Enteric Infections-Infectious diarrhea
2026-03-01
Enteric Infections- Infectious Diarrhea
Prof. Russell E. Lewis
Department of Molecular Medicine
University of Padua
russelledward.lewis@unipd.it
https://github.com/Russlewisbo
slides available at: www.padovaid.com
 |
Overview of infectious etiologies
- Most diarrhea is viral: stool cultures positive only 1.5-5.6%
- Viral: norovirus (most common), rotavirus, adenoviruses 40/41, astrovirus
- Bacterial: Salmonella, Campylobacter, Shigella, ETEC, EHEC/STEC
- Parasitic: Cryptosporidium, Giardia, Cyclospora, Entamoeba
Norovirus — “The winter vomiting virus”
Key Features
Most common cause of acute gastroenteritis worldwide (Ahmed et al., 2014)
Affects all ages, including highly immune populations
Mean incubation: 24-48 hours - “Winter vomiting disease” (Northern hemisphere)
Norovirus epidemiology & transmission
Viral Characteristics
Non-enveloped RNA virus, Caliciviridae family - Multiple genotypes; no lasting immunity after infection (Patel et al., 2008)
Extremely stable: resists alcohol, chlorine, temperatures to 60°C
Transmission Routes
Primarily fecal-oral >aerosol transmission documented
Fomite transmission (contaminated surfaces)- Can survive environmental conditions for weeks
Rotavirus overview
Epidemiology
Most common cause of severe diarrhea in children worldwide (Parashar et al., 2006) - >100 million cases annually
Approximately 150,000 deaths in children <5 years (Tate et al., 2016)
Peak incidence: 6-24 months age
Clinical Course
Duration 3-8 days , often more severe than norovirus
Dehydration: primary complication
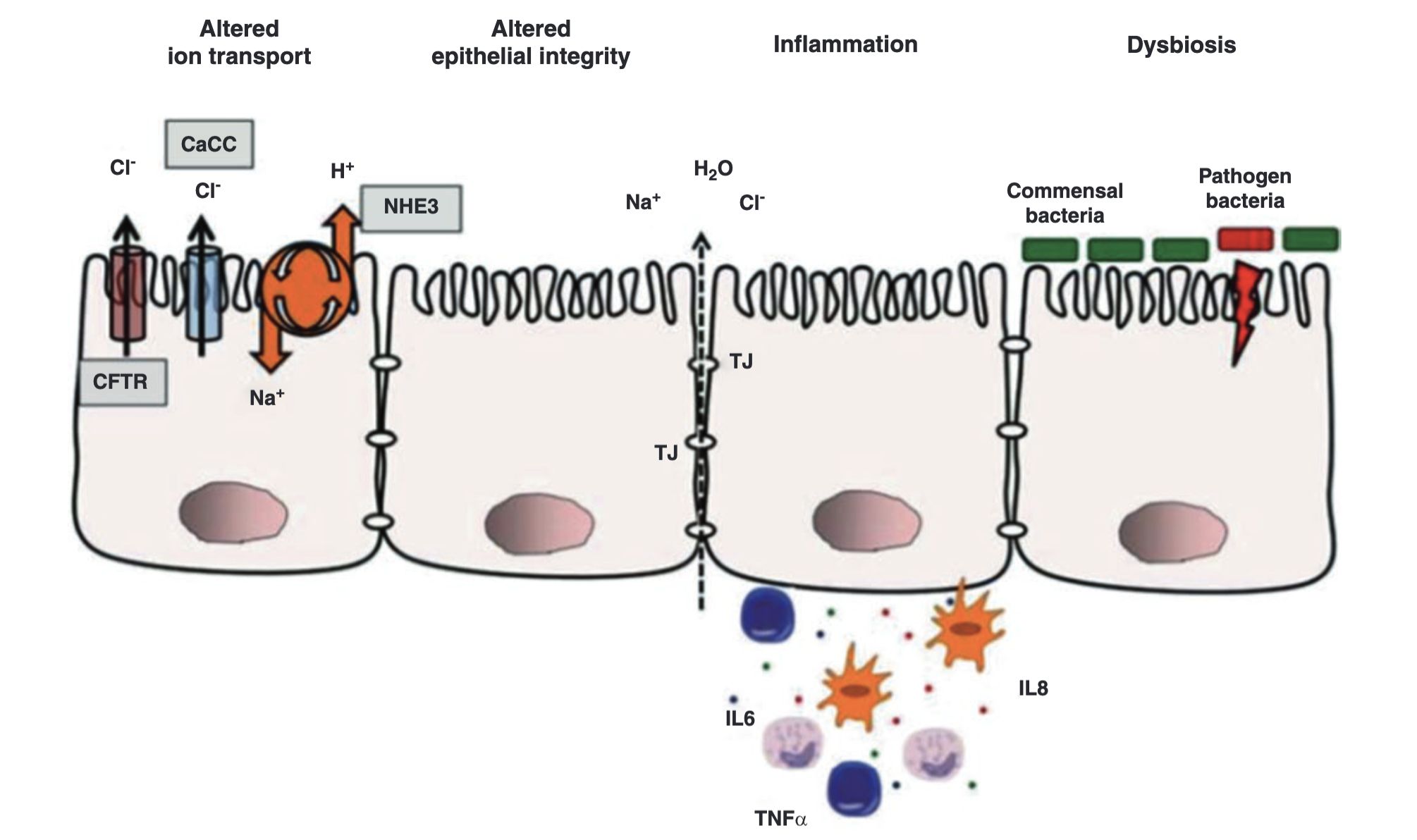
Rotavirus pathophysiology
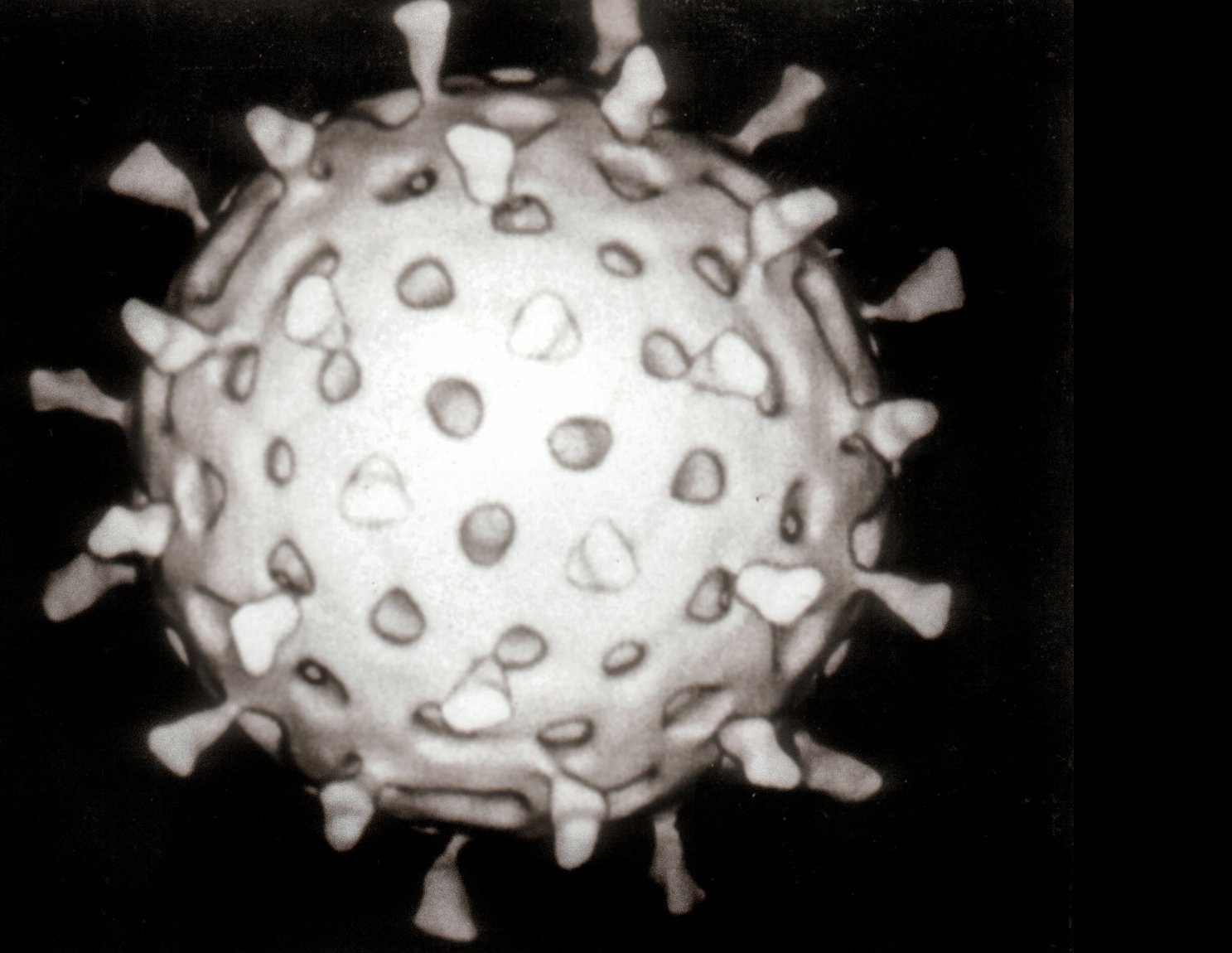
Viral Characteristics
70 nm non-enveloped RNA virus (Reoviridae family)
Segmented genome with multiple genes encoding virulence factors
Mechanisms of Diarrhea - Villus shortening and disruption - Brush-border enzyme deficiency (lactase, sucrase) - Calcium-dependent enterotoxin production (NSP4) - Impaired water and ion absorption
Rotavirus vaccines
Available Vaccines
RotaTeq (Pentavalent) - Manufactured by Merck - 3-dose series - RV1, RV2, RV3, RV4, RV5
Rotarix (Monovalent) - Manufactured by GSK - 2-dose series - RV1 genotype coverage
Impact on Disease:
Dramatic reduction in hospitalizations (>90%) (Ruiz-Palacios et al., 2006; Vesikari et al., 2006)
$1.2 billion in healthcare cost savings in US per year
Significant reduction in mortality globally in vaccinated populations

Enterotoxigenic E. coli (ETEC) overview
Epidemiology & Pathogenesis
Leading cause of acute diarrhea in developing countries (Qadri et al., 2005)
Survives in water; transmitted via contaminated food/water
Produces enterotoxins: heat-labile (LT) and heat-stable (ST) toxins
Clinical Presentation
Watery diarrhea, often dehydrating
Nausea common; vomiting less frequent
Fever absent or mild
Duration typically 3-5 days
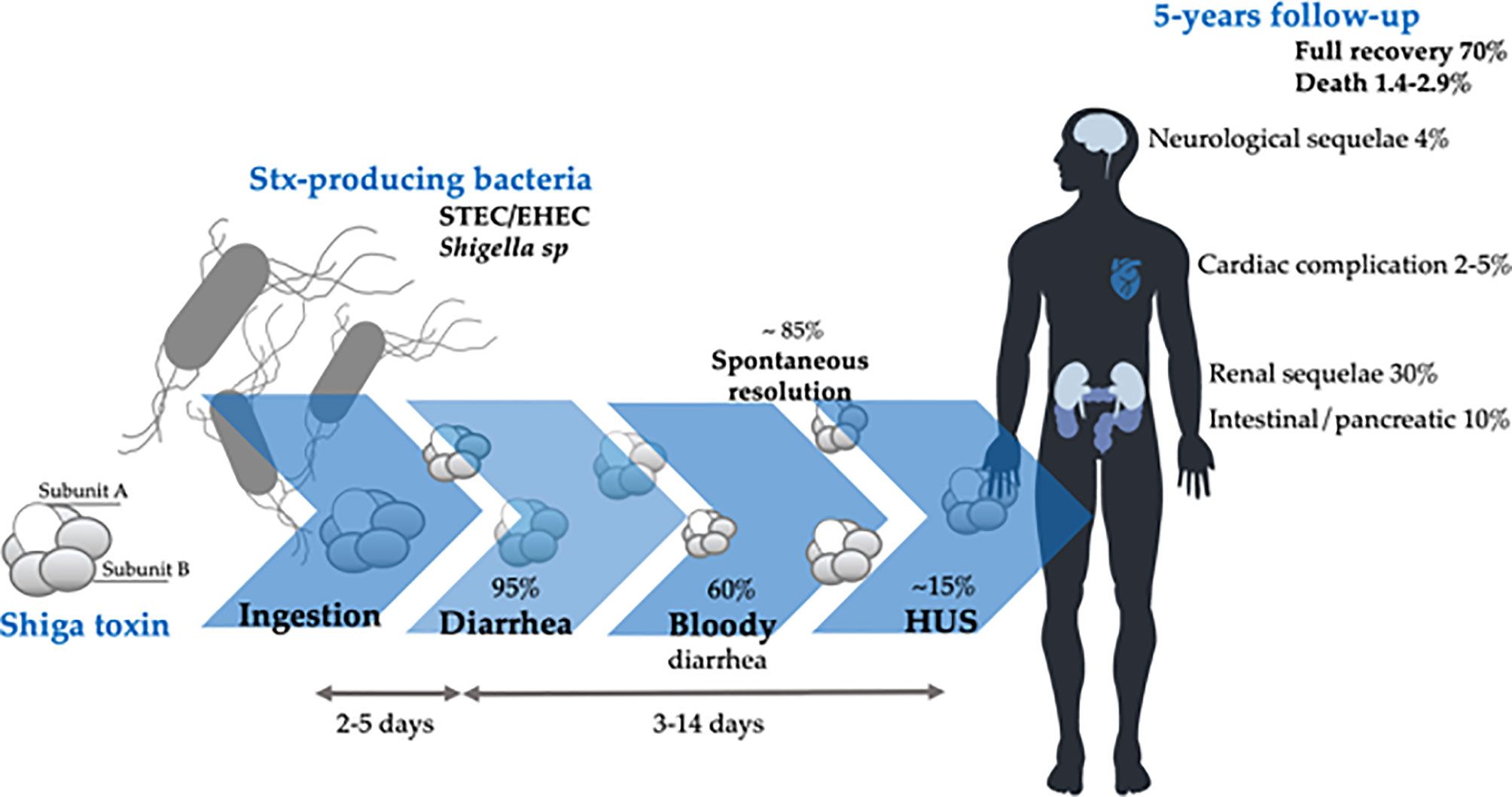
EHEC/STEC overview
Clinical Significance
Shiga toxin-producing E. coli (STEC) strains
E. coli O157:H7 most common in North America (Karch et al., 2005)
Multiple non-motile serotypes cause disease
Shiga toxin causes microangiopathic hemolytic damage (Tarr et al., 2005)
Hemolytic Uremic Syndrome (HUS)
STEC-Associated HUS
Occurs in approximately 5-15% of STEC infections
Often follows 3-5 days of hemorrhagic diarrhea
Triad: microangiopathic hemolytic anemia (schistocytes on blood smear), thrombocytopenia, acute kidney injury
Prognosis and Sequelae
5-year outcomes: ~70% complete recovery Mortality: 1.4-2.9%
Chronic sequelae: renal dysfunction (8-50%), neurological (5-25%), cardiac (5%)
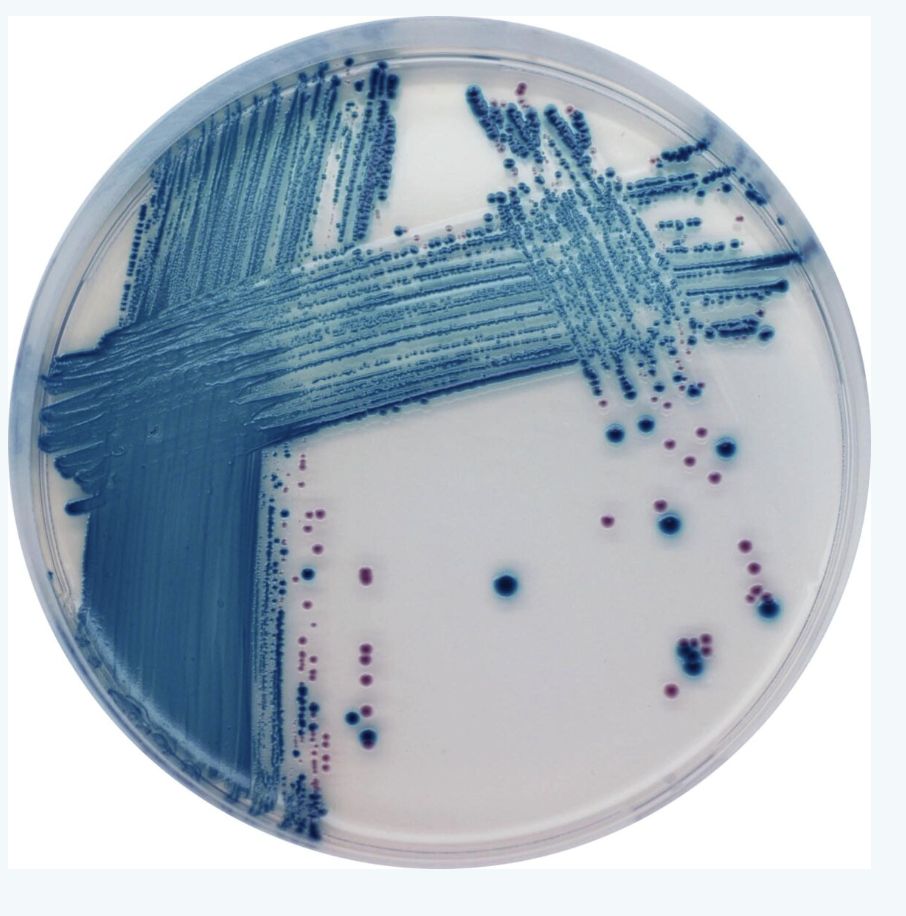
EHEC Detection Methods
Diagnostic Approaches
Sorbitol MacConkey agar: STEC O157:H7 appears non-sorbitol fermenting (colorless)
Chromogenic agar: substrate produces color with specific enzymes
EIA for Shiga toxins: rapid detection from stool
PCR for Stx genes: confirmatory molecular testing
EHEC Outbreaks — Germany 2011
2011 Outbreak Details
Strain: O104:H4 (unusual non-motile strain) (Rasko et al., 2011)
Total infected: 12,600 cases
HUS cases: 4,321
Deaths: 50 (42 from HUS, 8 from sepsis)
Unique Features
Prophage carrying Stx gene plus additional virulence genes
Multidrug resistance including fluoroquinolone resistance
Foodborne outbreak traced to sprouts from Egypt
Deadliest STEC outbreak in modern history

HUS in Italy?
Campylobacter infections

Campylobacter overview
Epidemiology - Most common bacterial cause of gastroenteritis globally (Kaakoush et al., 2015)
- Primarily Campylobacter jejuni (90% of infections) - Also: C. coli, C. lari, and other species
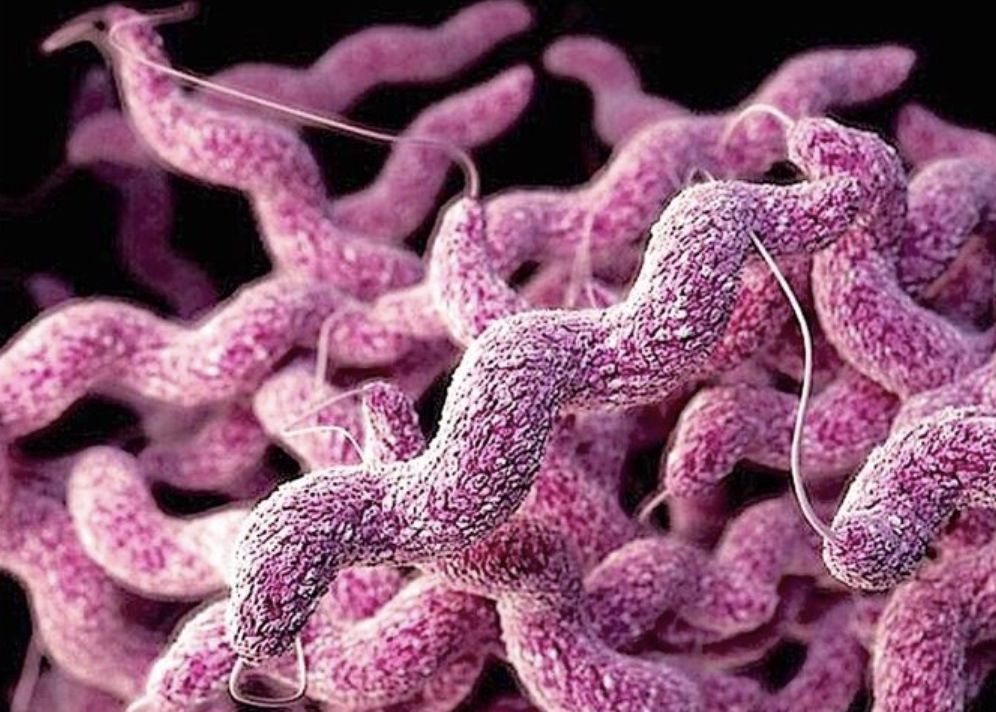
Characteristics
Gram-negative, microaerophilic curved rod
Minimal growth on routine culture media
Fastidious organism; requires special handling

Campylobacter transmission
Animal Reservoir
Common commensal in poultry (colonizes GI tract: 50-90% in GI tract)
- Also found in cattle, pigs, dogs, cats
Undercooked meat: primary source - unpasteurized milk: significant source
Environmental Survival
Survives in freshwater at temperatures <15°C
Sensitive to heat, desiccation, oxygen at room temperature - short survival in food chain; requires careful handling
Direct Transmission
Person-to-person transmission: uncommon but documented
Fecal-oral route primarily - Animal contact risk factor
Campylobacter diagnosis
Laboratory Detection
Stool culture on selective media (Campy agar, CCDA agar) -
Requires microaerophilic conditions
Gram-negative, S-shaped or curved rods on microscopy
Culture takes 48-72 hours minimum
Molecular Methods
PCR increasingly available at reference labs
Rapid diagnosis possible
Higher sensitivity than culture
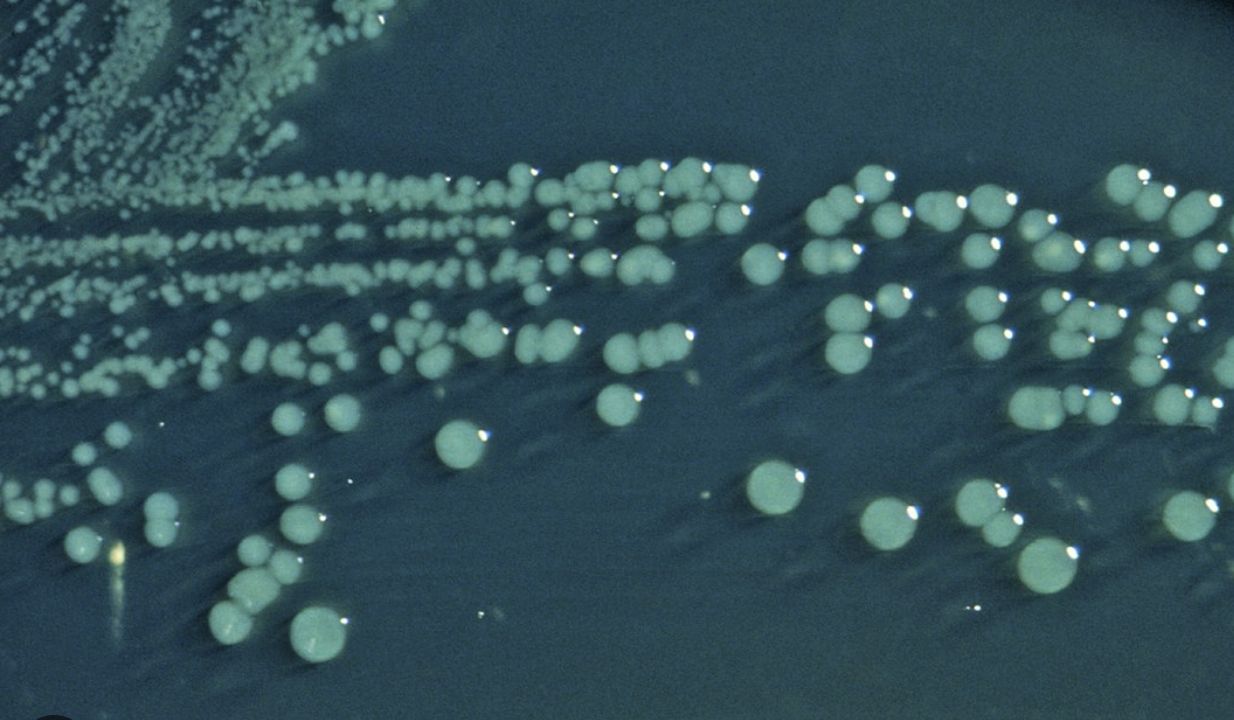
Salmonella infections

Non-typhoidal Salmonella transmission

Non-typhoidal Salmonella clinical features
Incubation Period : 8-72 hours (typically 12-36 hours)
Typical Presentation :
Diarrhea with abdominal pain and cramping
Fever in ~50% (often high—>39°C)
Nausea and vomiting common
Systemic symptoms: malaise, headache
Risk Factors for Severe Disease
- Extremes of age (<5 or >65 years)
- Achlorhydria or antacid use, Inflammatory bowel disease
- Sickle cell disease, immunosuppression
Prognosis
Self-limited in immunocompetent hosts, bacteremia in <5% (higher with underlying conditions)
Duration typically 4-7 days
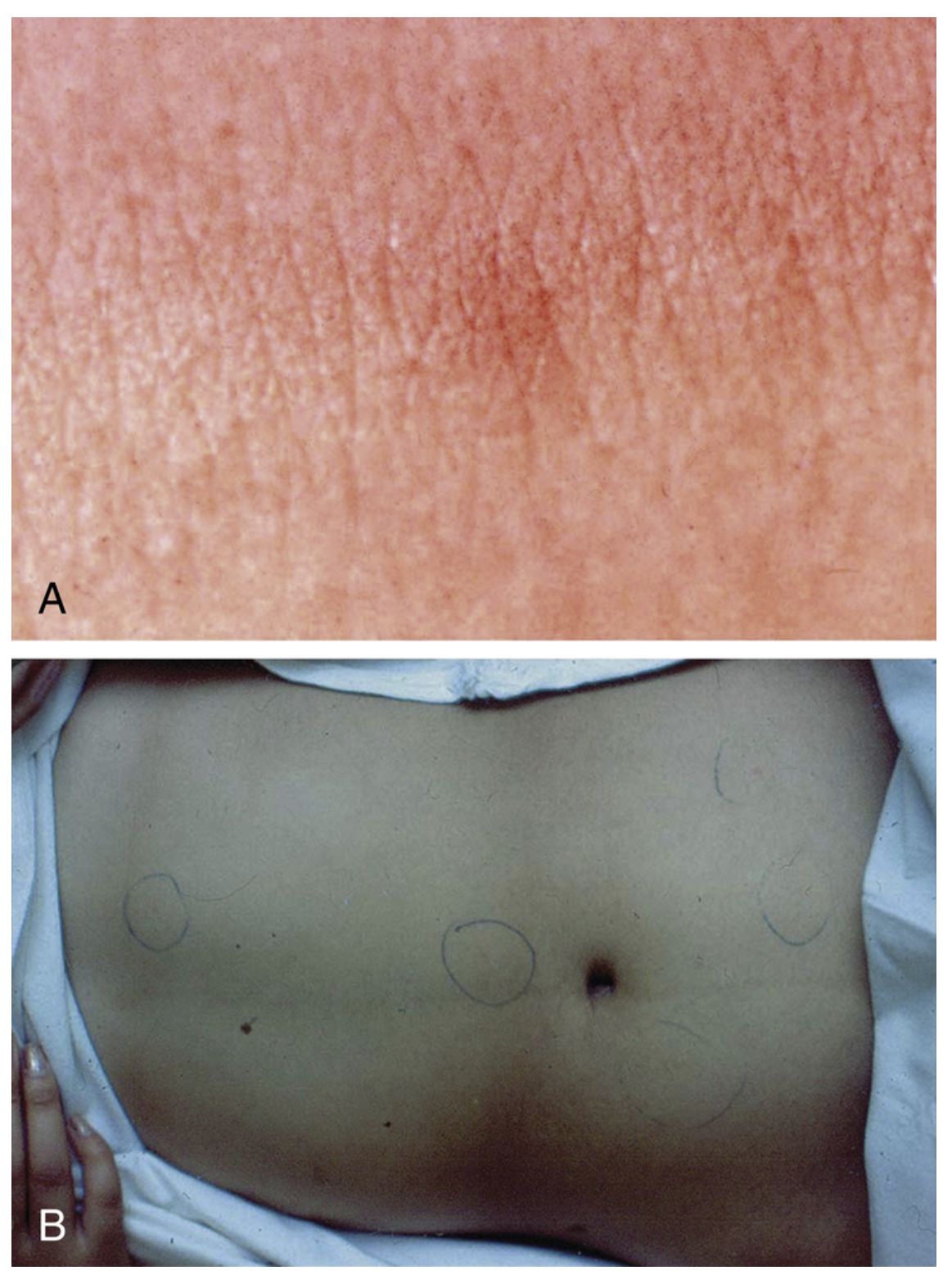
Typhoid fever — Clinical progression
Week 1: Septicemia Phase
- Gradual fever onset (prodrome over days)
- High fever develops, continuing to rise
- Bacteremia present
- Relative bradycardia (unusual for degree of fever)
- Malaise, headache, myalgias
Week 2-3: Systemic Phase
- Sustained high fever (often continuous pattern—“staircase fever”)
- Rose spots rash (evanescent, 2-3mm rose-colored papules on trunk)
- Hepatosplenomegaly with abdominal pain and distension, diarrhea or constipation
Week 3-4: Crisis Phase
Risk of intestinal perforation (Peyer’s patches ulcerate)
Septic shock possible
Delirium and altered mental status (“typhoid state”)
Myocarditis, pneumonia
Shigella pathophysiology and complications
Virulence Mechanisms
Invasion of colonic epithelium (ipaB, ipaC genes)
Intracellular multiplication - abscess formation and mucosal ulceration
Enterotoxin production: ShET1, ShET2
Complications
Shiga toxin produced by S. dysenteriae → HUS possible - HUS occurs in ~8% of children with S. dysenteriae infection
Toxic megacolon (rare)
Protein-calorie malnutrition from persistent diarrhea
Seizures, febrile delirium (especially in children)
Yersinia
Species of clinical importance:
- Yersinia enterocolitica - Yersinia pseudotuberculosis
Key characteristics - Zoonotic infections: wild and domestic animals
Transmission: undercooked pork, contaminated water
Can survive refrigeration (cold enrichment aids culture)
Clinical features : Watery diarrhea or dysentery
Distinctive: pharyngitis in ~20% (pharyngitis-gastroenteritis pattern)
Acute mesenteric lymphadenitis: can mimic appendicitis
Fever and abdominal pain prominent
Can cause arthralgia (particularly HLA-B27 associated)
Lab diagnosis - Culture on selective media (CIN agar)
- Overgrowth by normal flora; requires selective medium or cold enrichment

John Snow- Birth of medical epidemiology

Vibrio cholerae
Epidemiology
- Endemic in South Asia (particularly Bangladesh, India) (Sack et al., 2004)
- Seventh pandemic ongoing since 1961
- Transmitted via contaminated water in areas with poor sanitation
- Epidemic potential high; 3-5 million cases, 100,000-300,000 deaths annually (Ali et al., 2015)
Clinical Presentation
- Acute watery non-bloody diarrhea
- Characteristic “rice-water stools” (clear, watery, with flecks)
- Severe dehydration and shock possible
- Vomiting common
- Can be fulminant with progression to hypovolemic shock

Cholera management
Diagnostic approach
Culture on TCBS (Thiosulfate-Citrate-Bile Salts) agar
Oxidase-positive, gram-negative curved rods
PCR available at reference labs
Treatment
Fluid replacement is paramount!!!
Oral rehydration solution (ORS) is first-line
IV fluids (normal saline or Ringer’s lactate) for severe dehydration
Replacement volumes can be massive (10-20 L/day in severe cases)
Monitor for electrolyte abnormalities
Antimicrobial therapy
Decreases duration and volume of diarrhea
Doxycycline, fluoroquinolones, or azithromycin
Secondary to fluid replacement in priority
Prevention - Vaxchora: oral cholera vaccine for travelers to endemic areas
- Provides ~90% protection for 3 months, wanes thereafter - Food and water precautions essential

Traveler’s diarrhea — Overview
Epidemiology
Affects 300-500 million travelers annually
Attack rate varies by destination: 5-50% depending on region (Steffen et al., 2015)
Onset typically 5-15 days after arrival in endemic region
Duration usually 1-5 days (self-limiting in 90%)
Clinical Presentation
Watery diarrhea most common (80%)
Some bloody stools possible (10-20%)
Fever in 20-30%
Cramping abdominal pain
Systemic symptoms mild
Definition
≥3 unformed stools in 24 hours plus 1+ GI symptom
Occurring in someone traveling to area of higher risk

Traveler’s diarrhea — Prevention
Food and water precautions
Drink bottled or boiled water
Avoid ice, raw vegetables, raw/undercooked meat
Peel own fruits
Avoid street food and unpasteurized dairy
Antimicrobial prophylaxis
Not routinely recommended (resistance, adverse effects)
Consider for high-risk patients (immunocompromised, severe underlying disease)
Bismuth subsalicylate: effective prophylaxis (2 tablets QID)
Duration: maximum 3 weeks
