Primary targets: Topoisomerases
Quinolones target two essential bacterial enzymes:
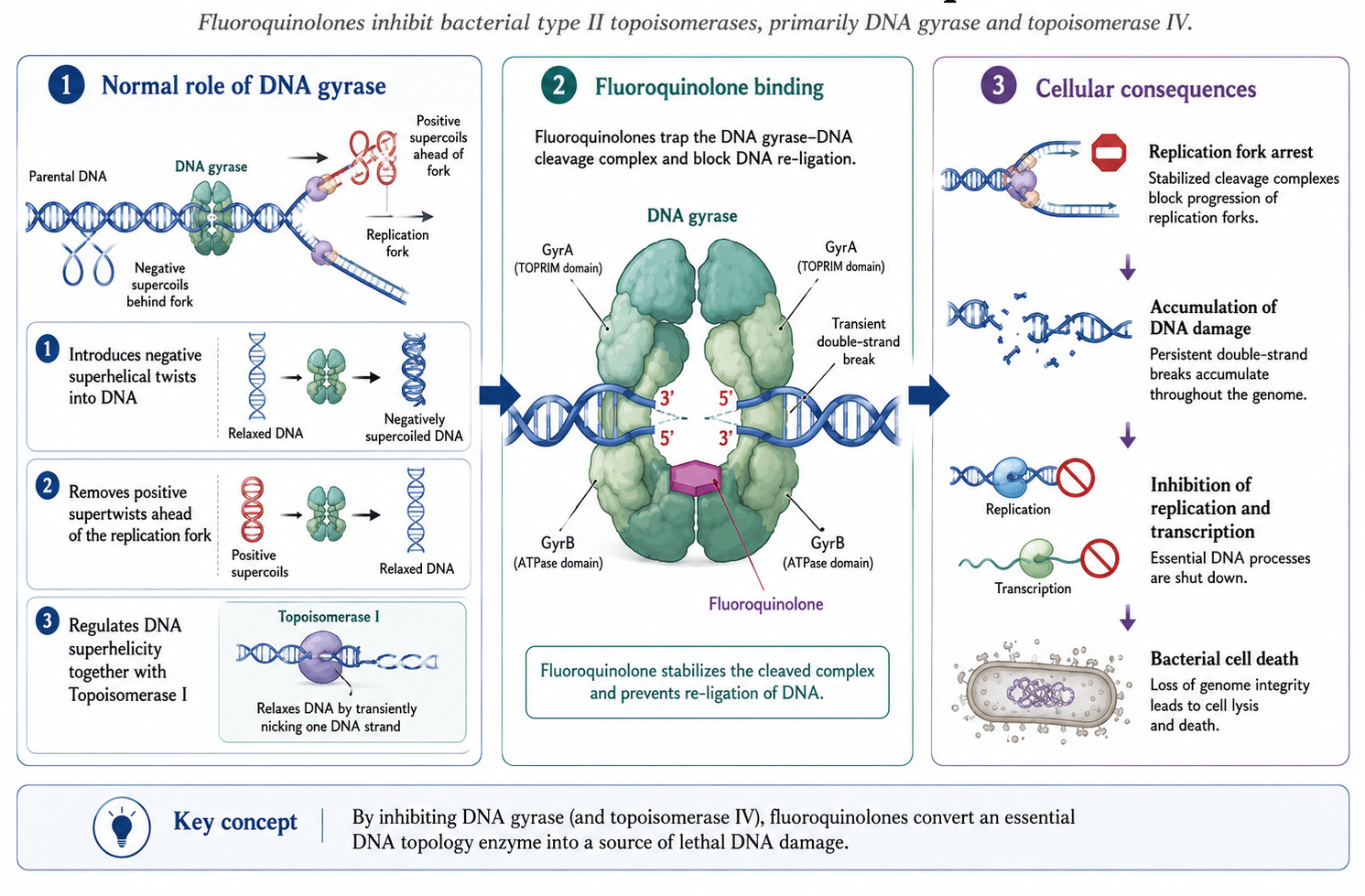
- DNA Gyrase (GyrA, GyrB subunits)
- Topoisomerase IV (ParC, ParE subunits)
- Both are Type II topoisomerases required for DNA replication.
Russell E. Lewis
Associate Professor of Infectious Diseases (MEDS-10/B)

russelledward.lewis@unipd.it
https://github.com/Russlewisbo
Slides and course materials: www.idpadova.com
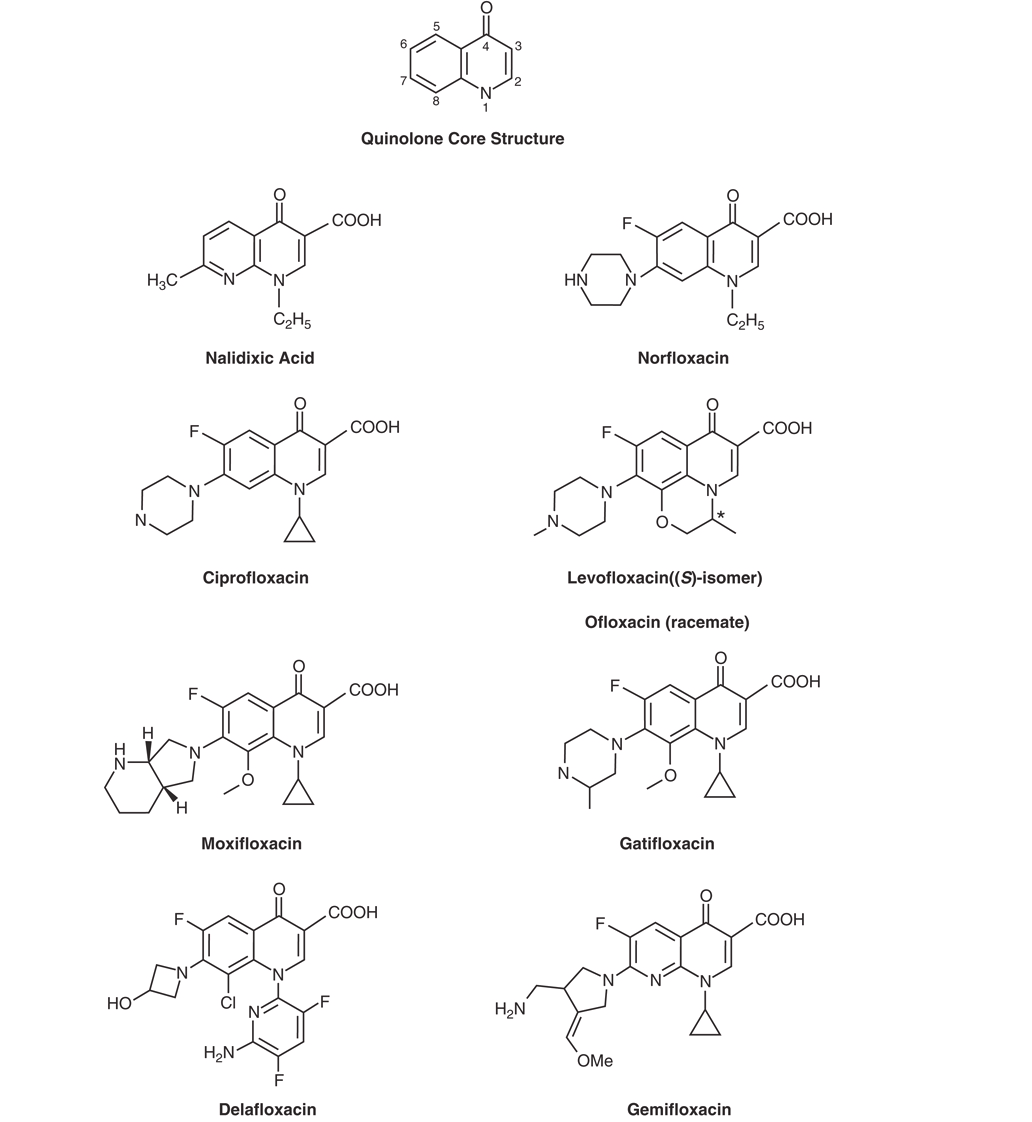
| Generation | Examples | Key Features |
|---|---|---|
| 1st | Nalidixic acid | UTI only; narrow spectrum |
| 2nd | Norfloxacin, Ciprofloxacin | Broader gram-negative; systemic use |
| 3rd | Levofloxacin | Enhanced gram-positive |
| 4th | Moxifloxacin, Gemifloxacin | Enhanced respiratory pathogens |
Older agents:
Newer agents:
Quinolones target two essential bacterial enzymes:
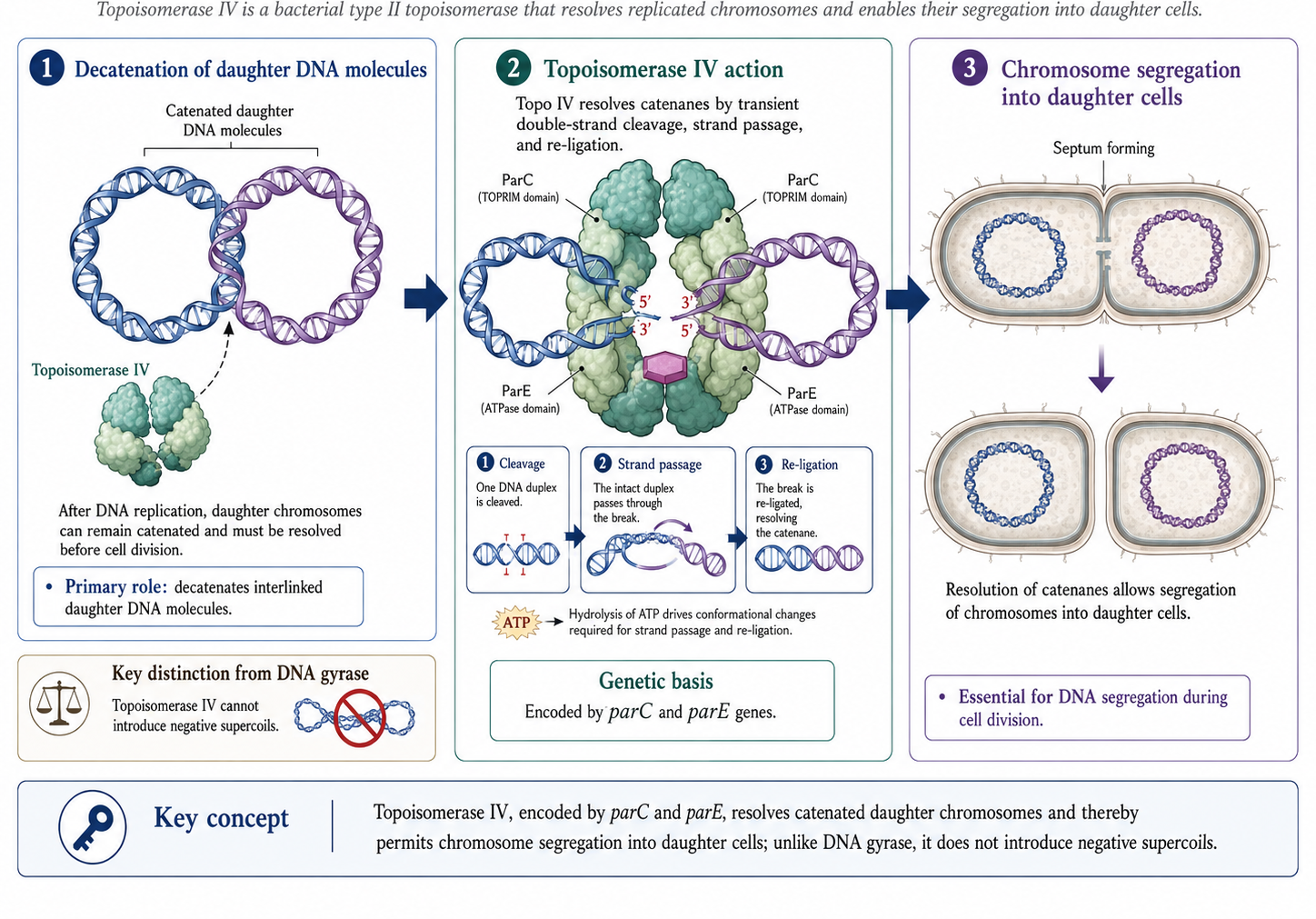
| Organism Type | Primary Target | Secondary Target |
|---|---|---|
| Gram-negative | DNA Gyrase | Topoisomerase IV |
| Gram-positive | Topoisomerase IV | DNA Gyrase |
How quinolones kill bacteria:
Key Point
Post-antibiotic effect: 1-2 hours
Quinolone resistance occurs through:
Quinolone Resistance-Determining Region (QRDR):
First mutation in primary target enzyme
Low-level resistance (8-fold MIC increase)
Second mutation in secondary target
High-level clinical resistance
Warning
Serial passage selects progressively resistant mutants!
| Organism | Pump System | Clinical Significance |
|---|---|---|
| E. coli | AcrAB-TolC | Often combined with gyrA mutations |
| P. aeruginosa | MexAB-OprM | Common in clinical isolates |
| P. aeruginosa | MexCD-OprJ | Selected by fluoroquinolone use |
| K. pneumoniae | OqxAB-TolC | Plasmid-encoded |
S. aureus:
Tip
Moxifloxacin is not affected by NorA overexpression!
Qnr proteins protect topoisomerases from quinolone action:
AAC(6’)-Ib-cr:
Rising Resistance
Best Activity:
Variable Activity:
Ciprofloxacin
Remains the most potent quinolone against gram-negative bacteria, especially P. aeruginosa
| Organism | Cipro | Levo | Moxi | Gemi | Dela |
|---|---|---|---|---|---|
| MSSA | 0.5 | 0.25 | 0.12 | 0.06 | 0.008 |
| MRSA | ≥32 | 16 | 4 | 8 | 0.5 |
| S. pneumoniae | 2 | 1 | 0.25 | 0.06 | 0.015 |
“Respiratory fluoroquinolones” have enhanced activity against:
Agents: levofloxacin, moxifloxacin, gemifloxacin
| Agent | B. fragilis MIC90 |
|---|---|
| Ciprofloxacin | 4-64 |
| Levofloxacin | 2->16 |
| Moxifloxacin | 0.5-8 |
| Delafloxacin | 0.12 |
Note
Most quinolones have poor anaerobic activity; moxifloxacin and delafloxacin are exceptions.
| Agent | M. tuberculosis | M. avium | M. fortuitum |
|---|---|---|---|
| Ciprofloxacin | 1 | 16 | 0.3->4 |
| Levofloxacin | 0.25-1 | 0.5-64 | 0.06-2 |
| Moxifloxacin | 0.125-0.5 | 0.5-16 | 0.06-1 |
CDC Recommendations
| Quinolone | Dose (mg) | Cmax (μg/mL) |
|---|---|---|
| Norfloxacin | 400 PO | 1.5 |
| Ciprofloxacin | 500 PO | 2.4 |
| Ofloxacin | 400 PO | 4.6 |
| Levofloxacin | 500 PO | 5.7 |
| Moxifloxacin | 400 PO | 4.3 |
| Delafloxacin | 450 PO | 7.45 |
| Site | Fold Increase |
|---|---|
| Feces | 100-1000× |
| Macrophages/Neutrophils | 2->100× |
| Bile | 2-20× |
| Lung tissue | 1.6-6× |
| Prostate tissue | 0.9-2.3× |
Warning
CSF penetration is generally LOW without meningeal inflammation
Primarily Renal:
Requires dose adjustment in renal impairment
Primarily Hepatic:
No renal dose adjustment
| Agent | CrCl 10-50 | CrCl <10 |
|---|---|---|
| Norfloxacin | q24h | q24h |
| Ciprofloxacin | q18h | q24h |
| Ofloxacin | q24h | ½ dose q24h |
| Levofloxacin | ½ dose q24h | ½ dose q48h |
| Moxifloxacin | No change | No change |
Critical interaction
Aluminum, magnesium, calcium, iron, and zinc form poorly absorbed chelates with quinolones.
Timing: Take quinolone 2 hours before or 2-6 hours after these agents
Ciprofloxacin inhibits CYP1A2:
| Drug | Effect |
|---|---|
| Theophylline | 30% ↓ clearance; monitor levels |
| Caffeine | ↑ levels |
| Tizanidine | ↑ CNS/hypotensive effects; AVOID |
| Clozapine | ↑ levels; monitor |
Note
Other quinolones have minimal CYP1A2 effects
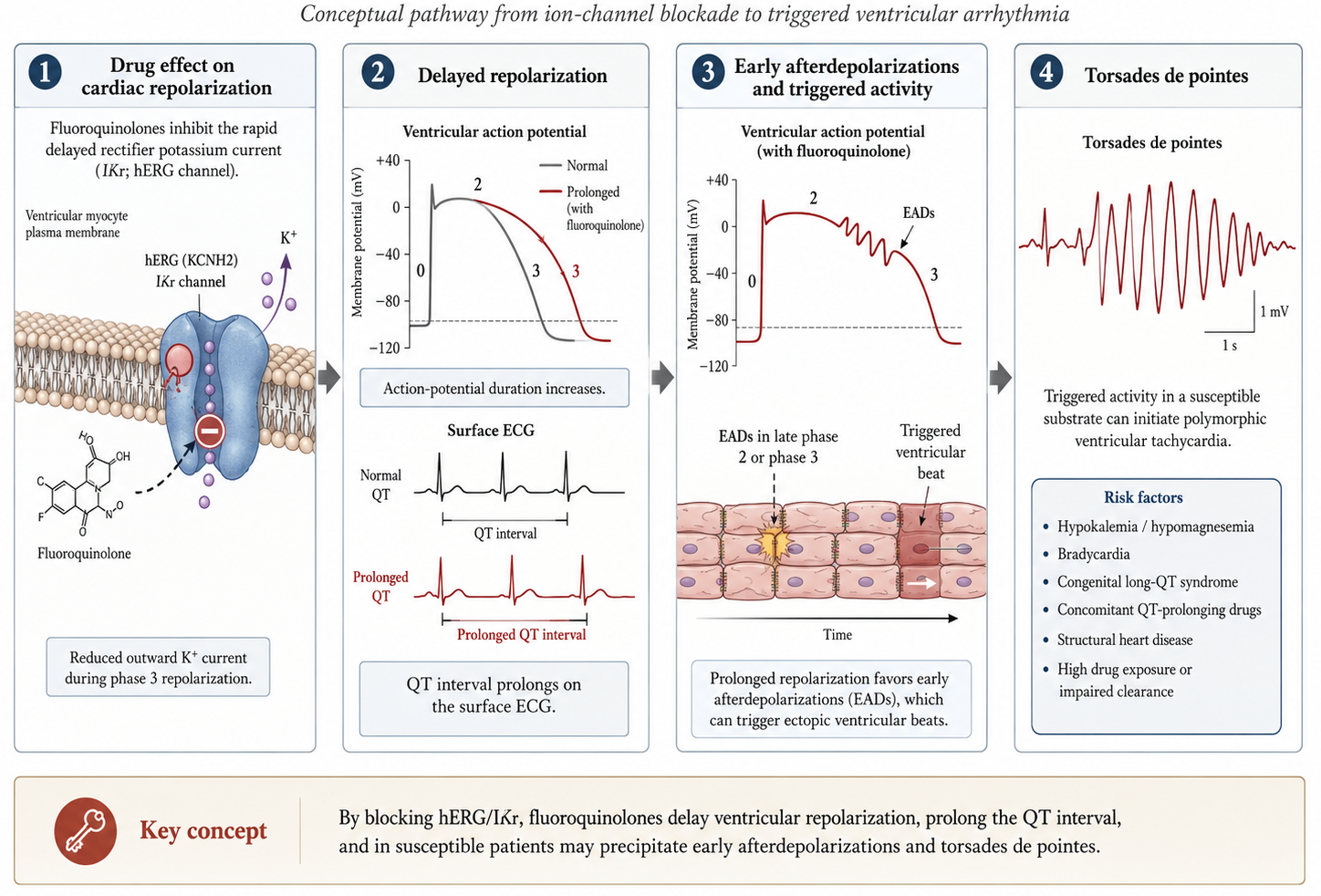
Warning
Avoid combining with other QT-prolonging agents:
Risk: Moxifloxacin > Levofloxacin > Ciprofloxacin
Uncomplicated cystitis (3-day course):
Warning
Reserve for patients with contraindications to first-line agents
First-line for chronic bacterial prostatitis
NO longer recommended for empirical gonorrhea treatment!
| Indication | Agent | Duration |
|---|---|---|
| Shigellosis | Ciprofloxacin | 3 days |
| Traveler’s diarrhea | Ciprofloxacin | 1-3 days |
| Typhoid (susceptible) | Ciprofloxacin | 5-7 days |
| Severe Salmonella | Ciprofloxacin | 7-14 days |
Warning
Watch for resistance in Salmonella from South/Southeast Asia
“Respiratory fluoroquinolones” provide:
IDSA/ATS Guidelines
Consider respiratory fluoroquinolones for CAP in:
Delafloxacin — newest quinolone:
Advantages of quinolones:
Note
Consider combination with rifampin for staphylococcal infections
Tuberculosis:
NTM:
FDA Black Box Warnings
Most common adverse effects (1-5%):
Warning
Associated with C. difficile outbreaks (NAP1/BI/027 strain)
| Effect | Frequency |
|---|---|
| Headache | 1-4% |
| Dizziness | 1-4% |
| Insomnia | 1-2% |
| Restlessness | 1-2% |
| Seizures | Rare |
Risk factors: High dose, renal impairment, concurrent NSAIDs
FDA Black Box Warning
Risk factors:
FDA Warning
Symptoms: Pain, burning, tingling, numbness, weakness
Relative risk by agent:
Warning
Avoid in: Long QT syndrome, uncorrected hypokalemia, concurrent QT-prolonging drugs
Both hypo- and hyperglycemia reported:
Warning
Monitor glucose in diabetic patients
Pediatrics:
Pregnancy:
Myasthenia Gravis:
| Interaction | Management |
|---|---|
| Cation-containing products | Separate by 2+ hours |
| Tizanidine | Avoid with ciprofloxacin |
| Theophylline | Monitor levels with ciprofloxacin |
| QT-prolonging drugs | Avoid; use ciprofloxacin if necessary |
| Warfarin | Monitor INR |
| Clinical Scenario | Preferred Agent(s) |
|---|---|
| Pseudomonas infection | Ciprofloxacin, Levofloxacin |
| CAP/Respiratory | Levofloxacin, Moxifloxacin |
| SSTI (including MRSA) | Delafloxacin |
| UTI/Prostatitis | Ciprofloxacin, Levofloxacin |
| Renal impairment | Moxifloxacin |
| Cardiac risk | Ciprofloxacin |
| Anaerobic coverage needed | Moxifloxacin |
| Organism | Cipro | Levo | Moxi |
|---|---|---|---|
| E. coli | 0.25 | 0.5 | 0.25 |
| K. pneumoniae | 0.5 | 0.5 | 1 |
| P. aeruginosa | 0.25-2 | 0.5-2 | 4-8 |
| H. influenzae | ≤0.03 | 0.03 | 0.03 |
| M. catarrhalis | ≤0.015 | ≤0.03 | ≤0.015 |
| Organism | Cipro | Levo | Moxi |
|---|---|---|---|
| Legionella spp. | 0.016-0.06 | 0.016-0.03 | 0.06 |
| M. pneumoniae | 0.5-4 | 0.5-2.5 | 0.12-0.3 |
| C. pneumoniae | 2 | 0.5-1 | 0.06-1 |
| C. trachomatis | 0.5-2 | 0.25-0.5 | 0.06 |
| Agent | Standard Dose | Renal Adjustment |
|---|---|---|
| Ciprofloxacin | 500 mg PO q12h | ↓ if CrCl <30 |
| Ciprofloxacin | 400 mg IV q12h | ↓ if CrCl <30 |
| Levofloxacin | 750 mg PO/IV daily | ↓ if CrCl <50 |
| Moxifloxacin | 400 mg PO/IV daily | None needed |
| Delafloxacin | 450 mg PO q12h | ↓ if CrCl <30 |