Febrile Neutropenia
Associate Professor of Infectious Diseases
Department of Molecular Medicine, University of Padua

https://github.com/Russlewisbo
Slides and course materials: www.padovaid.com
Background video: Neutrophil chasing S. aureus.
Taken by Dr. David Rogers, University of Vanderbuilt
Normal hematopoiesis
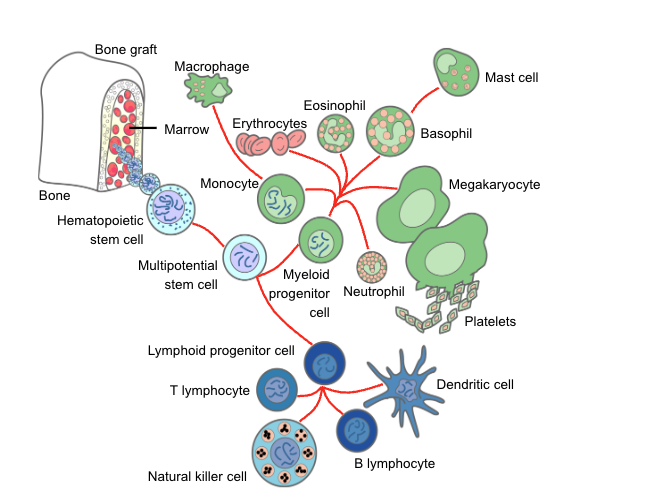
Myeloid lineage (neutrophils / platelets)
- Homogeneous, terminally differentiated effector cells
- Short-lived, post-mitotic
- Continuous high-throughput production
- Rapid quantitative recovery after chemotherapy (≈2–3 weeks)
Lymphoid lineage (T, B, NK cells)
- Highly heterogeneous populations
- Mix of short-lived effector cells and long-lived memory cells
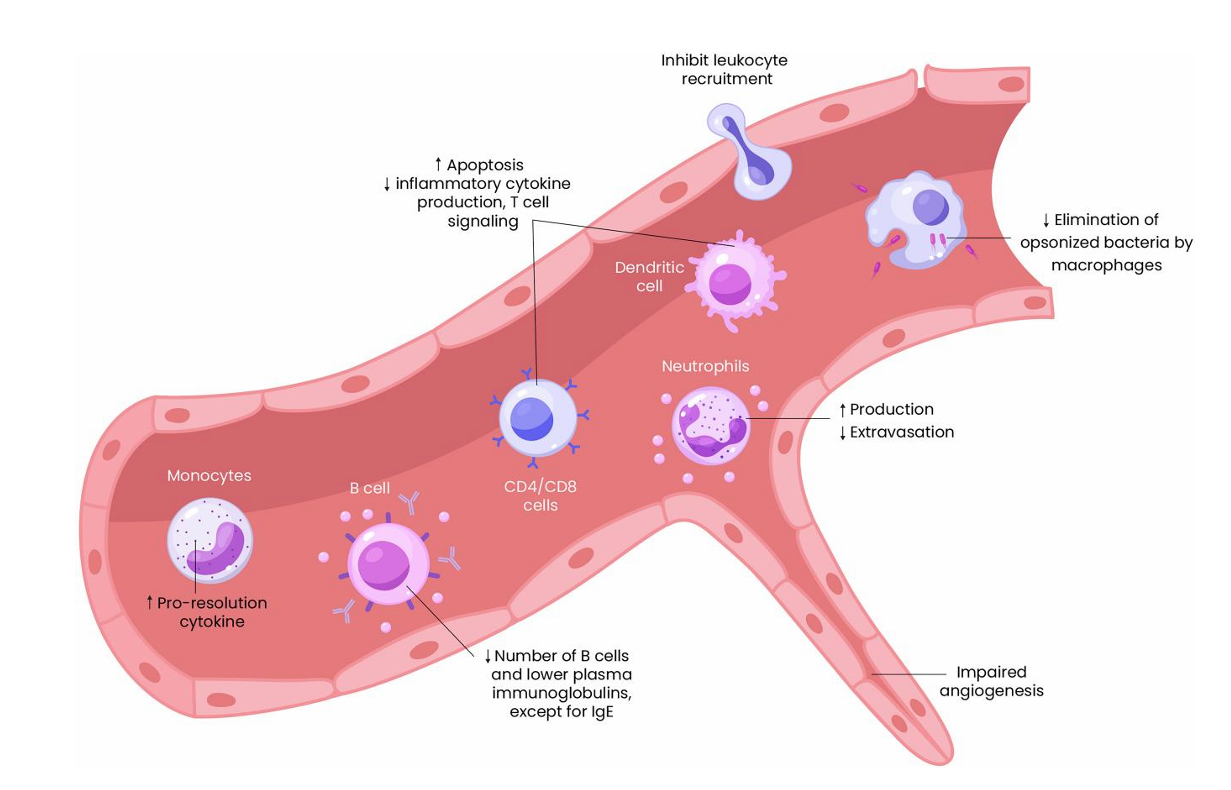
Corticosteroids
Paradoxical effects:
- ↑ Granulocytopoiesis (apparent benefit)
- ↓ Accumulation at infection site
- ↓ Adherent capacity
- ↓ Chemotaxis
- ↓ Phagocytosis
- ↓ Intracellular killing
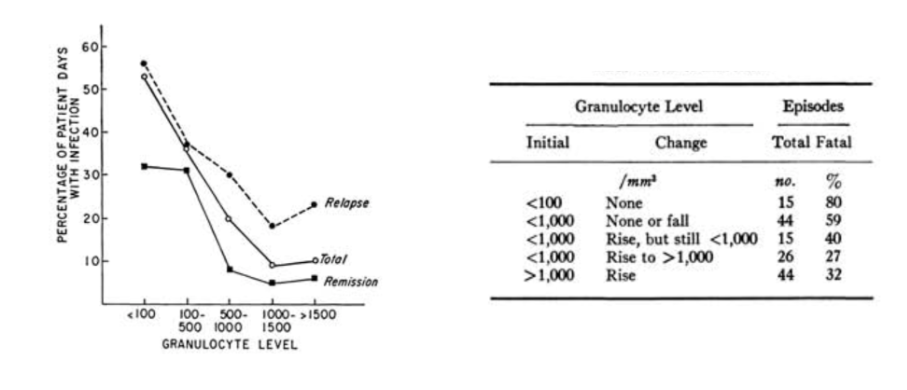
Quantitative relationship of neutropenia
with infection risk
The integument (skin, mucus membranes)
Skin:
- Chemotherapy → hair loss, dryness
- Catheters → direct microbial access
- Broken skin → S. aureus, gram-negatives
Oropharynx:
- Xerostomia + antibiotics → thrush, bacterial overgrowth
Chemotherapy-associated dysbiosis
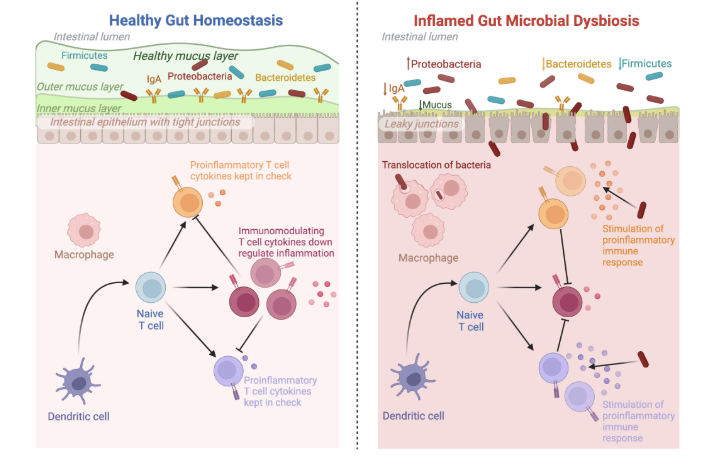
Model of mucosal barrier injury
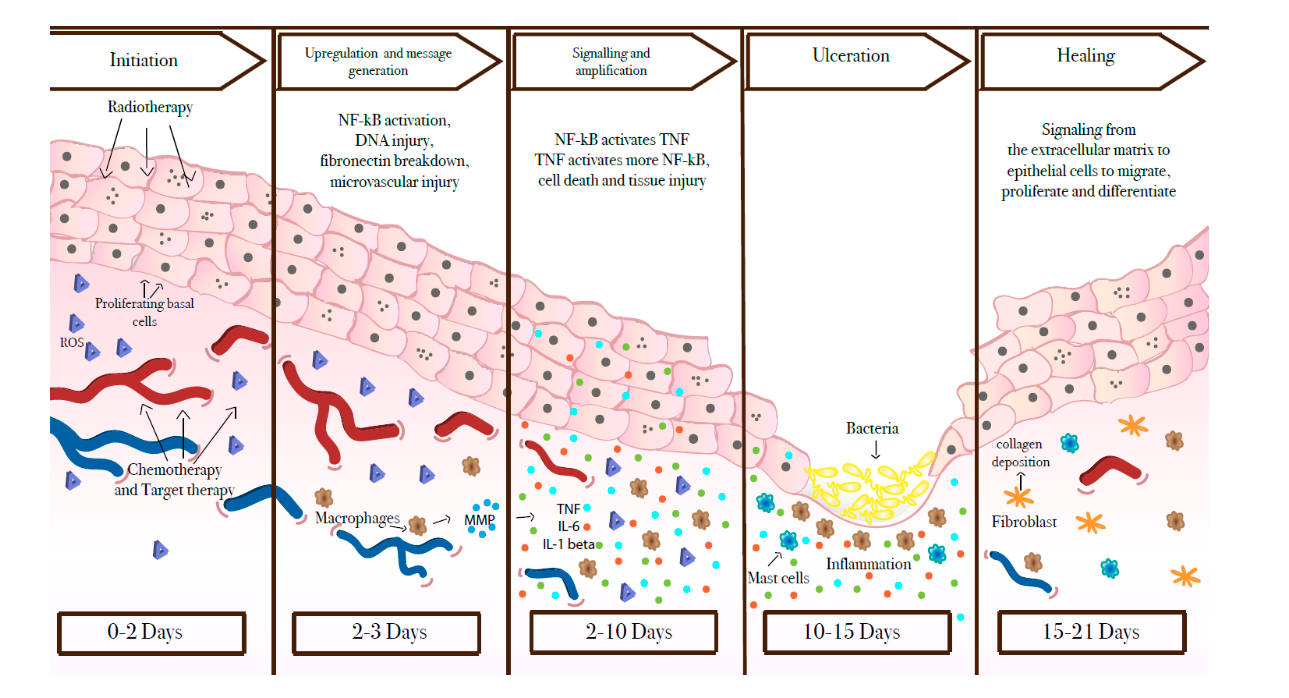
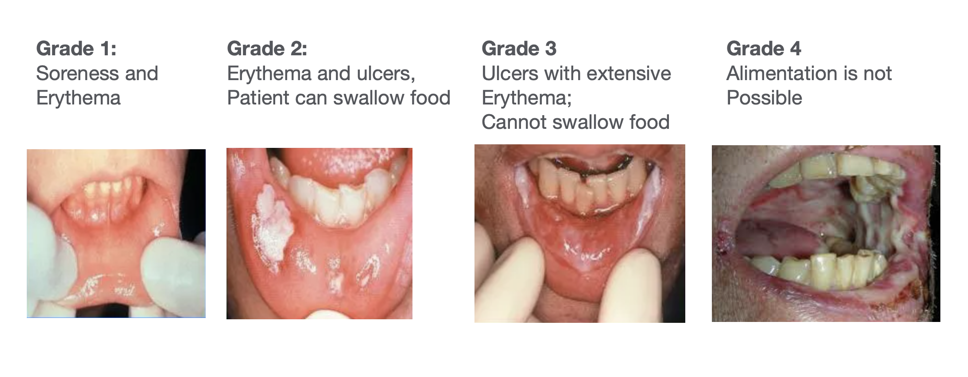
Mucositis
Which pathogens translocate to the bloodstream?
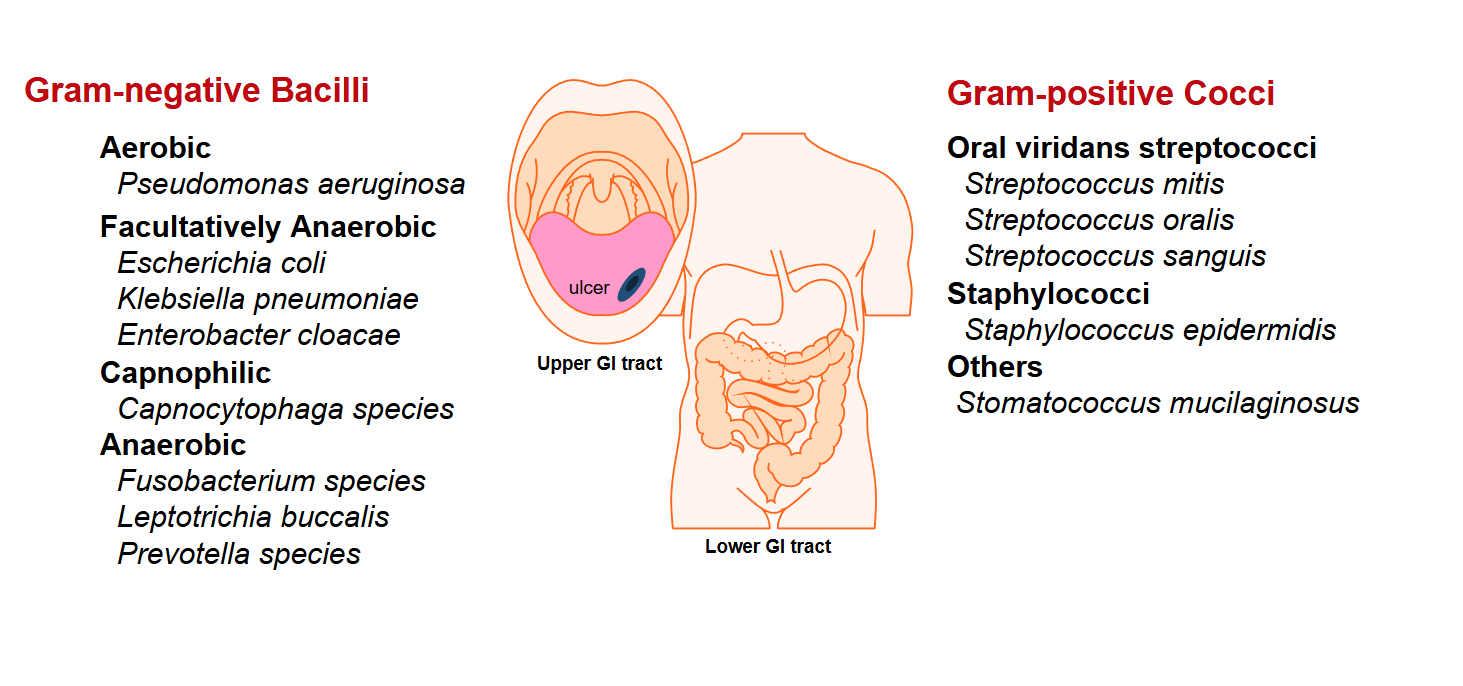
Most common bacterial pathogens
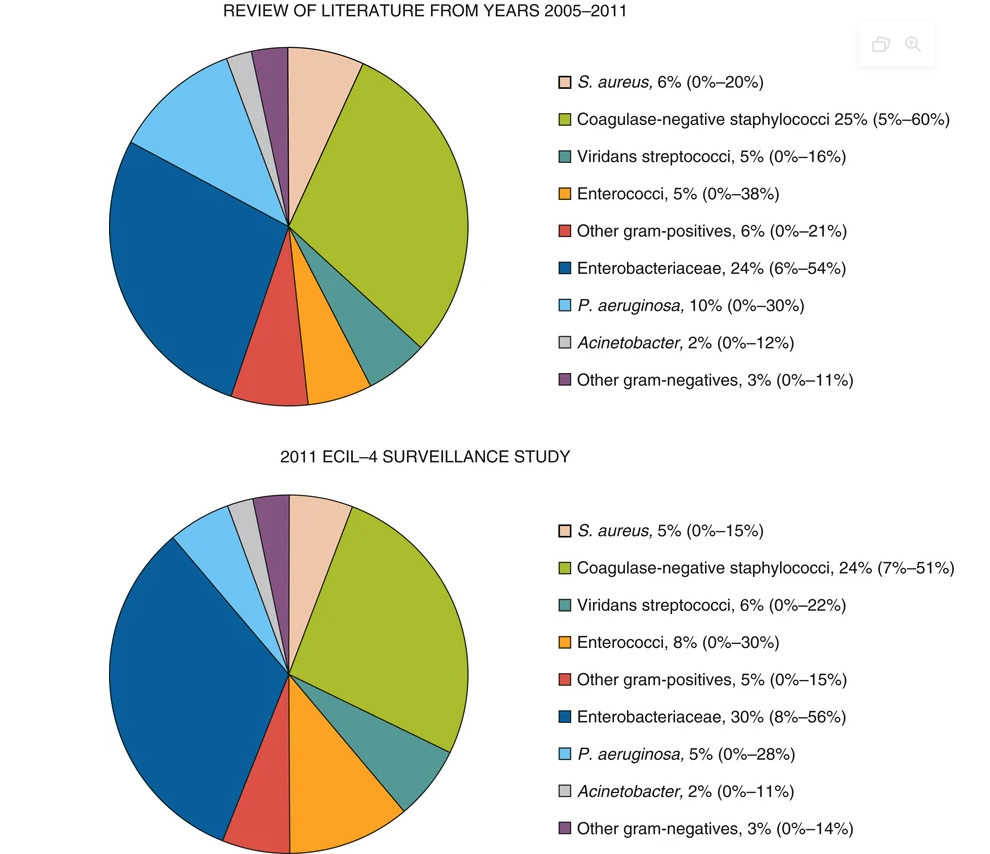
- Infectious source documented in only 20-30% of episodes
- Bacteremia documented in 10-25% of patients with fever
- Aerobic Gram-positive and Gram-negative
CVC-related infection rates
| Catheter Type | Per 100 devices | Per 1000 catheter-days | |
|---|---|---|---|
| Hickman/Broviac |  |
22.5 | 1.6 |
| Port-a-cath |  |
3.5-4 | 0.1 |
| PICC |  |
3.1 | 1.1 |
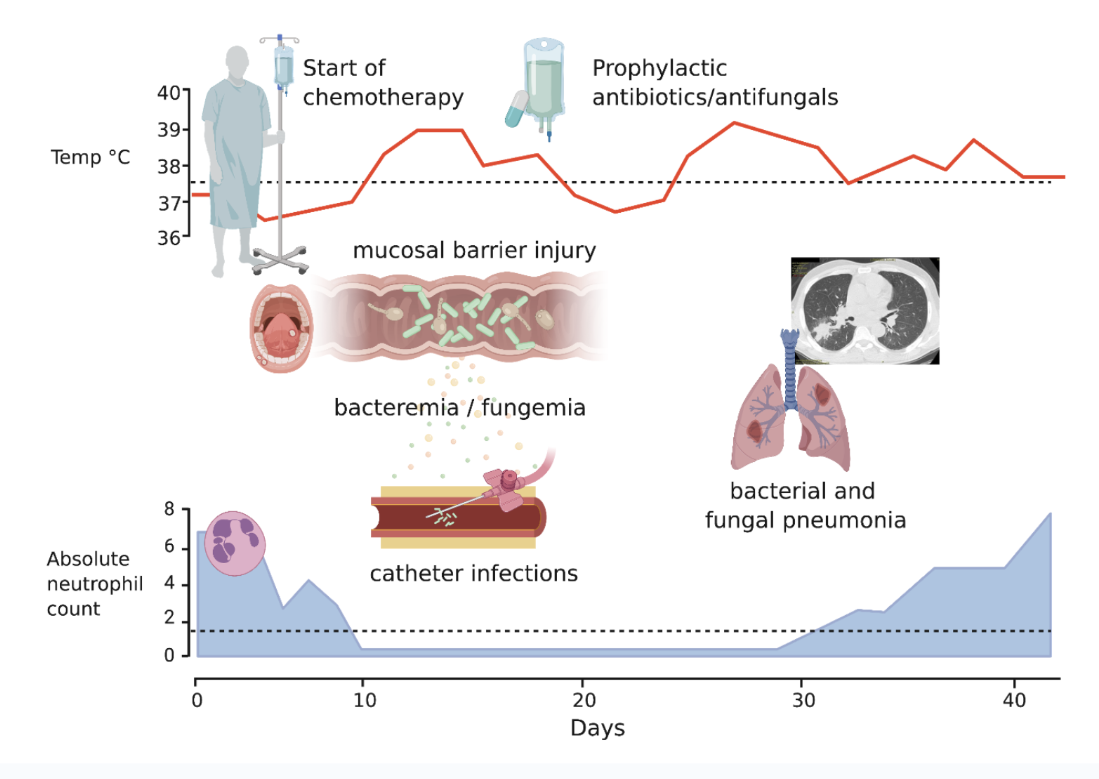
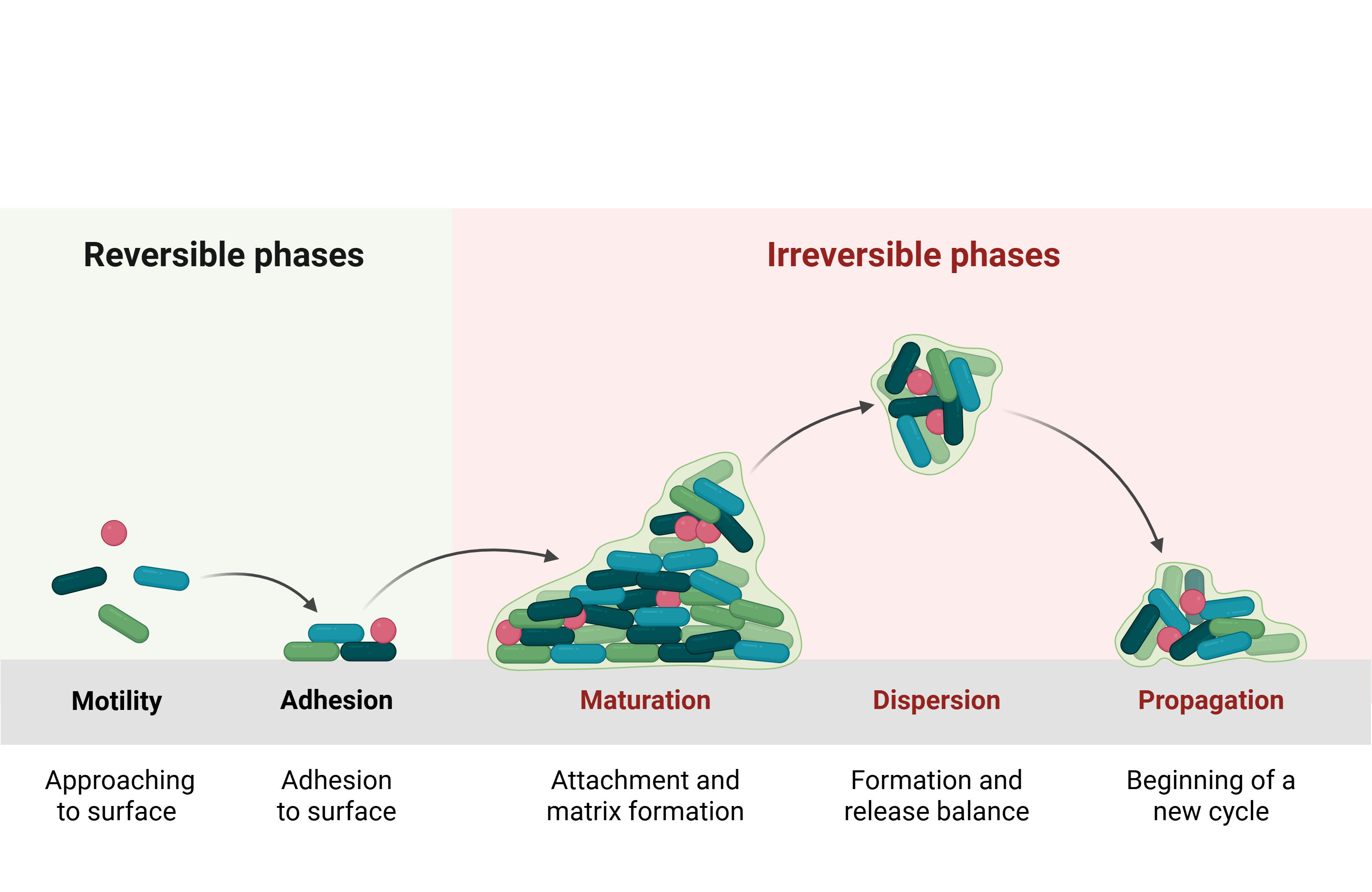
Sequence of infection
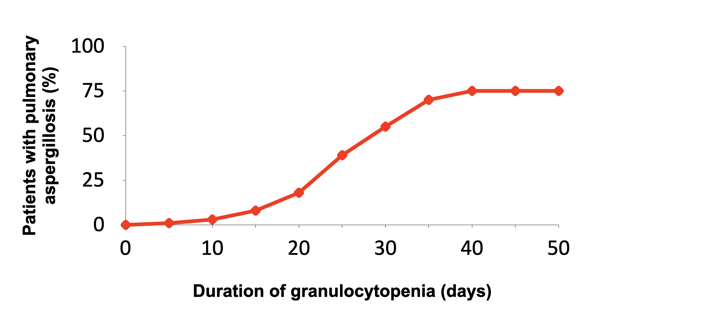
Invasive pulmonary aspergillosis risk vs. neutropenia
Novel targeted therapies: immune sequelae
| Target | Agents
|
B-Cell Depletion
|
T-Cell Depletion
|
HGG1
|
Neutropenia
|
|---|---|---|---|---|---|
| Rituximab | +++ | - | + | ++2 | |
| CD20 | Ofatumumab | +++ | - | + | |
| Obinutuzumab | |||||
| CD52 | Alemtuzumab | ++ | +++ | + | +3 |
| CD38 | Daratumumab | + | + | ||
| SLAMF7 | Elotuzumab | - | - | ||
| CD19/CD3 | Blinatumomab | +++ | + | ++ | ++ |
| Ibrutinib | |||||
| BTK | Acalabrutinib | ++ | + | ||
| Zanubrutinib | |||||
| Idelalisib | |||||
| PI3K | Copanlisib | ++ | + | ||
| Duvelisib | |||||
| JAK | Ruxolitinib | - | |||
| BCL-2 | Venetoclax | - | ++ |
Impaired cell-mediated immunity increases the spectrum of possible pathogens
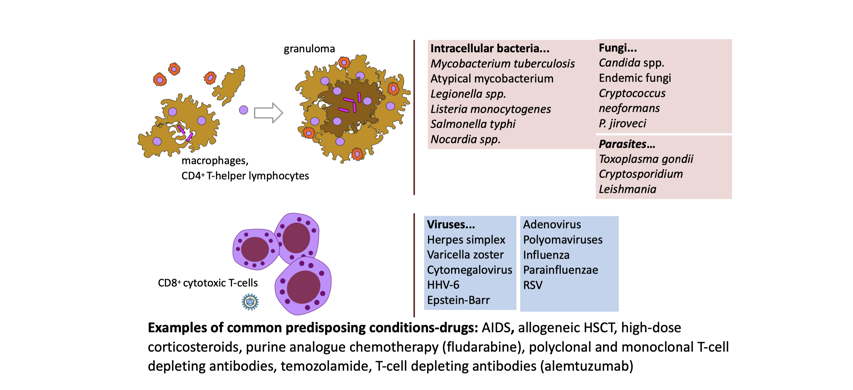
Fungal pathogens
Most Common:
- Aspergillus species > Candida in hematology due to fluconazole prophylaxis that covers yeast but not molds
- Candida species (increasing non-albicans)
Emerging concerns:
- Candida auris - MDR, biofilm-forming
- Azole-resistant Aspergillus fumigatus
- Mucorales (increasing in some centers)

Breakthrough fungal infections on antifungal prophylaxis
Granulocyte-colony stimulating factor (G-CSF)
Primary prophylaxis:
- When febrile neutropenia risk >20%
- Based on age, comorbidities, regimen
Secondary prophylaxis:
- After prior neutropenic complication
- When dose reduction would compromise outcomes
Glycopeptide use (to cover MRSA)

Add vancomycin or alternative (daptomycin) for:
- Suspected catheter-related infection
- Skin/soft tissue infection
- Known MRSA colonization
- Severe sepsis with hypotension
- Pneumonia (or linezolid but not daptomycin)
- Prior MRSA infection
Stop after 48-72h if no gram-positive pathogen identified
Mucormycosis

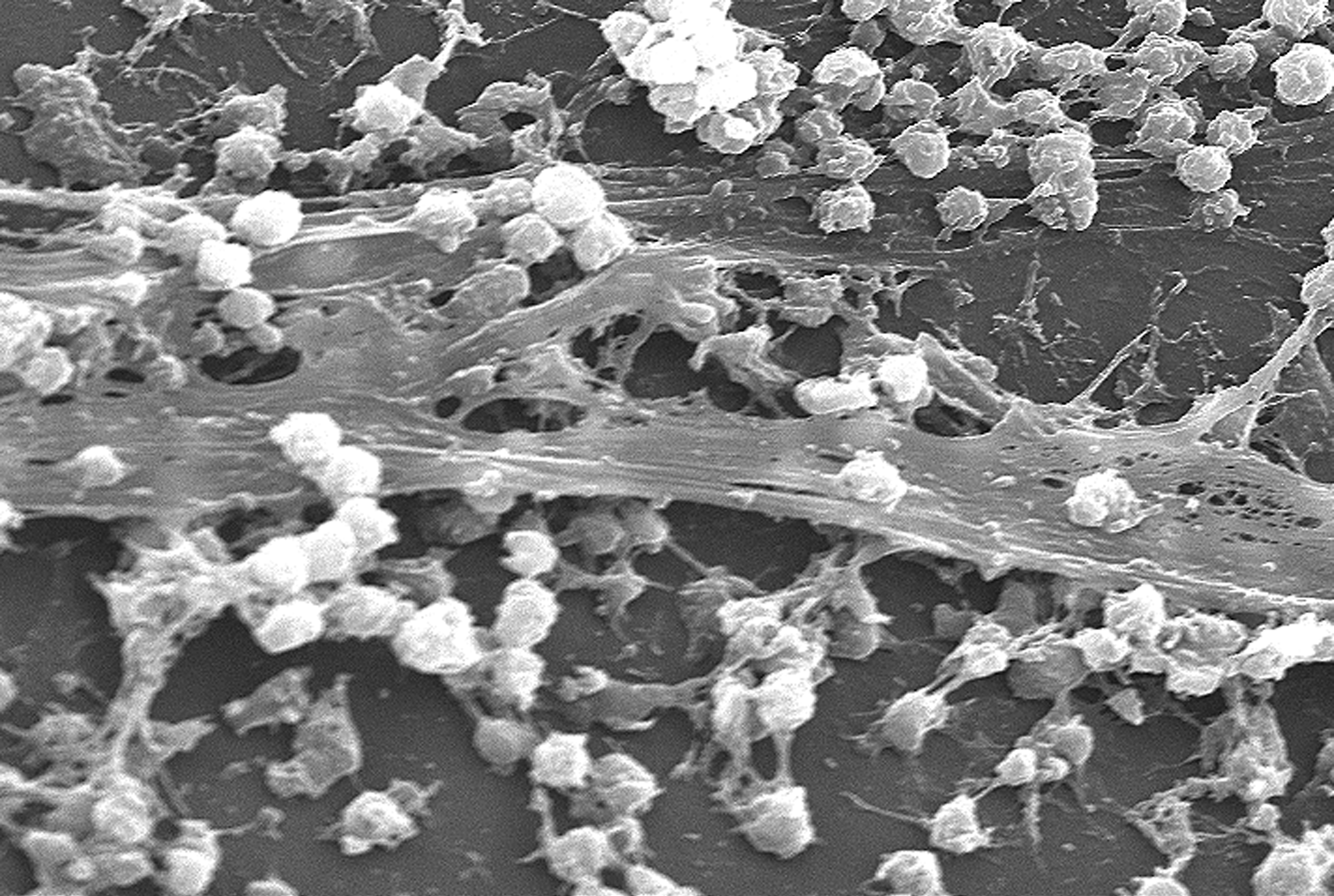
Central venous catheter (CVC) infections
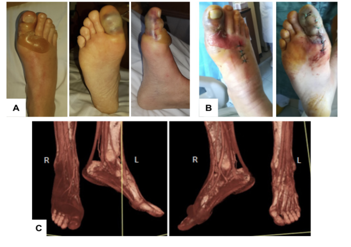
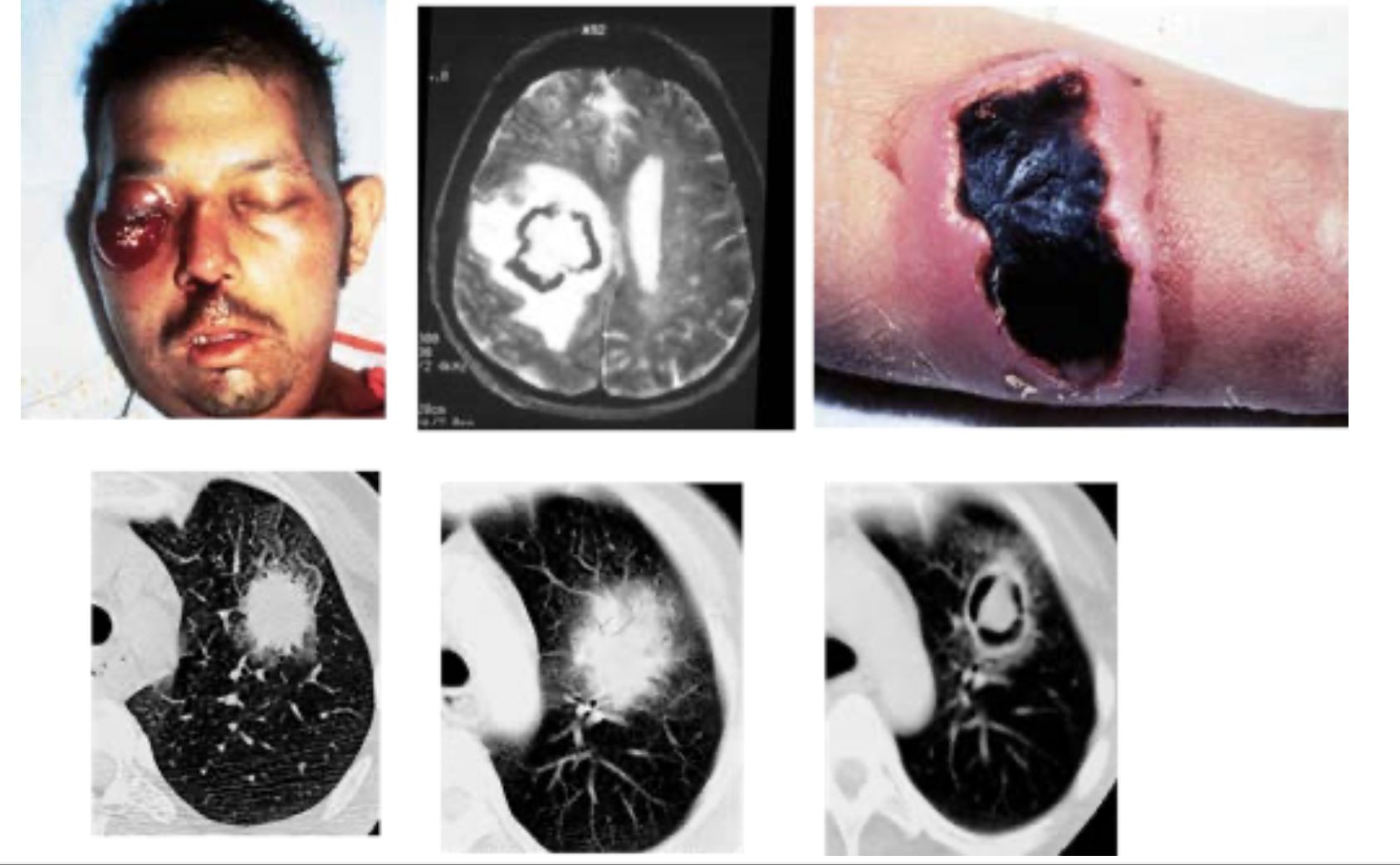
Skin lesions
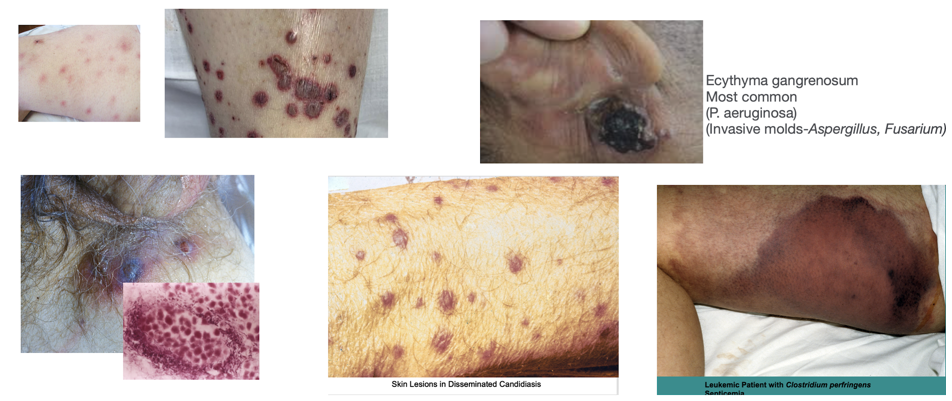
Common presentations:
- Ecthyma gangrenosum — necrotic ulcer with black eschar; classic for P. aeruginosa or invasive molds (Aspergillus, Fusarium)
- Disseminated papules/nodules — Candida, Fusarium, or Aspergillus septate emboli
- Leukemia cutis — infiltration by circulating blasts
- Intravascular hemolysis — rapidly spreading crepitant necrosis from Clostridium perfringens septicemia
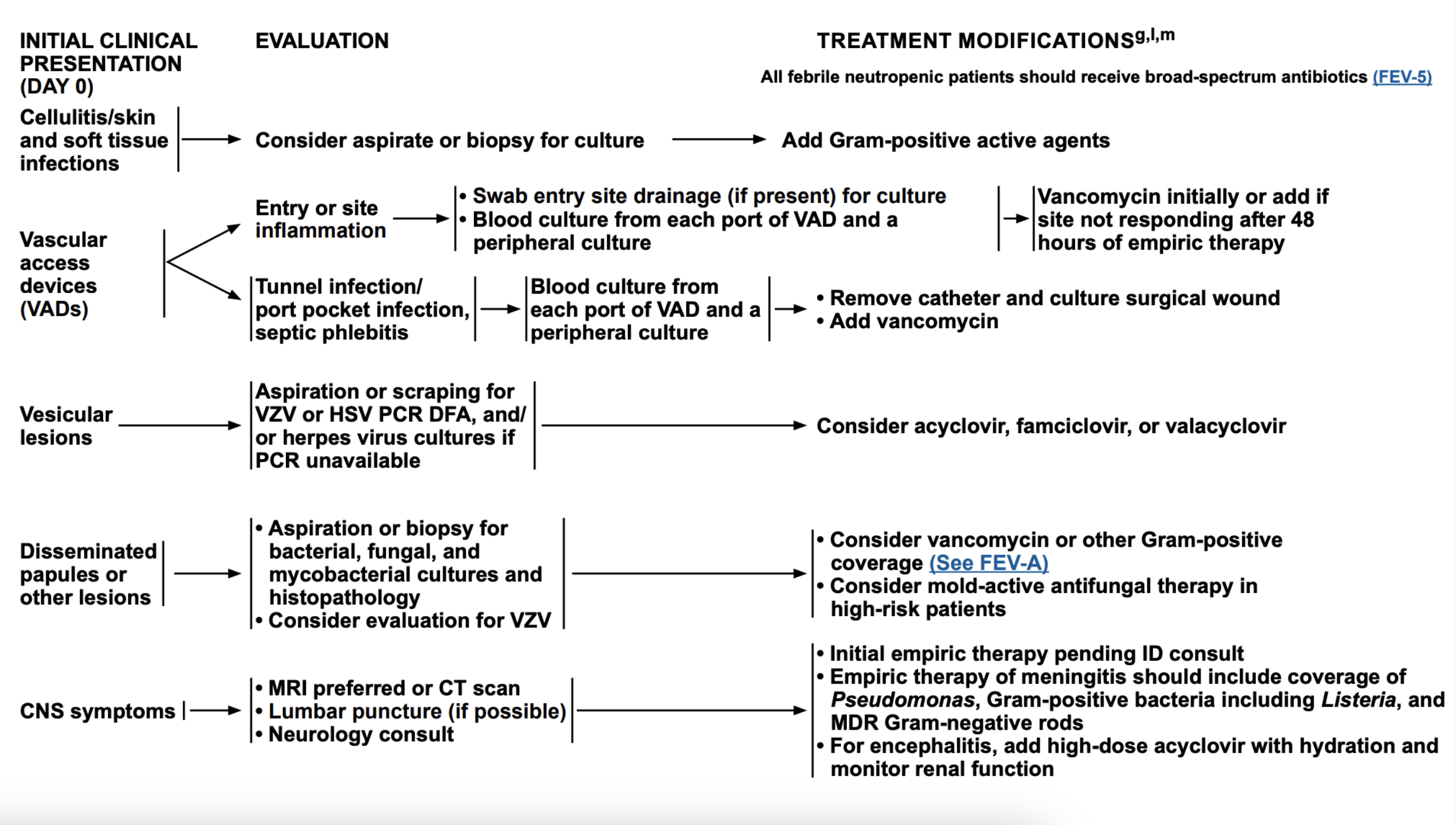
Skin and soft tissue: treatment approach
Oral-Upper GI infections
Candida- Thrush, esophagitis (odynophagia, retrosternal pain)
Vesicular lesions- painful grouped lesions→ulceration

Disseminated HSV- widespread vesicular rash , hepatitis (↑ AST/ALT, sometimes severe), pneumonitis
Pneumonia
up to 60% of patients may have findings of pneumonia on CT
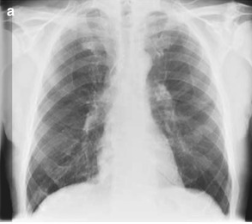
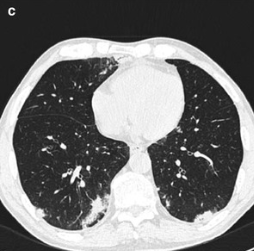
Common CT findings
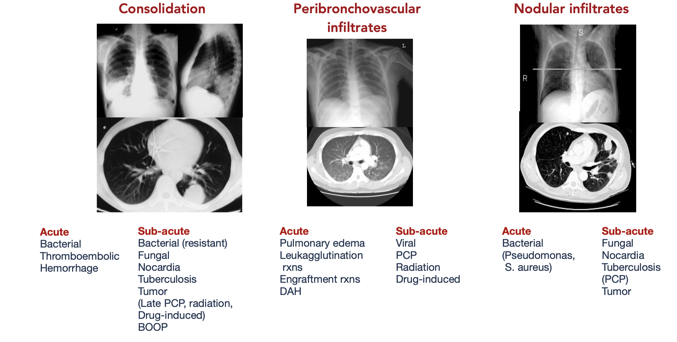
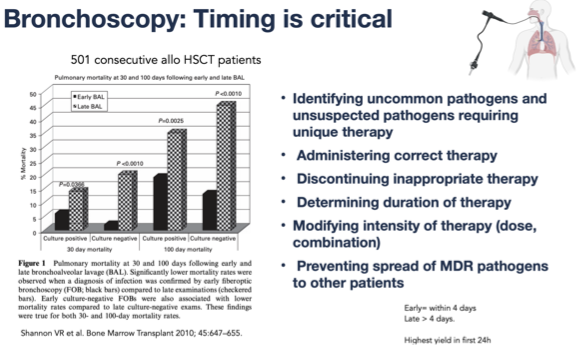
Bronchoscopy
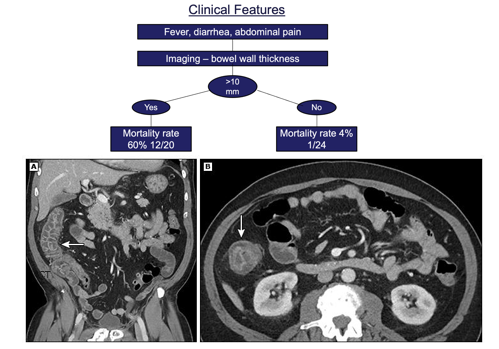
Neutropenic enterocolitis (typhlitis)
Clostridioides difficile colitis
First-line treatment: Stop unnecessary antibiotics →oral vancomycin 125 mg QID for 10 days or fidaxomicin 200 mg BID for 10 days
Fulminant disease: Oral vancomycin 500 mg QID (or via NG tube) combined with IV metronidazole 500 mg TID; →consider rectal vancomycin instillation if ileus is present
Ongoing/worsening CDI: Fidaxomicin if initially treated with vancomycin→ fecal microbiota transplant (if not neutropenic)
CDI resolved but at risk of recurrence: Consider continuing vancomycin or fidaxomicin if diarrhea recurs, and prophylactic vancomycin during subsequent antibiotic courses → taper regimens, fecal transplant (if patient not neutropenic) or bezlotoxumab
