Febrile Neutropenia
Associate Professor of Infectious Diseases
Department of Molecular Medicine
University of Padua
 |
 |
russelledward.lewis@unipd.it
https://github.com/Russlewisbo
Slides and course materials: www.padovaid.com
Normal hematopoiesis
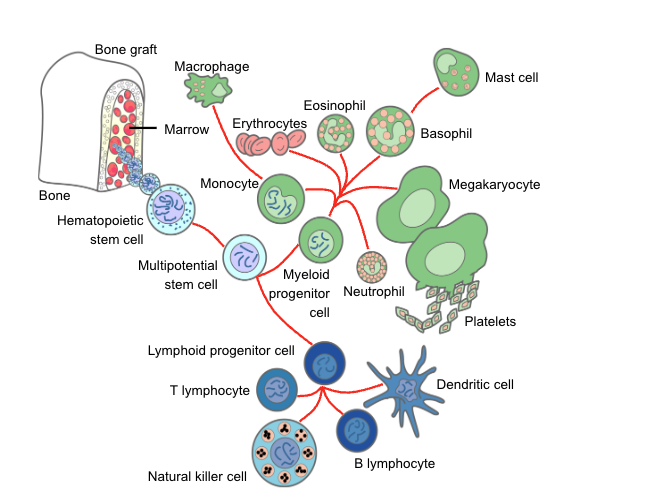
Myeloid lineage (neutrophils / platelets)
- Homogeneous, terminally differentiated effector cells
- Short-lived, post-mitotic
- Continuous high-throughput production
- Rapid quantitative recovery after chemotherapy
(≈2–3 weeks)
Lymphoid lineage (T, B, NK cells)
- Highly heterogeneous populations
- Mix of short-lived effector cells and long-lived memory cells
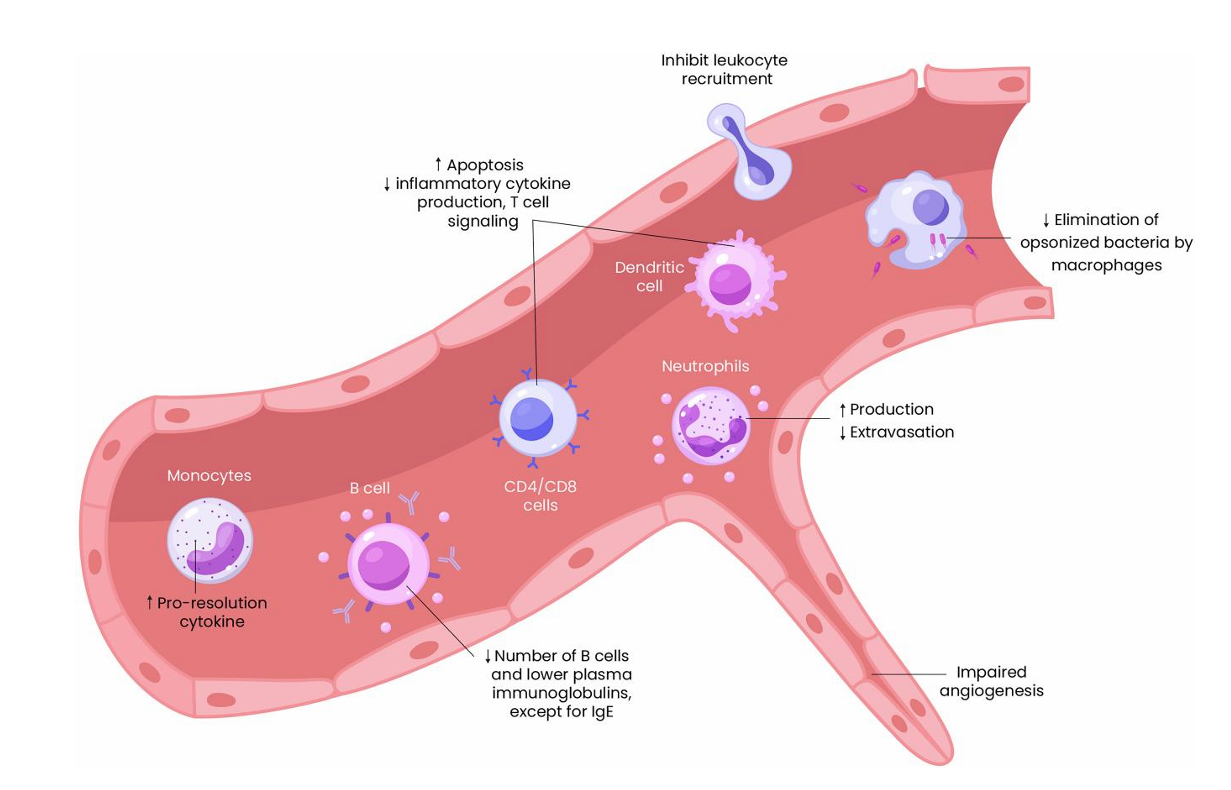
Corticosteroids
Paradoxical effects:
- ↑ Granulocytopoiesis (apparent benefit)
- ↓ Accumulation at infection site
- ↓ Adherent capacity
- ↓ Chemotaxis
- ↓ Phagocytosis
- ↓ Intracellular killing
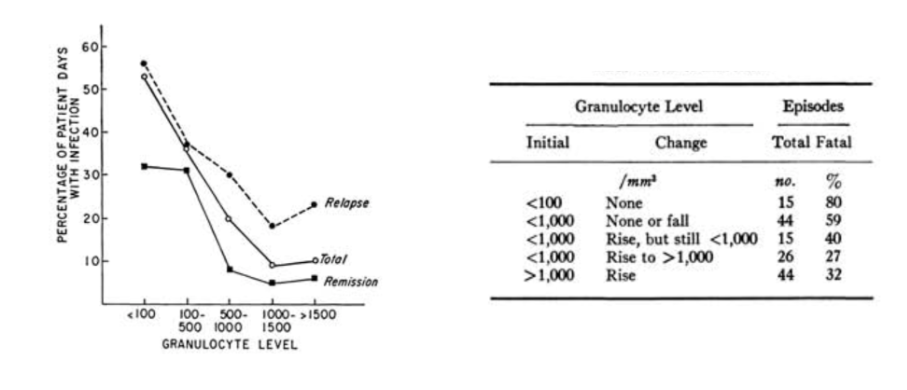
Quantitative relationship of neutropenia
with infection risk
The integument
Skin:
- Chemotherapy → hair loss, dryness
- Catheters → direct microbial access
- Broken skin → S. aureus, gram-negatives
Oropharynx:
- Xerostomia + antibiotics → thrush, bacterial overgrowth
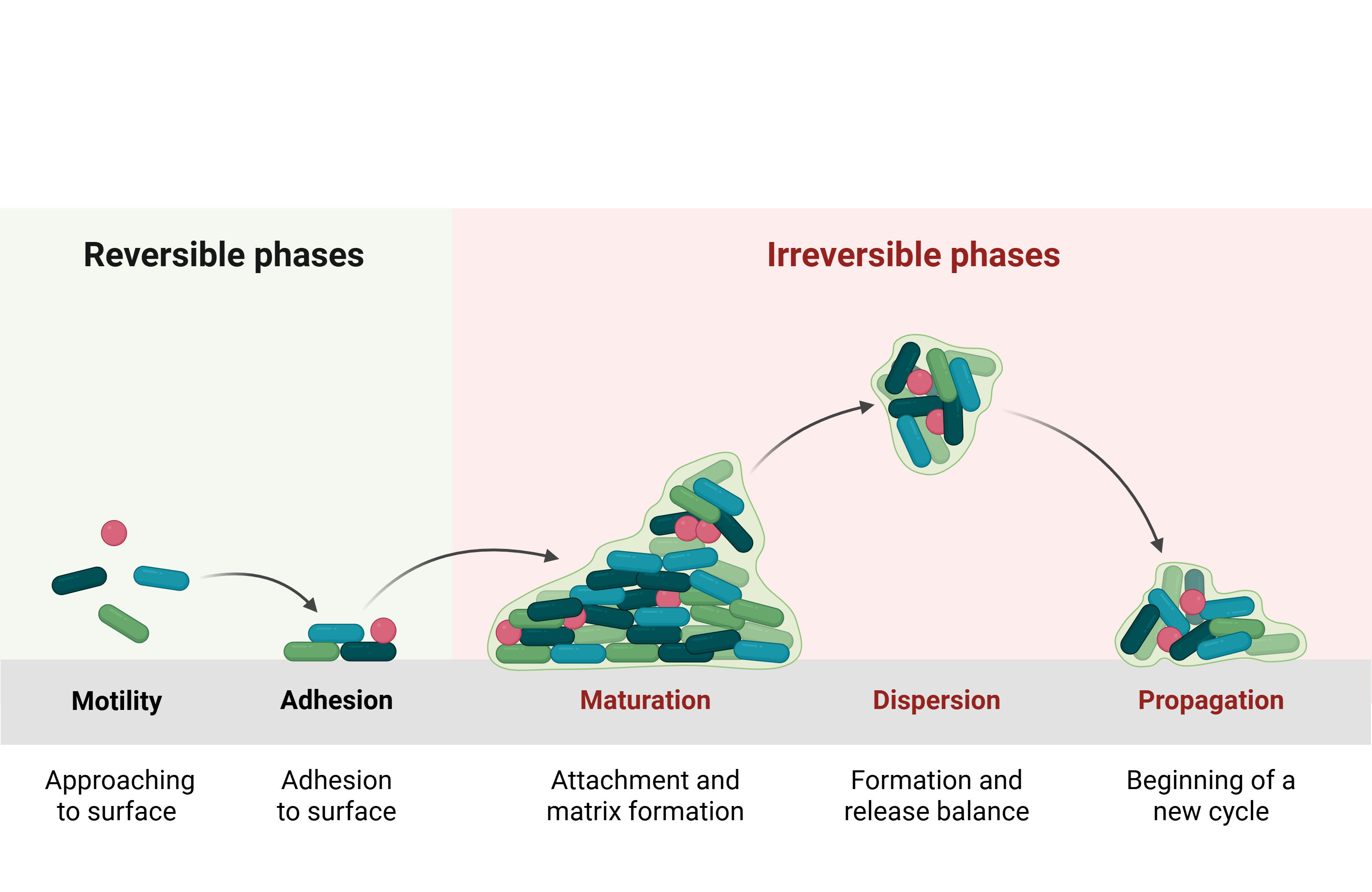
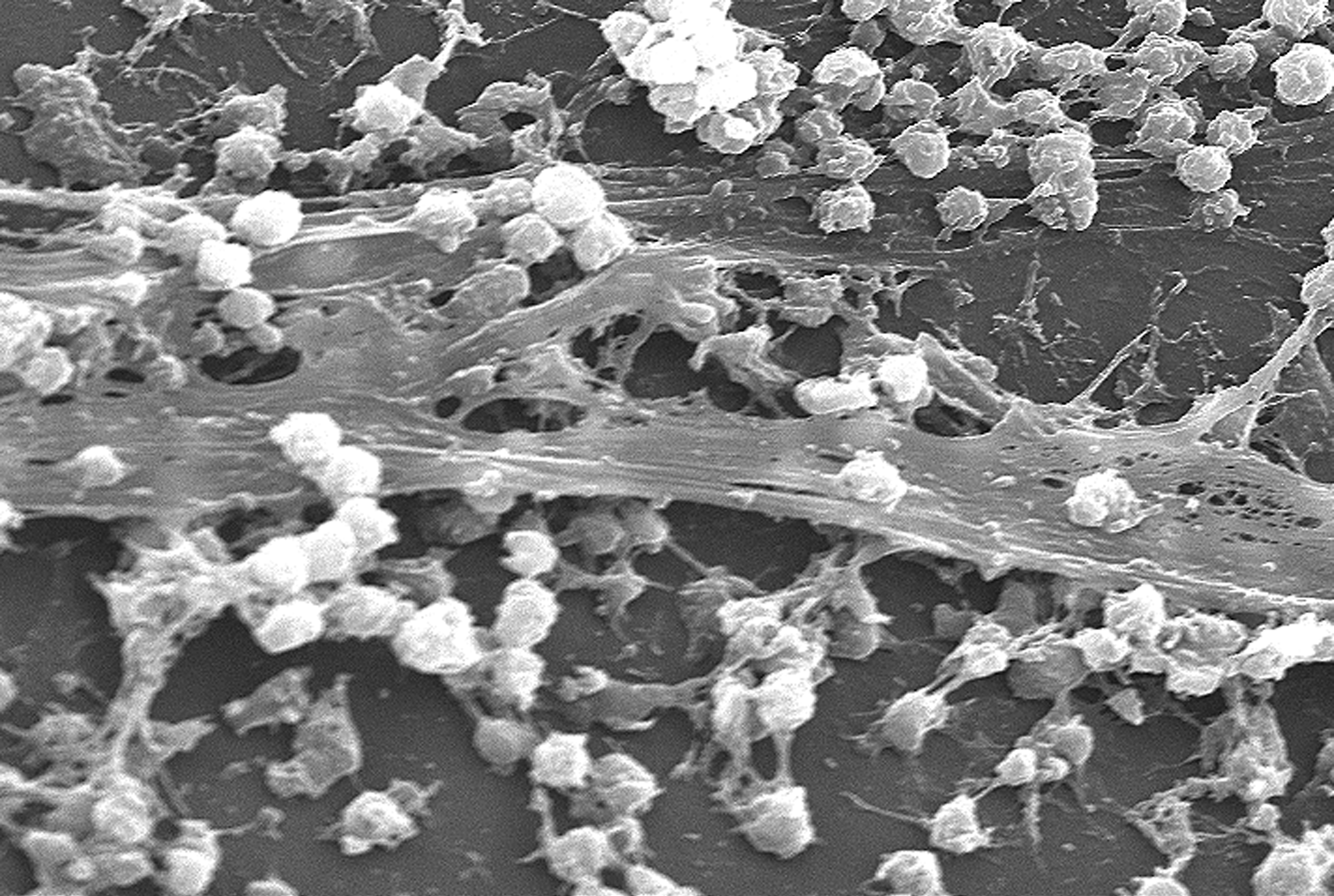
Chemotherapy-associated dysbiosis
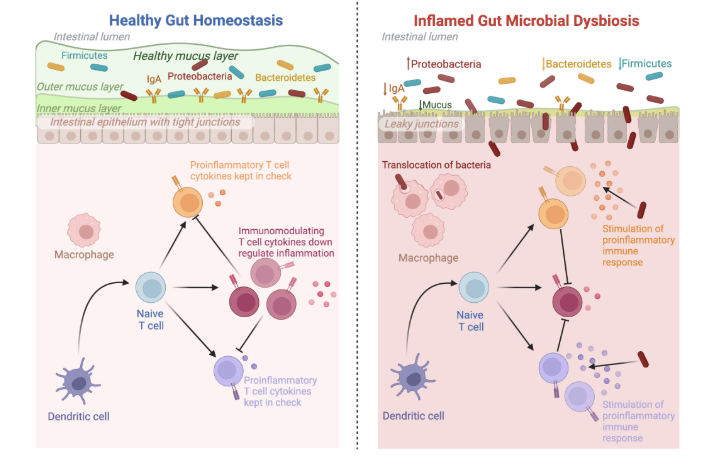
Model of mucosal barrier injury
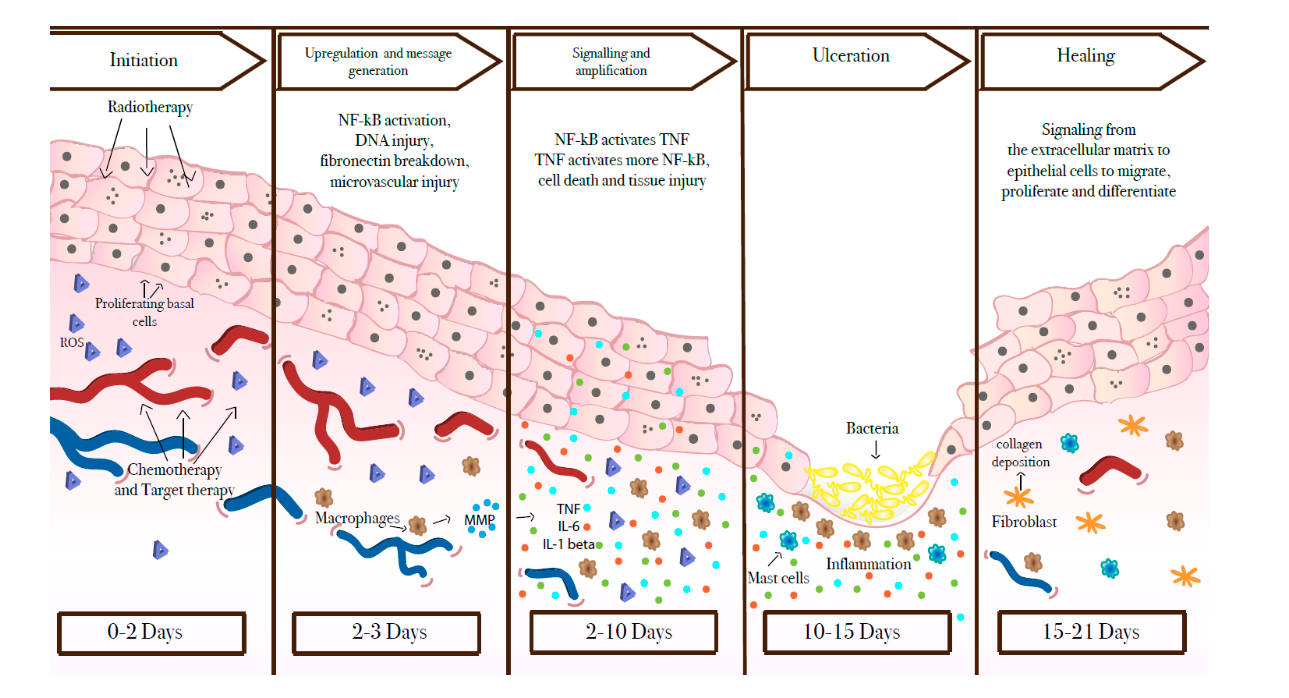
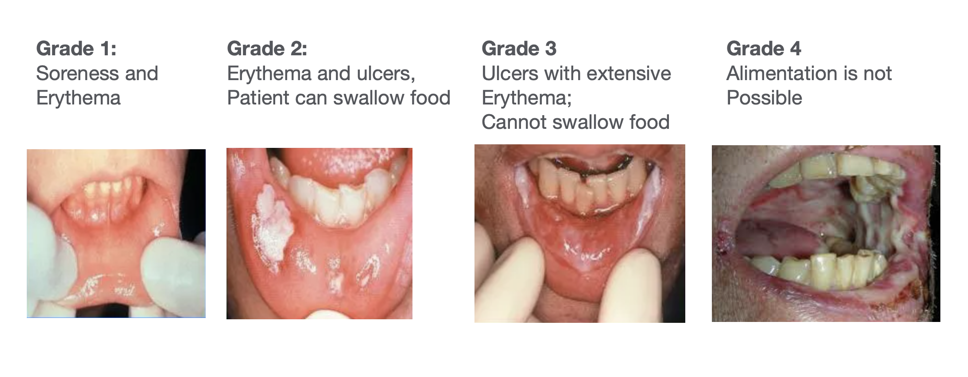
Mucositis
Which pathogens translocate?
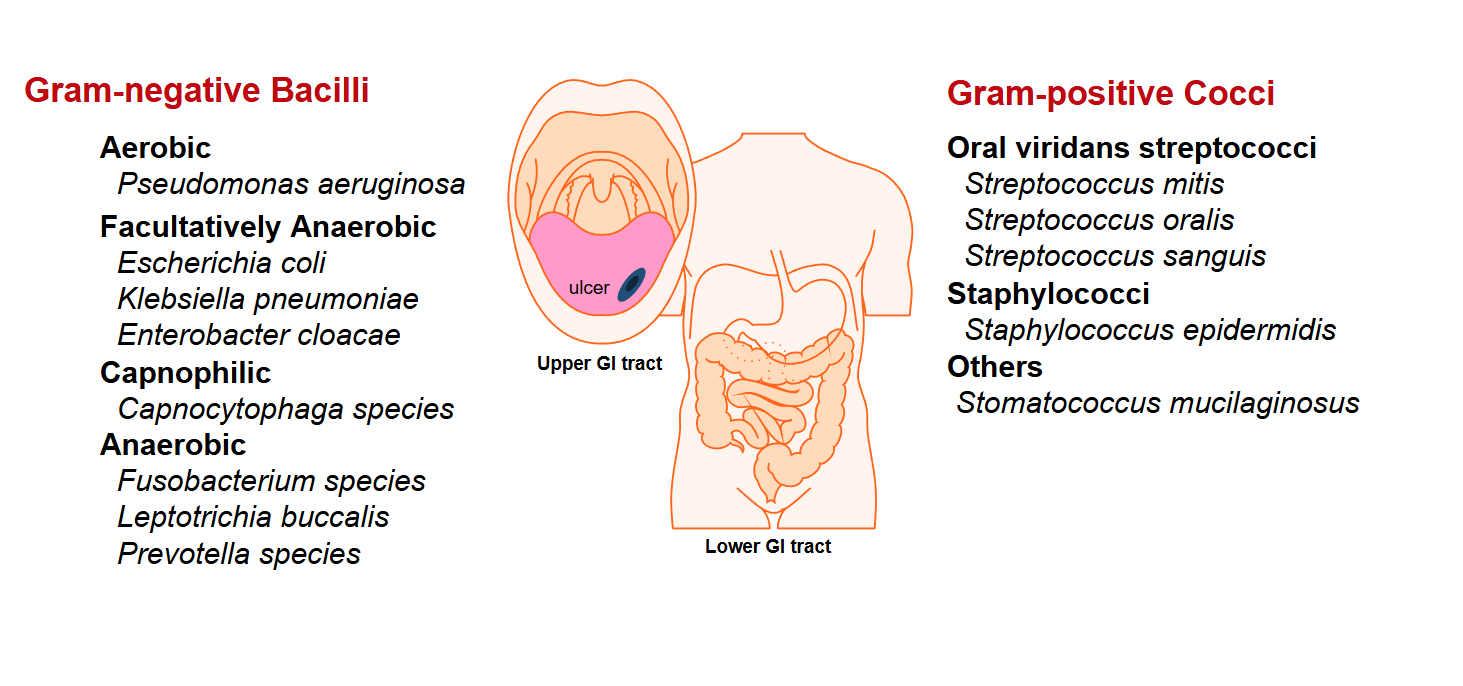
Most common bacterial pathogens
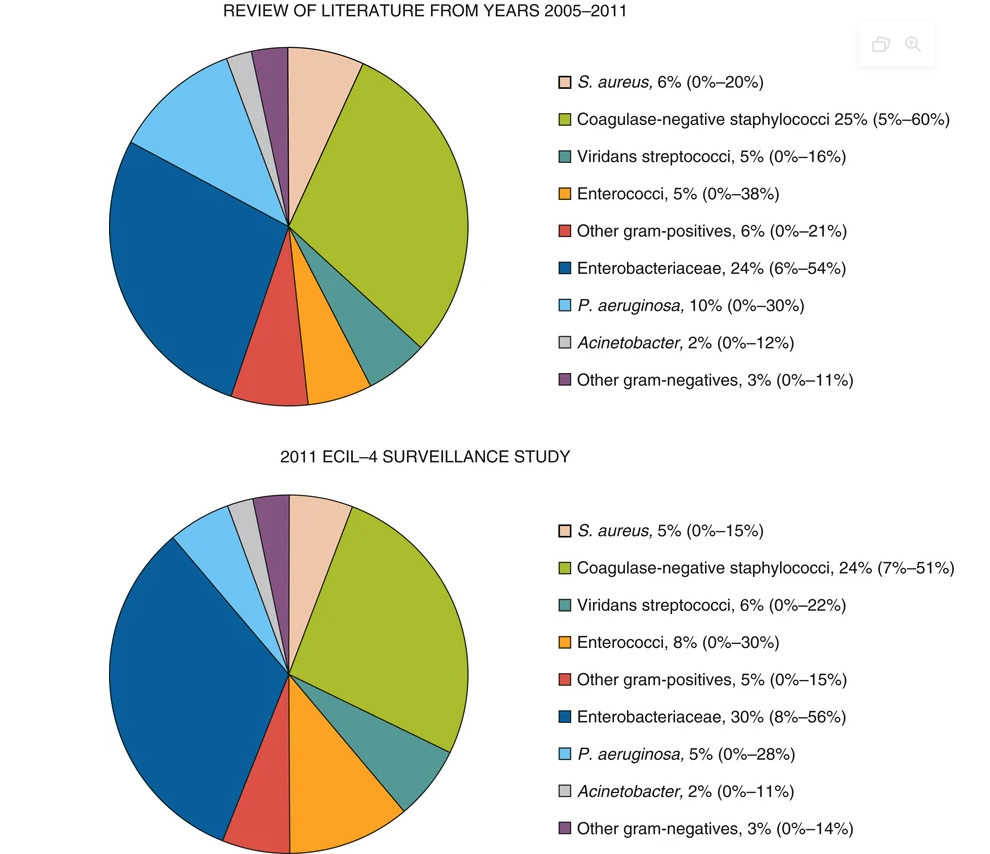
- Infectious source documented in only 20-30% of episodes
- Bacteremia documented in 10-25% of patients with fever
- Aerobic Gram-positive and Gram-negative
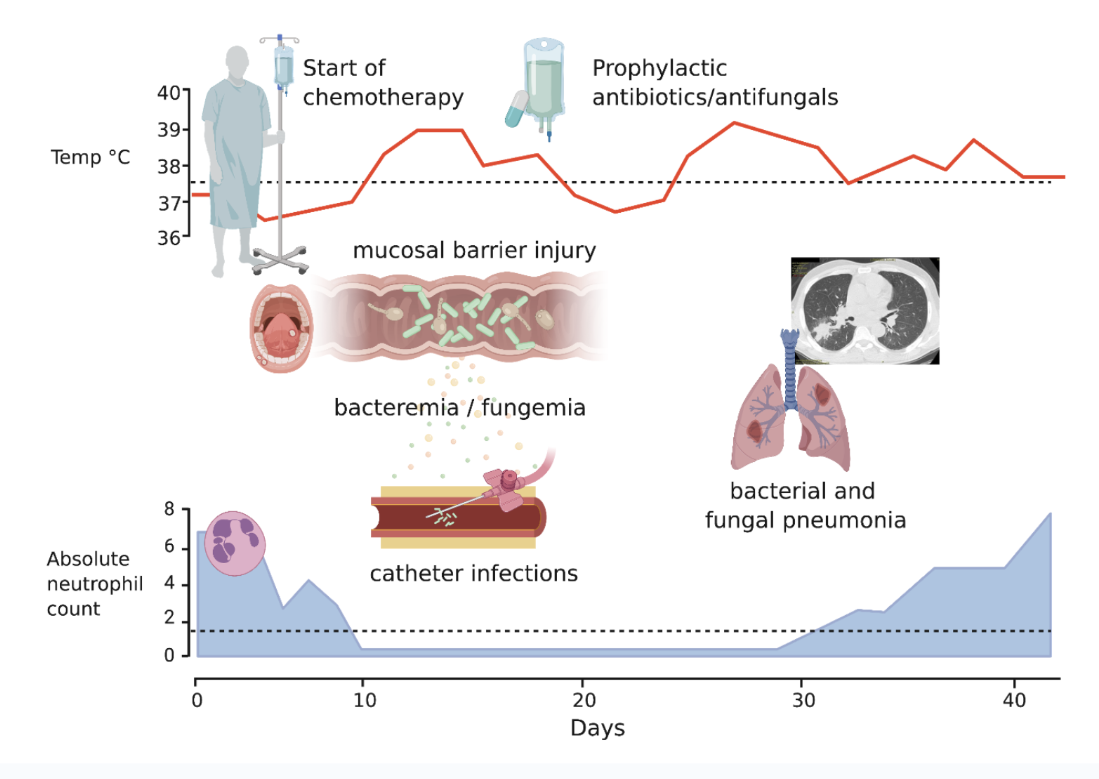
Sequence of infection
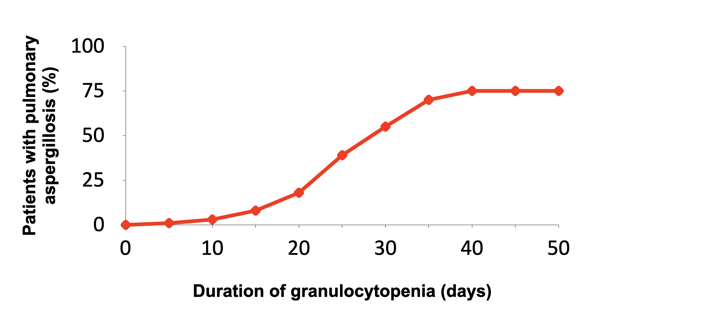
Invasive pulmonary aspergillosis risk vs. neutropenia
CVC-related infection rates
| Catheter Type | Per 100 devices | Per 1000 catheter-days | |
|---|---|---|---|
| Hickman/Broviac |  |
22.5 | 1.6 |
| Port-a-cath |  |
3.5-4 | 0.1 |
| PICC |  |
3.1 | 1.1 |
Impaired cell-mediated immunity increases the spectrum of possible pathogens
 :
:
Granulocyte-colony stimulating factor (G-CSF)
Primary prophylaxis:
- When febrile neutropenia risk >20%
- Based on age, comorbidities, regimen
Secondary prophylaxis:
- After prior neutropenic complication
- When dose reduction would compromise outcomes
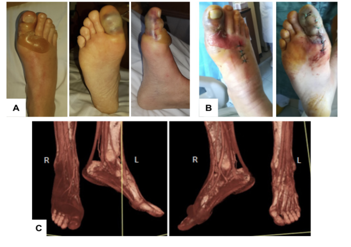
Mucormycosis

Central venous catheter (CVC) infections
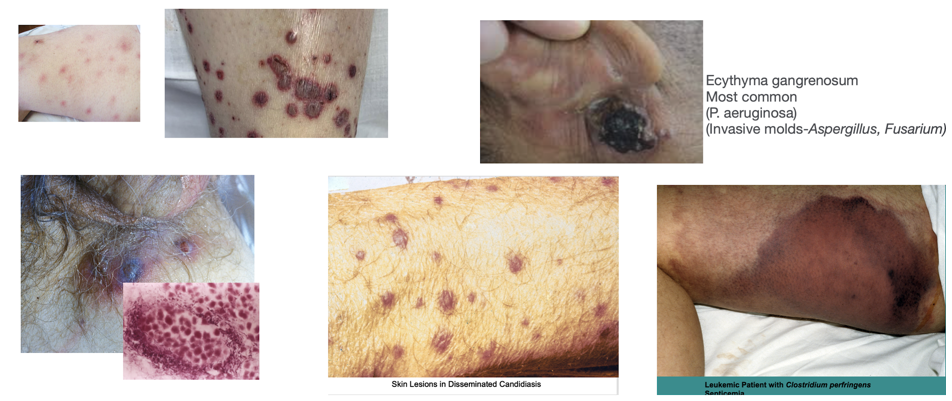
Skin lesions
Oral- Upper GI infection
Candida- Thrush, esophagitis (odynophagia, retrosternal pain)
Vesicular lesions- painful grouped lesions→ulceration

Disseminated HSV- widespread vesicular rash , hepatitis (↑ AST/ALT, sometimes severe), pneumonitis
Pneumonia
up to 60% of patients may have findings of pneumonia on CT
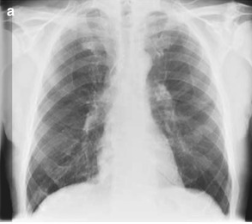
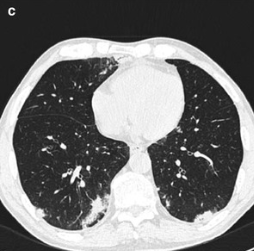
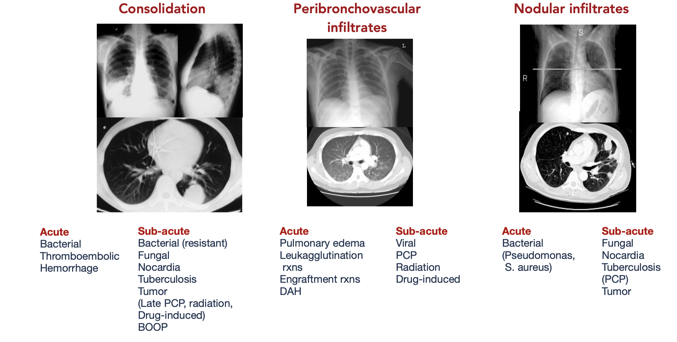
Common CT findings
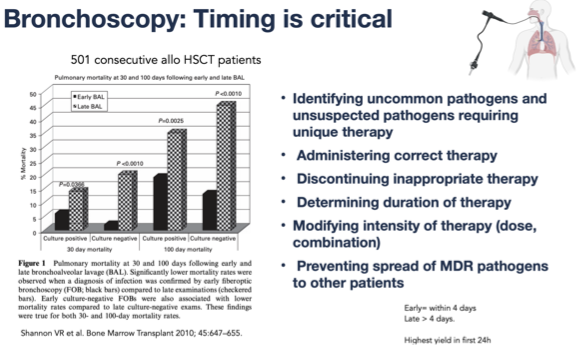
Bronchoscopy
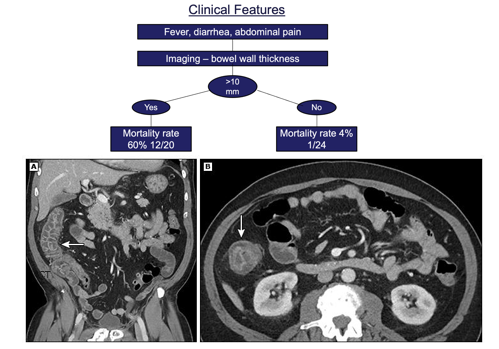
Neutropenic Enterocolitis (Typhlitis)