraemia / endocarditis continuation
VRE bacteraemia — treatment choices
| Agent | Pros | Cons |
|---|---|---|
| Linezolid 600 mg q12h | Oral option; effective; widely available | Bone marrow suppression with prolonged use; serotonin syndrome with SSRIs |
| Daptomycin ≥10 mg/kg | Bactericidal; once-daily | High doses needed; resistance emergence reported |
| Tigecycline | Activity vs VRE | Low serum levels; FDA mortality signal |
| Oritavancin | Single-dose; active vs VanA | Off-label; aPTT interference; cost |
| Quinupristin-dalfopristin | Active vs E. faecium (not faecalis) | IV only; arthralgia/myalgia; venous irritation |
Bacterial meningitis
- Empirical: vancomycin + 3rd-generation cephalosporin (cefotaxime or ceftriaxone) in adults
- Rationale: penicillin-resistant S. pneumoniae coverage
- Add ampicillin for Listeria if age >50 or immunocompromised
- Add dexamethasone for suspected pneumococcal meningitis
C. difficile infection
- Oral vancomycin 125 mg q6h × 10 days
- first-line for non-fulminant initial episode (IDSA/SHEA 2021)
- Fidaxomicin preferred when available (lower recurrence)
- Recurrent CDI: tapering/pulsed oral vancomycin OR fidaxomicin OR bezlotoxumab adjunct
- Fulminant disease: vancomycin 500 mg q6h PO + metronidazole 500 mg IV q8h ± rectal vancomycin
Teicoplanin- No longer available in EU
Teicoplanin — distinguishing features
- Glycopeptide complex from Actinoplanes teichomyceticus
- Lipophilic side chain → high protein binding (~90–95%), long half-life
- Spectrum largely overlaps vancomycin
- Higher MIC in some staphylococcal species (notably S. haemolyticus)
- VanA: resistant; VanB: susceptible (no induction)
- Not available in the United States **No role in Italy-Van A 95-96%.
Teicoplanin TDM — the critical detail
| Indication | Target trough (mg/L) | Loading regimen |
|---|---|---|
| Uncomplicated MRSA / soft tissue | 15–30 | 10 mg/kg q12h × 5 doses OR 12 mg/kg q12h × 3 doses |
| Complicated / serious MRSA (endocarditis, bone) | 20–40 | 12 mg/kg q12h × 5 doses |
| Non-MRSA, less serious | — | 6 mg/kg q12h × 3 doses |
Maintenance: 6 mg/kg/day after loading. Always load — half-life is too long to wait for steady state.
Teicoplanin — practical pearls
- Trough monitoring on day 4 (steady state after loading)
- Can be given IM bolus when IV access difficult
- Can give entire daily dose as slow bolus IV (no 60-minute infusion needed)
- Reduced red-neck syndrome vs vancomycin
- For VanB enterococcal endocarditis, teicoplanin remains a legitimate option
- Continued therapy at home (OPAT): once-daily dosing supports this
Teicoplanin clinical use cases
Where teicoplanin shines:
- Outpatient continuation therapy (once-daily dosing, IM or IV bolus possible)
- Patients intolerant of vancomycin (red-neck, less nephrotoxicity)
- VanB enterococcal infection
- Settings where AUC monitoring not feasible (trough-based TDM is simpler)
Caveats:
- Inferior to vancomycin in early endocarditis trials at low doses
- With aggressive loading and target-trough maintenance, modern outcomes comparable
Lipoglycopeptides
— the three newcomers
Three drugs, three personalities
| Telavancin | Dalbavancin | Oritavancin | |
|---|---|---|---|
| Parent compound | Vancomycin | A40926 (teicoplanin-like) |
Chloroeremomycin (vancomycin analog) |
| t½ | ~8 h | ~346 h (~14 d) | ~245 h (~10 d) |
| Dosing | 10 mg/kg q24h | 1000 mg + 500 mg/wk OR 1500 mg × 1 | 1200 mg × 1 |
| Renal adj. | Yes | No | No |
| Key activity gap | None vs VRSA | None vs VRSA | Active vs VRSA, VanA |
| Indications | ABSSSI, HAP/VAP | ABSSSI | ABSSSI |
| Coag assay issue | PT/aPTT/INR | None | aPTT × 5 days |
Telavancin
Telavancin mechanism and spectrum
- Vancomycin parent + decylaminoethyl tail (membrane-anchor) + phosphonomethylaminomethyl group
- Dual mechanism: D-Ala-D-Ala binding + membrane depolarisation
- 4–8× lower MICs than vancomycin against susceptible S. aureus
- Activity preserved against most VISA, hVISA
- Inactive against VRSA, VanA enterococci
Telavancin — the boxed warnings
Warning
- Nephrotoxicity — higher than vancomycin, particularly in patients with baseline CrCl <50 mL/min
- Fetal harm — animal teratogenicity; pregnancy test required before initiation in women of childbearing potential
- QTc prolongation — avoid in long-QT syndrome, uncompensated CHF, severe LVH, or concomitant QT-prolonging drugs
Plus: coagulation assay interference — PT, aPTT, INR, ACT spuriously prolonged. Draw before next dose for accurate result.
Telavancin clinical evidence
- ABSSSI (ATLAS 1 and 2): non-inferior to vancomycin; cure 88.3% vs 87.1%, and 90.6% vs 86.4% in MRSA subgroup
- HAP/VAP (ATTAIN 1 and 2): non-inferior to vancomycin overall; higher mortality in the subgroup with CrCl <50 mL/min
- Approved indications (US): cSSSI, HAP/VAP caused by S. aureus when alternatives are inappropriate
Dalbavancin
Dalbavancin — defining feature is half-life
- Parent: A40926 (teicoplanin-like glycopeptide), modified with lipophilic side chain
- t½ ~346 hours (~14 days); ~33% of drug still in plasma at 14 days
- Binds D-Ala-D-Ala with enhanced dimerisation
- Activity: MRSA, MSSA, CoNS, streptococci, vancomycin-susceptible enterococci
- Activity reduced against VISA; inactive against VRSA, VanA enterococci
Dalbavancin — clinical trial backbone
- DISCOVER 1 and 2 (Boucher 2014): two-dose regimen (1000 mg + 500 mg/wk) non-inferior to vancomycin → linezolid for ABSSSI
- DUR001-303 (Dunne 2016): single-dose 1500 mg non-inferior to two-dose regimen
- Rappo 2018: randomized comparator-controlled trial for adult osteomyelitis — high cure rates with two-dose dalbavancin
- DOTS (Turner 2025): RCT, dalbavancin (days 1 + 8) vs standard IV therapy for completion treatment in complicated S. aureus bacteraemia after blood-culture clearance — not superior but noninferior; comparable safety
- Vertebral osteomyelitis (open-label cohort): efficacious; growing real-world experience
DOTS — Pharmacokinetic data
Population PK model (n = 97, 640 samples): 3-compartment, zero-order input, first-order elimination
| Parameter | Estimate | 95% CI | IIV (CV%) |
|---|---|---|---|
| CL | 0.066 L/h | 0.062–0.069 | 22.6% |
| V1 (central) | 5.67 L | 5.37–5.99 | 19.7% |
- Protein binding >99% in 92.3% of paired samples — substantially higher than previously estimated (~93%)
- Unbound concentrations linked to total via power function: CU(t) = A × CT(t)K
DOTS PK — covariate effects on disposition
| Covariate | Parameter affected | Exponent | 95% CI |
|---|---|---|---|
| Creatinine clearance | CL ↑ | 0.21 | 0.16–0.30 |
| Body weight | V1 ↑ | 0.57 | 0.37–0.86 |
| Body weight | V2 ↑ | 0.82 | 0.37–1.46 |
| Body weight | V3 ↑ | 0.56 | 0.30–0.82 |
| Albumin | V2 ↓ | −0.81 | −1.79 to −0.32 |
| Albumin | fu scaling ↓ | −0.78 | −0.98 to −0.54 |
| Age | V3 ↑ | 0.63 | 0.44–0.83 |
All covariates entered as power functions on the respective parameter.
DOTS PK — exposure–response: day 22 concentration
- Among 93 evaluable patients, 72 (77.4%) achieved clinical success at day 70
- Total day 22 concentration >32 µg/mL identified as optimal cut point:
| n | Clinical success | ||
|---|---|---|---|
| C22 >32 µg/mL | 30 | 29 (96.7%) | |
| C22 ≤32 µg/mL | 63 | 43 (68.3%) | |
| Adjusted difference | 25.3 pp | 95% CI 3.5–47.0 |
- No increase in serious adverse events in the higher-exposure group (26.7% vs 42.9%; difference −16.2 pp, 95% CI −36.2 to 3.8)
- Effect consistent across subgroups: MRSA/MSSA, bacteraemia duration, deep-seated infection
DOTS PK — unbound exposure and late complications
- 73% of unbound samples below quantification by day 42; 98% by day 70
- All infectious complications occurred after day 40 — temporally coinciding with declining unbound exposure
- Unbound exposure–response associations were attenuated compared with total concentrations
- Narrow dynamic range of unbound concentrations (protein binding >99%)
- Many later samples near the lower limit of quantification (0.05 µg/mL)
Clinical implication: total day 22 concentration is a more practical and stable surrogate for sustained systemic exposure in this population
DOTS PK — implications for TDM and dosing
- Most patients receiving two 1500 mg doses do not achieve day 22 concentrations >32 µg/mL
- Mean day 22 concentration: 29.0 µg/mL; only 32.3% were above the threshold
- Patients below the threshold still had success rates numerically comparable to standard IV therapy
- However: exploratory data suggest some patients may benefit from a third dose between days 22–40
- Guided by low day 22 concentration (TDM approach)
- Or applied empirically in patients at risk for lower exposure (high weight, high CrCl, low albumin)
Important
The 32 µg/mL threshold requires external validation before clinical application. These findings are hypothesis-generating.
Dalbavancin in people who inject drugs (PWID)
- Increasingly used for S. aureus bacteraemia and right-sided endocarditis in PWID
- Single 1500 mg dose covers ~2 weeks of therapy without IV access
- Observational cohorts: outcomes comparable to standard IV therapy in selected patients
- Caveats: requires careful selection (source controlled, no metastatic complications)
- DOTS (Turner 2025) included right-sided native valve endocarditis; showed noninferiority to standard IV therapy — first RCT data in this population
- Dedicated left-sided or prosthetic valve endocarditis RCT data remain absent; further trials needed
Dalbavancin — practical use
- ABSSSI: 1500 mg IV × 1 OR 1000 mg + 500 mg one week later
- Osteomyelitis (off-label): 1500 mg + 1500 mg one week later
- Bacteraemia / endocarditis (off-label): variable regimens, often paired with initial vancomycin/daptomycin then dalbavancin for continuation
- Pediatric ABSSSI: <6 y 22.5 mg/kg; 6–<18 y 18 mg/kg (max 1500 mg)
- 30-minute infusion; 500 mg vials in 5% dextrose, 1–5 mg/mL
- No renal or hepatic adjustment (modest renal clearance reduction in severe impairment but no formal adjustment recommended)
- AEs: nausea, headache, diarrhoea, mild ALT elevation; well tolerated
Oritavancin
Oritavancin — the triple-mechanism agent
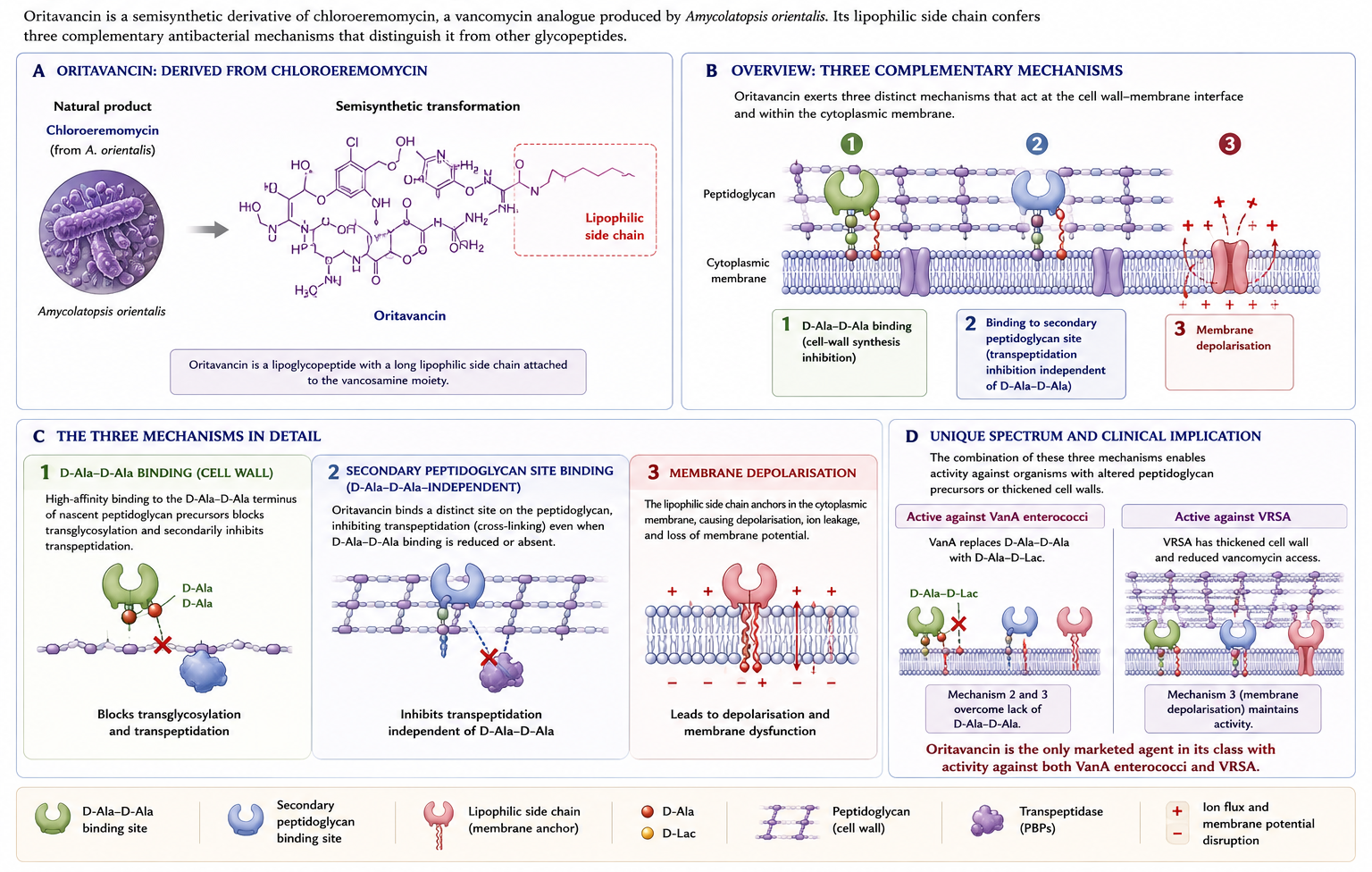
Oritavancin clinical evidence
- SOLO I and SOLO II (Corey 2014, 2015): single 1200 mg dose non-inferior to twice-daily vancomycin × 7–10 days for ABSSSI
- Approved indication: ABSSSI caused by susceptible gram-positive organisms
- Off-label uses (open-label cohorts):
- Acute osteomyelitis (Van Hise 2020 — two-year multicentre cohort, good outcomes with weekly or biweekly oritavancin)
- Prosthetic joint infection
- Bacteraemia, including VRE bacteraemia
- Two formulations: Orbactiv/Tenkasi (3 h infusion) and Kimyrsa (1 h infusion)
Oritavancin — the coagulation problem
Warning
aPTT artifactual prolongation for up to 5 days after a single dose.
Consequences:
- IV unfractionated heparin is contraindicated for 5 days (cannot reliably monitor with aPTT)
- For warfarin within 24 h, use chromogenic assay (not aPTT-based)
- PT/INR also affected up to 12 h
Oritavancin in prosthetic joint infection
- Open-label cohorts: single- or multiple-dose oritavancin for PJI when surgical control achieved
- Particularly attractive for staphylococcal and enterococcal PJI requiring prolonged therapy
- One protocol: 1200 mg IV → 1200 mg in 1 week → maintenance every 4 weeks for chronic suppression
- Evidence base: case series and small open-label cohorts; no RCT yet
- Antimicrobial stewardship implication: requires explicit protocol and follow-up
Oritavancin — other cautions
- CYP450 interactions: weak inhibitor (CYP2C9, CYP2C19), weak inducer (CYP3A4, CYP2D6) — monitor narrow-therapeutic-index substrates
- No dose adjustment for renal or hepatic impairment (mild-to-moderate)
- Adverse events: headache, nausea, vomiting, diarrhoea, mild ALT elevation, infusion reactions (flushing, pruritus)
Stewardship and practical decision-making
When to use lipoglycopeptides
Strong rationale:
- ABSSSI requiring inpatient gram-positive cover but suitable for early discharge / ED treatment
- Patients with poor adherence to oral step-down or unable to take oral
- Difficult IV access where prolonged IV not feasible
- VRE bacteraemia / VanA enterococcal infection — oritavancin specifically
- Outpatient continuation of osteomyelitis or endocarditis therapy (off-label)
Weaker rationale (think twice):
- Routine ABSSSI in patients who can take oral cephalexin/clindamycin/doxycycline
- Hospital-acquired infections where source control isn’t established
- Patients with concurrent need for IV unfractionated heparin (avoid oritavancin)
Pharmacoeconomics — when does cost make sense?
- Acquisition cost: dalbavancin €1500–2500 per 1500 mg dose; oritavancin €2500–3500 per 1200 mg dose (varies by country)
- Per-day hospital ward cost: €500–1500 in most European systems
- Breakeven: ~2–3 hospital days avoided per single-dose lipoglycopeptide
- Cost-effective when:
- Avoiding admission entirely for ABSSSI
- Discharging early from bacteraemia
- Replacing prolonged OPAT IV course
- Less cost-effective when displacing inexpensive oral options
Resistance and surveillance concerns
- Long tissue persistence of dalbavancin and oritavancin → prolonged sub-MIC exposure in vivo
- Theoretical concern for selection of resistance, particularly enterococci
- To date, no large-scale resistance emergence documented in surveillance (SENTRY, ATLAS)
- Vigilance warranted as use expands; reporting of unusual MIC patterns essential
Decision framework — empirical gram-positive cover
| Scenario | First-line | Lipoglycopeptide role |
|---|---|---|
| ABSSSI, inpatient, oral step-down possible | Vancomycin → oral step-down | Single-dose dalbavancin if ED discharge desired |
| ABSSSI, ED, avoid admission | — | Single-dose dalbavancin or oritavancin |
| MRSA bacteraemia, complicated | Vancomycin (AUC) or daptomycin | Dalbavancin for continuation (off-label) |
| MRSA endocarditis | Vancomycin or daptomycin (+ ceftaroline) | Investigational role |
| HAP/VAP, MRSA | Vancomycin or linezolid | Telavancin only if alternatives unsuitable |
| Diabetic foot osteomyelitis, MRSA | Standard regimen | Dalbavancin two-dose attractive |
| VanA VRE bacteraemia | Linezolid, daptomycin (high-dose), tigecycline | Oritavancin if other options exhausted |
| C. difficile colitis | Oral vancomycin or fidaxomicin | No role |
Cases for discussion
Case 1 — MRSA bacteraemia with rising creatinine
55-year-old man, T2DM, admitted with right-sided infective endocarditis, MRSA bacteraemia. Day 5 of vancomycin (trough 18 mg/L, AUC 580). Creatinine has risen from 0.9 → 1.6 mg/dL. Blood cultures still positive at 96 h.
What do you do?
- Switch to daptomycin 8–10 mg/kg?
- Add ceftaroline?
- Continue vancomycin and accept renal injury?
- Image to look for missed focus?
Case 2 — ABSSSI in IV drug user
32-year-old woman, active opioid injection use, presents with extensive cellulitis of forearm at injection site. Stable, no systemic features. MRSA likely. Refusing admission, no IV access available, unreliable for outpatient appointments.
What’s your antibiotic strategy?
- Standard oral cephalexin → outpatient?
- IV vancomycin via PICC?
- Single-dose dalbavancin 1500 mg in ED?
- Single-dose oritavancin 1200 mg in ED?
Case 3 — VanA VRE bacteraemia
68-year-old, post-cardiac surgery, in ICU on day 21. New fever with positive blood cultures: E. faecium VanA phenotype. Patient has acute kidney injury (CrCl 30 mL/min) and is on dual antiplatelet therapy.
Treatment options?
- Linezolid 600 mg q12h
- Daptomycin 10 mg/kg (renally adjusted)
- Oritavancin single-dose
- Tigecycline
Take-home messages
Five key teaching points
- Vancomycin is still the workhorse — but use AUC-guided dosing (400–600 mg·h/L) for serious MRSA infection. Trough-only is yesterday’s standard.
- Resistance: VanA, VanB define VRE clinical management; hVISA and VISA require an alternative agent; VRSA is rare but real.
- Teicoplanin: always load (10–12 mg/kg q12h × 3–5 doses) — target troughs 15–30 (mild) or 20–40 (severe) mg/L. Lower nephrotoxicity, no US availability.
- Dalbavancin / oritavancin: single- or two-dose regimens with weeks-long half-lives — game-changing for outpatient ABSSSI and growing role in osteomyelitis/endocarditis. Cost matters.
- Oritavancin uniquely covers VRSA and VanA enterococci — but its 5-day aPTT interference contraindicates concurrent IV unfractionated heparin.
Questions to think about
- For your hospital, what is the local prevalence of MRSA, hVISA, VRE phenotypes? How does this change your empirical choices?
- Is your lab equipped to flag MIC creep or to perform PAP-AUC for suspected hVISA?
- Does your antimicrobial stewardship programme have a protocol for single-dose dalbavancin in the ED? What patient-selection criteria would you build in?
- For your next vancomycin patient, will you use trough-based or AUC-based dosing? What tool will you use?
Key references
- Murray BE, Arias CA, Nannini EC. Glycopeptides and lipoglycopeptides. In: Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases, 9th ed., 2025.
- Rybak MJ et al. Therapeutic monitoring of vancomycin for serious MRSA infections: A revised consensus guideline by ASHP/IDSA/PIDS/SIDP. Am J Health-Syst Pharm. 2020.
- Liu C et al. Clinical practice guidelines by IDSA for the treatment of MRSA infections in adults and children. Clin Infect Dis. 2011.
- Kalil AC et al. Management of adults with hospital-acquired and ventilator-associated pneumonia: IDSA/ATS guidelines. Clin Infect Dis. 2016.
- Shariati A et al. Global prevalence of vancomycin-resistant, intermediate, and heterogeneously vancomycin-intermediate S. aureus: systematic review and meta-analysis. Sci Rep. 2020.