Carbapenems, Carbapenem/β-Lactamase Inhibitor Combinations, and Aztreonam
Russell E. Lewis
2026-05-13
Carbapenems,
Carbapenem/β-Lactamase Inhibitors,
and Azteonam
Russell E. Lewis
Associate Professor of Infectious Diseases

russelledward.lewis@unipd.it
https://github.com/Russlewisbo
Slides and course materials: www.idpadova.com
Learning objectives
- Describe the mechanism of action and structure-activity relationships of carbapenems
- Compare the spectrum of activity, pharmacokinetics, and clinical uses of ertapenem, imipenem, and meropenem
- Explain the role of vaborbactam and relebactam in restoring carbapenem activity
- Identify the resistance mechanisms that limit carbapenem efficacy
- Apply PK/PD principles to optimize carbapenem dosing
- Define the unique role of aztreonam in β-lactam allergy and MBL-producing infections
Chemistry
Carbapenem core structure
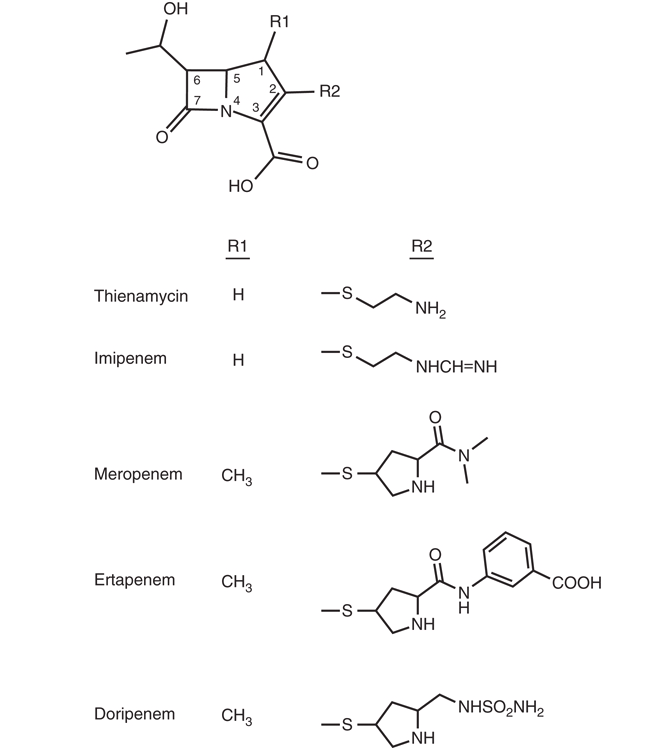
- Derivatives of thienamycin (Streptomyces cattleya)
- Differ from penicillins: carbon replaces sulfur at position 1, double bond between C2 and C3
- Trans-1α-hydroxyethyl side chain at C6 → stability against ESBLs and AmpC β-lactamases
- The broad spectrum of carbapenems is directly linked to this structural stability
From thienamycin to clinical agents
- Thienamycin: too chemically unstable for clinical use
- Imipenem: N-formimidoyl derivative of thienamycin
- Degraded by renal DHP-I → requires cilastatin
- Meropenem & ertapenem: 1β-methyl substituent at C2
- Stable to DHP-I → no cilastatin needed
- Doripenem: available outside the US
Mechanism of Action
PBP binding profile
- Carbapenems inhibit cell wall synthesis by binding to PBPs
- Preferential binding: PBPs 1a, 1b, 2, and 4
- Lesser binding to PBP3 (the main target of aminopenicillins and cephalosporins)
- Multi-PBP binding → broad spectrum of activity
Outer membrane penetration
- Carbapenems cross the gram-negative outer membrane through specific OMPs
- OprD (P. aeruginosa): imipenem’s primary entry portal
- OmpK35/OmpK36 (K. pneumoniae)
- OmpC/OmpF (Enterobacter spp.)
- Loss of these porins contributes to resistance
Time-dependent killing
- Carbapenems display time-dependent bactericidal activity
- Key PK/PD parameter: fT>MIC
- Target: 50%–100% of the dosing interval
- Clinical implication: extended or prolonged infusions optimize this target
Resistance Mechanisms
Overview of carbapenem resistance
Four principal mechanisms:
- β-Lactamase production (most common in gram-negatives)
- Diminished permeability (porin loss/modification)
- Efflux pump upregulation
- Altered PBP targets (primarily gram-positives)
β-Lactamase-mediated resistance
Class A (KPC carbapenemases): Serine-based; K. pneumoniae carbapenemase is the most important globally
Class B (Metallo-β-lactamases/MBLs): Zinc-dependent; hydrolyze ALL carbapenems; NO clinically available BLI inhibits them
Class D (OXA-type): Found frequently in A. baumannii; emerging in Enterobacterales
Class A carbapenemases: KPC
Klebsiella pneumoniae carbapenemase (KPC)
Most important carbapenem resistance determinant worldwide
Predominantly in K. pneumoniae, but spreading to other species
Inhibited by: avibactam, vaborbactam, relebactam
Not inhibited by: clavulanic acid, tazobactam, sulbactam
Class B: Metallo-β-lactamases
- Zinc-dependent enzymes (NDM, VIM, IMP)
- Hydrolyze ALL β-lactams except aztreonam
- No clinically available BLI inhibits MBLs
- Treatment strategy: aztreonam + ceftazidime-avibactam
- Intrinsic MBLs in S. maltophilia, E. meningoseptica
Class D: OXA-type carbapenemases
- Found predominantly in Acinetobacter baumannii
- OXA-48-like enzymes emerging in Enterobacterales
- Generally not inhibited by vaborbactam or relebactam
- Limited treatment options
Porin-mediated resistance in P. aeruginosa
- OprD loss: Major contributor to carbapenem resistance
- Imipenem: OprD is the primary entry portal → most affected by OprD loss
- Meropenem: less dependent on OprD → less affected
- OprD loss often occurs during therapy
Efflux-mediated resistance
- MexA-MexB-OprM system in P. aeruginosa
- Meropenem is a substrate; imipenem is NOT
- Upregulation → increased meropenem resistance
- Combined with OprD loss → high-level resistance to both agents
Porin-mediated resistance in enterobacterales
- OmpK35/OmpK36 loss in K. pneumoniae
- OmpC/OmpF loss in Enterobacter spp.
- Often combined with β-lactamase production
- Contributes to resistance even without carbapenemase production
PBP-mediated resistance in Gram-positives
- Low-affinity PBP targets → class-wide β-lactam resistance
- PBP2a in MRSA → carbapenem resistance
- PBP5 in E. faecium → carbapenem resistance
- 40%–50% of S. aureus strains are MRSA
- 60%–80% of E. faecium strains are ampicillin-resistant
PBP binding resistance
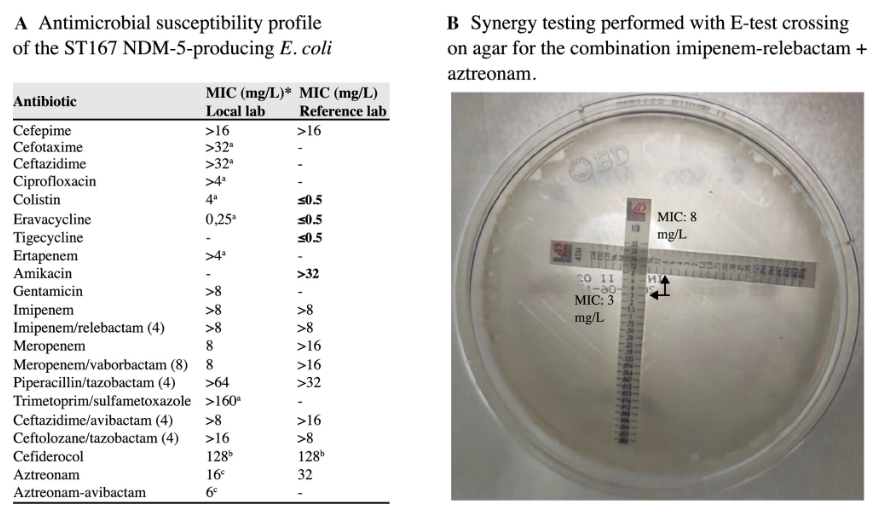
A 65-year-old man without identifiable risk factors for multidrug-resistant pathogens was admitted with peritonitis, isolating NDM-producing Escherichia coli from a rectal swab and intraoperative samples.
After surgery, ceftazidime-avibactam/aztreonam was administered. Due to poor clinical response, he was switched to imipenem-relebactam/aztreonam, resulting in a successful outcome.
Whole-genome sequencing detected blaNDM-5 and blaCMY-148 β-lactamases, PBP3 YRIN insertion, and mutated cirA gene.
This case illustrates the importance of considering different mechanisms of resistance when choosing combination therapy.
PBP-mediated resistance in MDR strains
PBP3 four-amino-acid insertions (typically YRIN or YRIK between residues 333–334 in the β2b–β2c loop, adjacent to the transpeptidase active site) reduce susceptibility to PBP3-targeting β-lactams (aztreonam, cefepime, ceftazidime).
First described in 2015 with reduced aztreonam–avibactam susceptibility, these insertions are now common in globally disseminated high-risk E. coli lineages (ST167, ST405, ST410, ST648), which frequently co-carry NDM metallo-β-lactamases plus CMY cephalosporinases or CTX-M ESBLs.
Many β-lactams rely predominantly on PBP3 inhibition and are therefore vulnerable to these target alterations; carbapenems, with broader PBP binding, are less affected — though carbapenem–β-lactamase inhibitor combinations differ in their behavior.
Whole-genome sequencing is needed to rapidly detect uncommon resistance genotypes such as PBP3 insertions and guide rational combination therapy.
Carbapenem-Resistant Enterobacterales
CRE: A growing threat
- Increasing incidence of CRE worldwide
- Multiple resistance mechanisms: carbapenemases, porin mutations, ESBL/AmpC + porin loss, efflux
- Detection challenges in routine diagnostic labs
- 2011: CLSI decreased carbapenem breakpoints fourfold
Why breakpoints changed
- Higher 2010 breakpoints missed resistance mechanisms
- Revised breakpoints negate need for routine carbapenemase detection (mCIM, Carba NP)
- But: confirming carbapenemase genes may still guide treatment
- KPC → meropenem-vaborbactam preferred
- MBL → aztreonam + ceftazidime-avibactam
- OXA-48 → ceftazidime-avibactam
Carbapenem-BLI Combinations
Two new combinations
| Feature | Meropenem-Vaborbactam (Vabomere) | Imipenem-Relebactam (Recarbrio) |
|---|---|---|
| Approval year | 2017 | 2019 |
| BLI class | Cyclic boronic acid | Diazabicyclooctane |
| Inhibits KPC | Yes (potently) | Yes |
| Inhibits AmpC | Yes | Yes |
| Inhibits MBL | No | No |
| Inhibits OXA-48 | No | No |
Meropenem-vaborbactam
- Dose: 4 g IV q8h via 3-hour infusion (2 g meropenem + 2 g vaborbactam)
- Vaborbactam designed specifically to bind KPC
- Preferred agent for KPC-producing CRE (IDSA 2023 guidance)?
- Vaborbactam does NOT enhance activity vs P. aeruginosa (unless carbapenemase present)
- Dose adjustment based on MDRD formula
Imipenem-relebactam
- Dose: 1.25 g IV q6h via 30-minute infusion (500 mg imipenem + 500 mg cilastatin + 250 mg relebactam)
- Relebactam inhibits AmpC → restores imipenem activity vs P. aeruginosa
- Emerging role: difficult-to-treat P. aeruginosa
- AmpC drives resistance to imipenem more than meropenem
- Can also be used for KPC-producing CRE (less clinical data)
PK/PD of the BLI components
- Vaborbactam: %fT>CT is the PK/PD driver; target threshold ~8 μg/mL
- Relebactam: AUC/MIC ratio drives efficacy
- Both BLIs require renal dose adjustment
- 3-hour infusion for meropenem-vaborbactam optimizes both components
Antibacterial activity
MIC90 comparison: Gram-positive cocci
Comparative Activity of Ertapenem, Imipenem, and Meropenem (MIC90, μg/mL)a
| Organism | Ertapenem | Imipenem | Meropenem |
|---|---|---|---|
| S. aureus, oxacillin-susceptible | 0.25 | 0.12 | 0.12 |
| S. aureus, oxacillin-resistant | >16 | >16 | >16 |
| CoNS, oxacillin-susceptible | 0.25 | 0.12 | 0.12 |
| CoNS, oxacillin-resistant | >16 | >16 | >16 |
| Streptococcus pneumoniae | 0.06–0.5 | 0.06–0.25 | 0.06–1 |
| β-Hemolytic streptococci | 0.06 | 0.06 | 0.06 |
| Viridans group streptococci | 0.12 | 0.03 | 0.03 |
| Enterococcus faecalis | 8 | 1 | 8 |
| Enterococcus faecium | >8 | >8 | >8 |
| Bacillus anthracis | —b | 0.12 | 0.05 |
| Listeria monocytogenes | 0.25 | 0.06 | 0.12 |
MIC90 Comparison: Gram-negative cocci & enterobacterales (1)
| Organism | Ertapenem | Imipenem | Meropenem |
|---|---|---|---|
| Haemophilus influenzae | 0.03 | 0.25 | 0.06 |
| Moraxella catarrhalis | 0.03 | 0.25 | 0.03 |
| Neisseria gonorrhoeae | 0.06 | 0.25 | 0.03 |
| Neisseria meningitidis | 0.03 | 0.03 | 0.03 |
| Escherichia coli | 0.06 | 0.5 | 0.03 |
| Escherichia coli, ESBL-producing | 0.06 | 0.5 | 0.06 |
| Salmonella spp. | 0.06 | ≤0.5 | 0.03 |
| Shigella spp. | 0.06 | ≤0.5 | 0.03 |
| Klebsiella pneumoniaec | 0.12 | 0.5 | 0.12 |
| Klebsiella oxytoca | 0.06 | 0.5 | 0.12 |
| Enterobacter cloacae | 0.06 | 0.5 | 0.12 |
MIC90 Comparison: Enterobacterales (2) & Non-fermenters
| Organism | Ertapenem | Imipenem | Meropenem |
|---|---|---|---|
| Klebsiella (Enterobacter) aerogenes | 0.06 | 0.5 | 0.12 |
| Morganella morganii | 0.06 | 8 | 0.12 |
| Citrobacter spp. | 0.06 | 0.5 | 0.12 |
| Serratia marcescens | 0.06 | 0.5 | 0.12 |
| Proteus mirabilis | 0.06 | 1 | 0.12 |
| Aeromonas spp. | 0.25 | 0.5 | 0.12 |
| Pseudomonas aeruginosac | >8 | 1 to >8 | 0.5 to >8 |
| Acinetobacter baumanniic | >8 | >8 | >8 |
| Stenotrophomonas maltophilia | >8 | >8 | >8 |
| Burkholderia cepacia | >8 | >8 | 4 |
MIC90 comparison: anaerobes
| Organism | Ertapenem | Imipenem | Meropenem |
|---|---|---|---|
| Peptostreptococcus spp. | 0.125 | 0.25 | 0.125 |
| Fusobacterium spp. | 0.03 | 0.12 | 0.03 |
| Bacteroides fragilis | 0.5 | 0.5 | 0.25 |
| Clostridium perfringens | 0.06 | 0.5 | 0.06 |
| Clostridioides difficile (formerly Clostridium difficile) | 4 | 2 | 2 |
Gram-positive activity
- S. pneumoniae: MIC <0.03 μg/mL (penicillin-susceptible), ~0.5 μg/mL (penicillin-resistant)
- β-Hemolytic streptococci: exquisitely susceptible
- MSSA: MIC <0.5 μg/mL; MRSA: resistant (PBP2a)
- E. faecalis: susceptible to imipenem (MIC ≤2); resistant to ertapenem/meropenem
- E. faecium: resistant to all carbapenems (PBP5)
Gram-negative activity: Enterobacterales
- Most inhibited at MIC ≤1 μg/mL for imipenem/meropenem
- Ertapenem MICs typically ≤0.1 μg/mL (including ESBL-producers)
- Exceptions for imipenem: Morganella, Providencia, Proteus — higher MICs, CLSI has no breakpoints; relebactam does not restore activity
- KPC-producing K. pneumoniae: MIC ≥8 μg/mL → resistant
- KPC-producing E. coli: often lower MICs (0.5–4 μg/mL)
Gram-negative activity: Non-fermenters
- P. aeruginosa: susceptible to imipenem and meropenem but NOT ertapenem
- A. baumannii: variable susceptibility; OXA-type carbapenemases common
- S. maltophilia: intrinsically resistant (chromosomal MBL-L1)
- Burkholderia cepacia: variable
Anaerobic activity
- Ertapenem and meropenem: excellent anaerobic coverage
- Broad activity against Bacteroides fragilis group, Clostridium spp.
- Imipenem: good but may have slightly higher MICs for some Bacteroides
- No carbapenem active against Clostridioides difficile
Other notable activity
- Neisseria gonorrhoeae: highly susceptible; ertapenem activity against ceftriaxone-resistant strains
- N. meningitidis: MIC <0.1 μg/mL
- H. influenzae: susceptible including β-lactamase producers
- Nocardia spp.: imipenem has best activity
- Mycobacteria: imipenem active against some NTM and M. tuberculosis
Individual Agent Profiles
Ertapenem: Key features
- Once-daily dosing (1 g IV q24h) — ideal for OPAT
- Long half-life (~4 hours) due to high protein binding (92%–95%)
- No activity against: P. aeruginosa, Acinetobacter, Enterococcus
- Excellent ESBL-producer coverage
- Preferred for community-acquired polymicrobial infections
Ertapenem: Hypoalbuminemia concern
- 92%–95% protein bound → sensitive to albumin levels
- Hypoalbuminemia → increased free drug → faster renal clearance
- Clinical consequence: subtherapeutic levels despite “adequate” dosing
- Consider alternative carbapenem or TDM in ICU patients with low albumin
Imipenem-cilastatin: Key features
- Must be coadministered with cilastatin (DHP-I inhibitor)
- Most frequent dosing: q6h (less convenient)
- Highest seizure risk among carbapenems
- Unique activity: E. faecalis, Nocardia, mycobacteria
- Decreased infusion stability vs. meropenem
Imipenem: Seizure risk
- Reported rates: 1%–3% general; up to 10% with risk factors
- Risk factors: renal impairment, CNS pathology, high doses
- Mechanism: GABA receptor antagonism
- Dose reduction in renal impairment is critical
- Meropenem preferred when CNS infection or seizure risk exists
Meropenem: Key features
- Most versatile carbapenem for serious infections
- Extended infusion (3 hours) optimizes PK/PD target
- ~2% protein binding → nearly all drug is free
- Half-life ~1 hour with normal renal function
- Good CSF penetration → carbapenem of choice for meningitis
- Can combine total daily dose in 2 bags, infuse each over 12 hours
Meropenem: Extended infusion strategy
- Standard: 1–2 g IV q8h over 30 minutes
- Extended: 1–2 g IV q8h over 3 hours
- Rationale: increases %fT>MIC from ~60% to >90% at standard dose
- Most beneficial for organisms with elevated MICs (4–8 μg/mL)
- Not stable for continuous infusion — use 2 bags over 12h each as alternative
Pharmacokinetics Comparison
PK parameters at a glance
| Parameter | Ertapenem | Imipenem | Meropenem |
|---|---|---|---|
| Protein binding | 92%–95% | ~20% | ~2% |
| Half-life (h) | ~4 | ~1 | ~1 |
| Dosing frequency | q24h | q6–8h | q8h |
| CSF penetration | Poor | Moderate | Good |
| DHP-I stability | Yes | No (needs cilastatin) | Yes |
| Renal elimination | Yes | Yes | Yes |
Renal dose adjustment
- All carbapenems require dose reduction in renal impairment
- Critical for seizure prevention (especially imipenem)
- Ertapenem: no adjustment until CrCl <30 mL/min
- Imipenem: reduce dose AND frequency as CrCl decreases
- Meropenem: extend interval; consider extended infusion maintained
Adverse Effects
Common adverse effects
| Effect | Ertapenem | Imipenem | Meropenem |
|---|---|---|---|
| Diarrhea | ++ | ++ | ++ |
| Nausea/vomiting | + | ++ | ++ |
| Seizure | + | +++ | + |
| Rash | + | ++ | + |
| Transaminase elevation | + | ++ | + |
| Headache | + | + | ++ |
Valproic acid interaction
- Class effect — ALL carbapenems cause precipitous VPA decrease
- Onset: within 24 hours of coadministration
- Mechanism: increased VPA glucuronidation + decreased intestinal absorption
- VPA levels often drop 50%–90%
- Clinical recommendation: avoid concomitant use; use alternative anticonvulsant or alternative antibiotic
β-Lactam cross-allergenicity
- Carbapenems share the β-lactam core with penicillins
- Cross-reactivity rate: approximately 1%
- Carbapenems generally safe in penicillin-allergic patients
- Use caution with history of severe (anaphylactic) penicillin allergy
- Aztreonam: no cross-reactivity with penicillins/carbapenems
- Exception: shares side chain with ceftazidime
Clinical Applications
Treatment algorithm: Carbapenem selection
- Empiric/broad-spectrum: Meropenem (extended infusion)
- Step-down/OPAT: Ertapenem
- Mixed GN + E. faecalis: Imipenem
- KPC-producing CRE: Meropenem-vaborbactam
- DTR P. aeruginosa: Imipenem-relebactam
- MBL producers: Aztreonam + ceftazidime-avibactam
- Severe β-lactam allergy + GN coverage: Aztreonam
ESBL-producing enterobacterales
- Carbapenems remain agents of choice for serious ESBL infections
- MERINO trial: meropenem superior to piperacillin-tazobactam for ESBL bacteremia
- Ertapenem suitable for step-down therapy and less severe infections
- Once-daily dosing facilitates OPAT transition
KPC-producing CRE: Preferred agents
- First-line: Meropenem-vaborbactam (IDSA 2023 guidance)
- Alternative: Ceftazidime-avibactam
- Vaborbactam designed specifically for KPC binding
- Early clinical data: improved outcomes vs. best available therapy
- Imipenem-relebactam: less clinical data for KPC infections
Difficult-to-Treat P. aeruginosa
- DTR-PA: resistant to all traditional first-line agents
- Imipenem-relebactam: key agent (relebactam inhibits AmpC → restores imipenem activity)
- AmpC overproduction is a major driver of imipenem resistance in P. aeruginosa
- Alternative: ceftolozane-tazobactam, ceftazidime-avibactam
- For MBL-producing P. aeruginosa: cefiderocol
MBL-producing organisms
- No available BLI inhibits MBLs
- Aztreonam: stable to MBL hydrolysis
- Aztreonam + ceftazidime-avibactam: synergistic combination
- Avibactam protects aztreonam from serine β-lactamases
- Aztreonam resists MBL hydrolysis
- Cefiderocol: alternative for MBL-producers
Aztreonam
Aztreonam: Unique monobactam
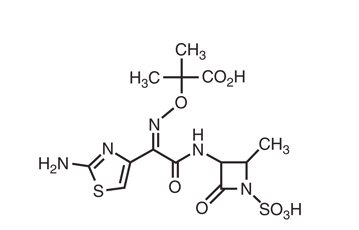
- Only clinically available monobactam
- Monocyclic β-lactam ring (not bicyclic like other β-lactams)
- Minimal cross-allergenicity with penicillins/cephalosporins/carbapenems
- Spectrum: aerobic gram-negatives ONLY
- No activity against gram-positives or anaerobes
Aztreonam: Dosing and PK
- Adult dose: 2 g IV q8h (consider extended infusion over 3 hours)
- Pediatric dose: 30 mg/kg IV q6–8h (max 120 mg/kg/day)
- Higher doses for cystic fibrosis patients
- Adverse effects: rash, diarrhea, transaminase elevation, neutropenia, phlebitis
Aztreonam: Clinical niche
Two primary roles:
- Severe β-lactam allergy → safe alternative for gram-negative coverage
- Exception: shares side chain with ceftazidime (cross-reactivity possible)
- MBL-producing infections → combined with ceftazidime-avibactam
- Stable to MBL hydrolysis
- Avibactam covers co-produced serine β-lactamases
Aztreonam side chain similarity
- Similar R1 side chain to ceftazidime and cefiderocol
- This side chain provides activity vs P. aeruginosa
- Cross-allergenicity possible with ceftazidime (but not other cephalosporins)
- Stability to MBLs is due to the monobactam ring, not the side chain
Putting it all together
Summary: Choosing the right carbapenem
| Clinical Scenario | Preferred Agent |
|---|---|
| ESBL bacteremia | Meropenem |
| ESBL step-down/OPAT | Ertapenem |
| Mixed GN + E. faecalis | Imipenem |
| KPC-producing CRE | Meropenem-vaborbactam |
| DTR P. aeruginosa | Imipenem-relebactam |
| MBL-producing CRE | Aztreonam + CAZ-AVI |
| Severe β-lactam allergy | Aztreonam |
| Meningitis | Meropenem |
| Nocardiosis | Imipenem |
Dosing summary
Key takeaways
- Carbapenems are time-dependent killers — optimize fT>MIC with extended infusions
- Ertapenem has a narrow niche (no Pseudomonas, no Acinetobacter, no Enterococcus)
- Know the resistance mechanism to choose the right agent
- KPC → meropenem-vaborbactam; DTR-PA → imipenem-relebactam; MBL → aztreonam + CAZ-AVI
- Avoid carbapenems with VPA — class-wide interaction
- Aztreonam is uniquely safe in β-lactam allergy and uniquely active against MBL-producers
Class-wide reminders
- ALL carbapenems: reduce dose in renal impairment
- ALL carbapenems: precipitous decrease in VPA levels
- ALL carbapenems: time-dependent kill → optimize infusion duration
- ALL carbapenems: no activity vs MRSA or VRE
- ALL carbapenems (except ertapenem): Pseudomonas activity
- Neither BLI: covers MBLs or OXA-48
References
Abdul-Aziz, Mohd H., Hasan Sulaiman, Mohd-Basri Mat-Nor, Vineya Rai, Pui-Yin Wong, Mohd S. Hasan, Abdul Nasir Abd Rahman, et al. 2020. “Continuous \(\beta\)-Lactam Infusion in Critically Ill Patients: The Clinical Evidence.” Intensive Care Medicine 46: 1086–88.
Bush, Karen, and Patricia A. Bradford. 2020. “Interplay Between \(\beta\)-Lactamases and New \(\beta\)-Lactamase Inhibitors.” Clinical Microbiology Reviews 32 (2): e00159–18.
Cercenado, Emilia, Mercedes Marín, Patricia Muñoz, Rosario Insa, Maria Esther Cruz, and Emilio Bouza. 2007. “In Vitro Activities of Tigecycline and Eight Other Antimicrobials Against Various Nocardia Species Identified by Molecular Methods.” Antimicrobial Agents and Chemotherapy 51 (3): 1102–4.
Clinical and Laboratory Standards Institute. 2011. “Performance Standards for Antimicrobial Susceptibility Testing: Twenty-First Informational Supplement (M100-S21).” Wayne, PA: Clinical; Laboratory Standards Institute.
Davies, Timothy A., Anne Marie Queenan, Brian J. Morrow, Wenliang Shang, Kent Amsler, Wenping He, Annette S. Lynch, Christopher Pillar, and Robert K. Flamm. 2011. “Longitudinal Survey of Carbapenem Resistance and Resistance Mechanisms in Enterobacteriaceae and Non-Fermenters from the USA in 2007–08.” Journal of Antimicrobial Chemotherapy 66 (10): 2298–2307.
Drusano, George L. 1986. “An Overview of the Pharmacology of Imipenem/Cilastatin.” Journal of Antimicrobial Chemotherapy 18 (Suppl E): 79–92.
Fabrizio, Claudia, Felice Valzano, Simone Giuliano, Elisabetta Morelli, Daniela Serio, Giovanni Battista Buccoliero, Maurizio Cervellera, et al. 2026. “Optimizing Target Inactivation to Treat Multidrug-Resistant Escherichia Coli with NDM and PBP3 Mutations: ‘Going the Extra Mile’.” Antimicrobial Agents and Chemotherapy 70 (5): e00887–25. https://doi.org/10.1128/aac.00887-25.
Fritsche, Thomas R., Marjorie G. Stilwell, and Ronald N. Jones. 2009. “Antimicrobial Activity of Doripenem Tested Against Resistant Phenotype Haemophilus Influenzae and Moraxella Catarrhalis.” Diagnostic Microbiology and Infectious Disease 63 (2): 216–20.
Frumin, Jonathan, and Jason C. Gallagher. 2009. “Allergic Cross-Sensitivity Between Penicillin, Carbapenem, and Monobactam Antibiotics: What Are the Chances?” Annals of Pharmacotherapy 43 (2): 304–15.
Fuda, Chris C. S., Jed F. Fisher, and Shahriar Mobashery. 2005. “\(\beta\)-Lactam Resistance in Staphylococcus Aureus: The Adaptive Resistance of a Plastic Genome.” Cellular and Molecular Life Sciences 62 (22): 2617–33.
Goldstein, Ellie J. C., Diane M. Citron, C. Vreni Merriam, Yumi A. Warren, Karen L. Tyrrell, and Helen T. Fernandez. 2000. “Comparative in Vitro Activities of Ertapenem (MK-0826) Against 1,001 Anaerobes Isolated from Human Intra-Abdominal Infections.” Antimicrobial Agents and Chemotherapy 44 (9): 2389–94.
Griffith, David C., John S. Loutit, Elizabeth E. Morgan, Stephanie Durso, and Michael N. Dudley. 2017. “Phase 1 Study of the Pharmacokinetics and Safety of the \(\beta\)-Lactamase Inhibitor Vaborbactam (RPX7009) in Subjects with Various Degrees of Renal Impairment.” Antimicrobial Agents and Chemotherapy 61 (9): e00741–17.
Harris, Patrick N. A., Paul A. Tambyah, David C. Lye, Yin Mo, Tau Hong Lee, Meseret Yilmaz, Talal H. Alenazi, et al. 2018. “Effect of Piperacillin-Tazobactam Vs Meropenem on 30-Day Mortality for Patients with E coli or Klebsiella Pneumoniae Bloodstream Infection and Ceftriaxone Resistance: A Randomized Clinical Trial.” JAMA 320 (10): 984–94.
Jones, Ronald N., Helio S. Sader, and Thomas R. Fritsche. 2009. “Comparative Activity of Doripenem and Three Other Carbapenems Tested Against Gram-negative Bacilli with Various \(\beta\)-Lactamase Resistance Mechanisms.” Diagnostic Microbiology and Infectious Disease 63 (4): 440–44.
Kohler, Thilo, Mehrnaz Michéa-Hamzehpour, Sebastien F. Epp, and Jean-Claude Pechère. 1999. “Carbapenem Activities Against Pseudomonas Aeruginosa: Respective Contributions of OprD and efflux Systems.” Antimicrobial Agents and Chemotherapy 43 (2): 424–27.
Ma, Jun, Linghui Zhu, Qingxing Ou, Wei Yu, Cen Huang, Huan Xu, Juan Du, and Feng Zhao. 2022. “Aztreonam-Avibactam Versus Aztreonam Plus Ceftazidime-Avibactam for the Treatment of Infections Caused by Metallo-\(\beta\)-Lactamase-Producing Gram-Negative Bacteria.” International Journal of Antimicrobial Agents 60 (5–6): 106660.
Majumdar, Anita K., David G. Musson, Karen L. Birk, Carolyn J. Kitchen, Scott Holland, Janet McCrea, Govinda Mistry, et al. 2002. “Pharmacokinetics of Ertapenem in Healthy Young Volunteers.” Antimicrobial Agents and Chemotherapy 46 (11): 3506–11.
Masuda, Nobuhisa, Etsuko Sakagawa, Shizuko Ohya, Naomasa Gotoh, Hiroshi Tsujimoto, and Taiji Nishino. 2000. “Substrate Specificities of MexAB-OprM, MexCD-OprJ, and MexXY-OprM Efflux Pumps in Pseudomonas Aeruginosa.” Antimicrobial Agents and Chemotherapy 44 (12): 3322–27.
Mavridou, Eleftheria, Christian G. Giske, Lena E. Friberg, Daniel J. Diekema, and S. Leverett. 2015. “Pharmacodynamics of MK-7655, a Novel \(\beta\)-Lactamase Inhibitor, Combined with Imipenem in a Hollow Fibre Infection Model Against Pseudomonas Aeruginosa.” Antimicrobial Agents and Chemotherapy 59 (2): 1314–22.
Miller, Abby D., Arthur M. Ball, P. Brandon Bookstaver, Brian Dooha, Samir P. Bhatt, Sujata M. Bhavnani, Theodore R. Pasquale, and Jesus Morales-Ramirez. 2011. “Epileptogenic Potential of Carbapenem Agents: Mechanism of Action, Seizure Rates, and Clinical Considerations.” Pharmacotherapy 31 (4): 408–23.
Mori, Hiroshi, Keiko Takahashi, and Takaharu Mizutani. 2007. “Interaction Between Valproic Acid and Carbapenem Antibiotics.” Drug Metabolism Reviews 39 (4): 647–57.
Nicolau, David P. 2008. “Pharmacodynamic Optimization of \(\beta\)-Lactams in the Patient Care Setting.” Critical Care 12 (Suppl 4): S2.
Nordmann, Patrice, Thierry Naas, and Laurent Poirel. 2011. “Global Spread of Carbapenemase-Producing Enterobacteriaceae.” Emerging Infectious Diseases 17 (10): 1791–98.
Norrby, S. R. 1997. “Meropenem in the Treatment of Serious Infections: A Review of Studies.” Clinical Infectious Diseases 24 (Suppl 2): S247–53.
Reyes, Jesús, Ana Catalina Aguilar, Christian Capataz, Camilo Moya, Christian J. Pallares, Cristhian Hernandez-Gómez, Jorge Osorio, et al. 2023. “Molecular Epidemiology and Clinical Outcomes of Carbapenem-Resistant Pseudomonas Aeruginosa Infections: A Prospective Cohort Study.” The Lancet Microbe 4 (8): e579–88.
Shields, Ryan K., Erin K. McCreary, Rachel V. Marini, Crystal B. Moser, Arvind Bhimaraj, Jennifer S. Esterly, Cornelius J. Clancy, and M. Hong Nguyen. 2020. “Early Experience with Meropenem-Vaborbactam for Treatment of Carbapenem-Resistant Enterobacteriaceae Infections.” Clinical Infectious Diseases 71 (3): 667–71.
Stellfox, Madison E., and Yohei Doi. 2026. “Case Commentary: When One Target Is Not EnoughPBP3 Insertions and Target Redundancy in Escherichia Coli.” Antimicrobial Agents and Chemotherapy 70 (5): e00053–26. https://doi.org/10.1128/aac.00053-26.
Tamma, Pranita D., Samuel L. Aitken, Robert A. Bonomo, Amy J. Mathers, David van Duin, and Cornelius J. Clancy. 2023. “Infectious Diseases Society of America Guidance on the Treatment of AmpC \(\beta\)-Lactamase-Producing Enterobacterales, Carbapenem-Resistant Acinetobacter baumannii, and Stenotrophomonas Maltophilia Infections.” Clinical Infectious Diseases 74 (12): 2089–2114.
Trias, J., and H. Nikaido. 1990. “Protein D2 Channel of the Pseudomonas Aeruginosa Outer Membrane Has a Binding Site for Basic Amino Acids and Peptides.” Journal of Biological Chemistry 265 (26): 15680–84.
Unemo, Magnus, and Robert A. Nicholas. 2012. “Emergence of Multidrug-Resistant, Extensively Drug-Resistant and Untreatable Gonorrhea.” Future Microbiology 7 (12): 1401–22.
Weiner-Lastinger, Lindsey M., Sandra Abner, Jonathan R. Edwards, Alexander J. Kallen, Maria Karlsson, Shelley S. Magill, Daniel Pollock, et al. 2020. “Antimicrobial-Resistant Pathogens Associated with Adult Healthcare-Associated Infections: Summary of Data Reported to the National Healthcare Safety Network, 2015–2017.” Infection Control & Hospital Epidemiology 41 (1): 1–18.
Yigit, Hesna, Anne Marie Queenan, Gregory J. Anderson, Antonio Domenech-Sanchez, James W. Biddle, Carey D. Steward, Sebastian Alberti, Karen Bush, and Fred C. Tenover. 2001. “Novel Carbapenem-Hydrolyzing \(\beta\)-Lactamase, KPC-1, from a Carbapenem-Resistant Strain of Klebsiella Pneumoniae.” Antimicrobial Agents and Chemotherapy 45 (4): 1151–61.
Zhanel, George G, Courtney K Lawrence, Heather Adam, Frank Schweizer, Sheryl Zelenitsky, Michael Zhanel, Philippe R S Lagacé-Wiens, et al. 2018. “Imipenem-Relebactam and Meropenem-Vaborbactam: Two Novel Carbapenem-β-Lactamase Inhibitor Combinations.” Drugs 78 (1): 6598. https://doi.org/10.1007/s40265-017-0851-9.
Zusman, Oren, Liron Farbman, Zeev Tredler, Vered Daitch, Amir Lador, Leonard Leibovici, and Mical Paul. 2015. “Association Between Hypoalbuminaemia and Mortality Amongst Patients Treated with Ertapenem Versus Other Carbapenems: Prospective Study and Meta-Analysis.” Clinical Microbiology and Infection 21 (1): 54–58.