Principles of Antibiotic Therapy
Prof. Russell Lewis
Department of Molecular Medicine
University of Padua
russelledward.lewis@unipd.it
https://github.com/Russlewisbo
slides available at: www.padovaid.com
 |
Antibiotics- The Medical Miracle
Medicine in the pre-antibiotic era
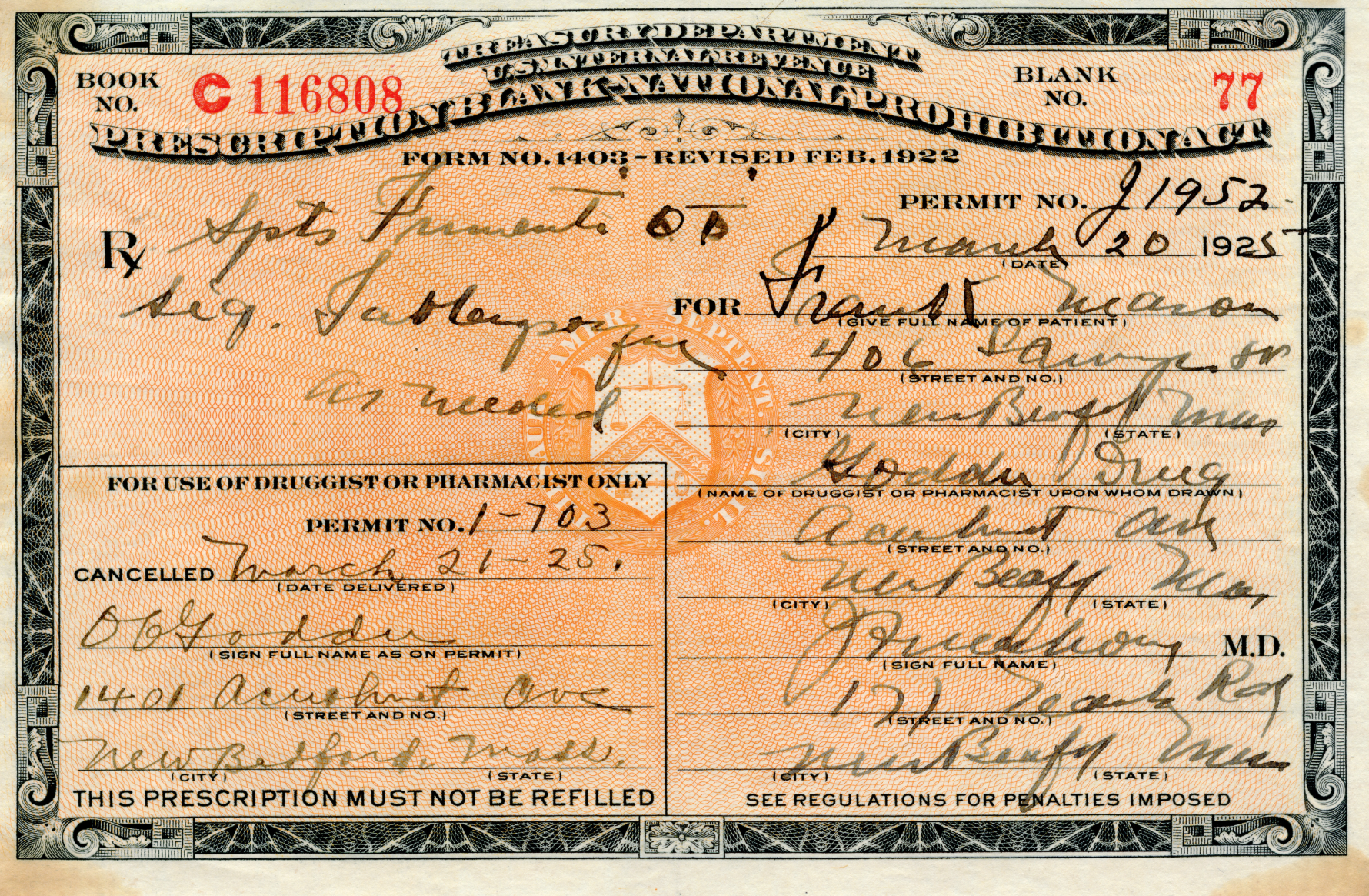
A copy of a doctor’s prescription issued to a patient in Massachusetts in 1925. The doctor here wrote in a common Latin term, “Spts frumenti” or spiritus frumenti -i.e. whiskey

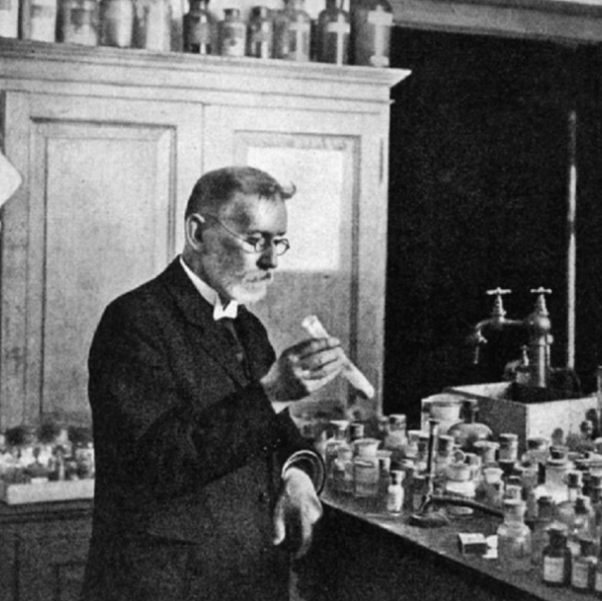
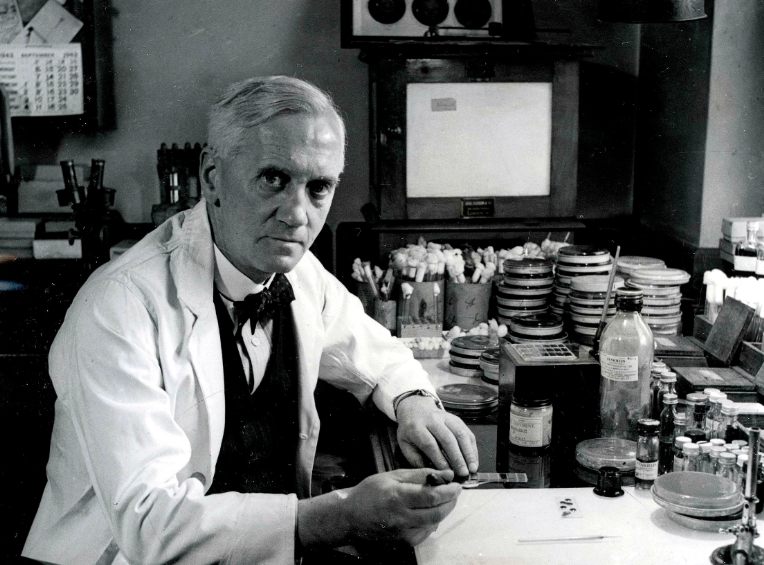
Dawn of antibiotic discovery
| Paul Ehrlich Salvarsan 1909 |
Alexander Fleming Purified and tested by Florey, Chain, Heatley-1940 |
Gerhard Domagk, Sulfanilamides 1931 |
|---|---|---|
 |
 |
 |
World Health Organization (WHO)
Pathogen Priority List
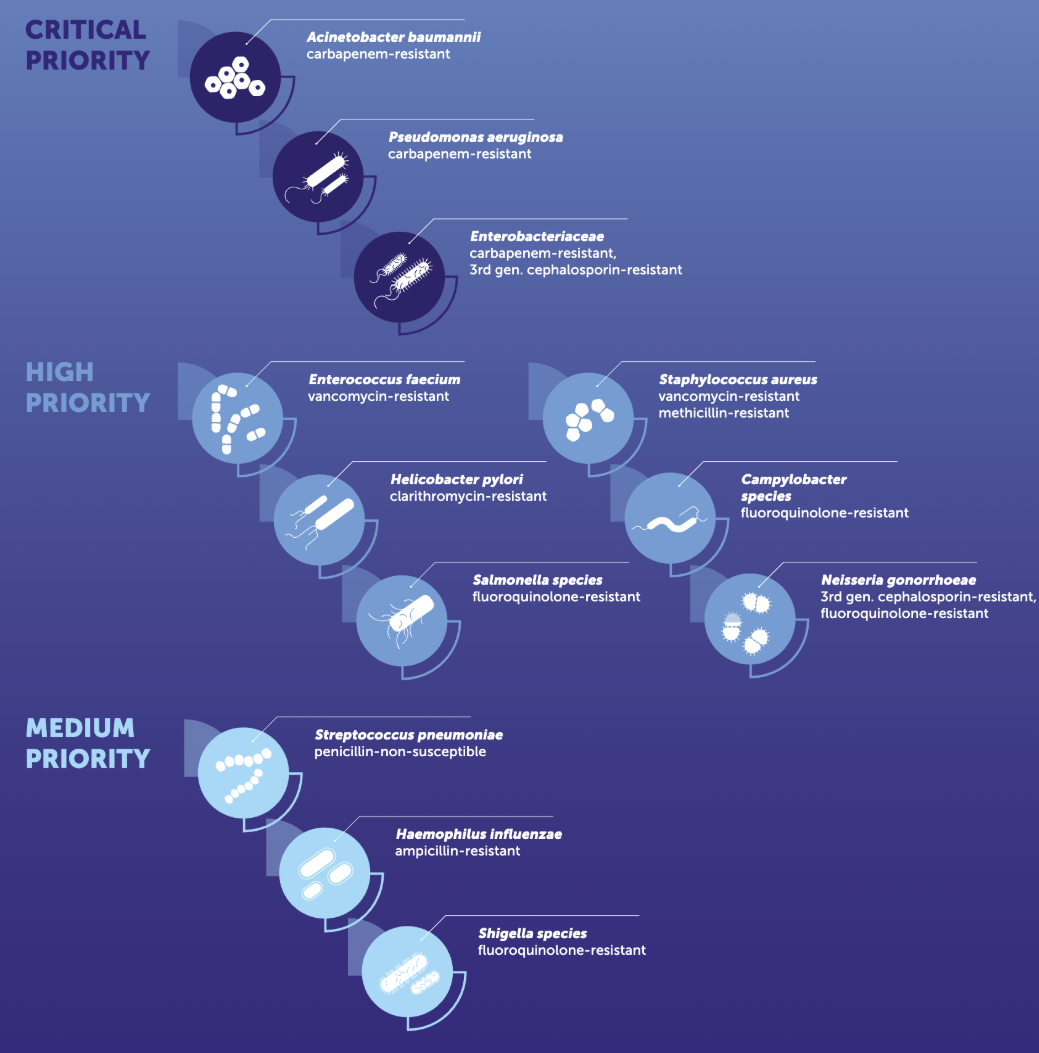
Methicillin-resistant
Staphylococcus aureus (MRSA)
Carbapenem-resistant Enterobacterales (CRE)
Multi-drug resistant (MDR)
Acinetobacter baumannii
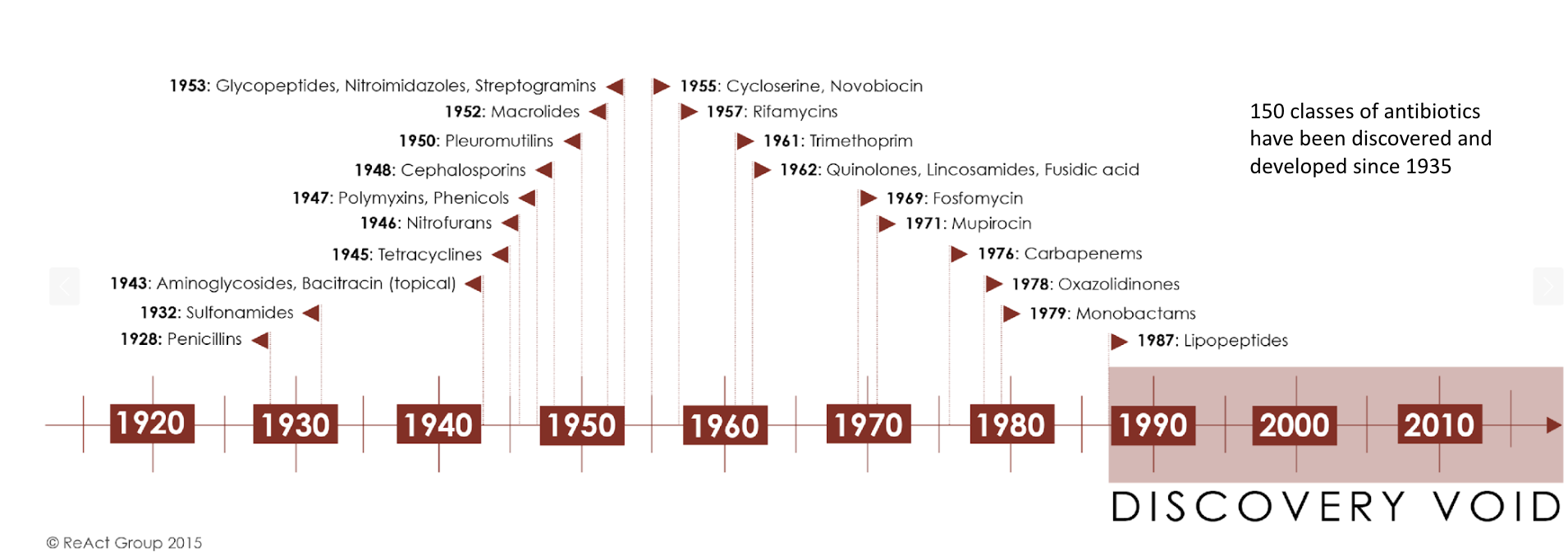
Antibiotic discovery is slowing
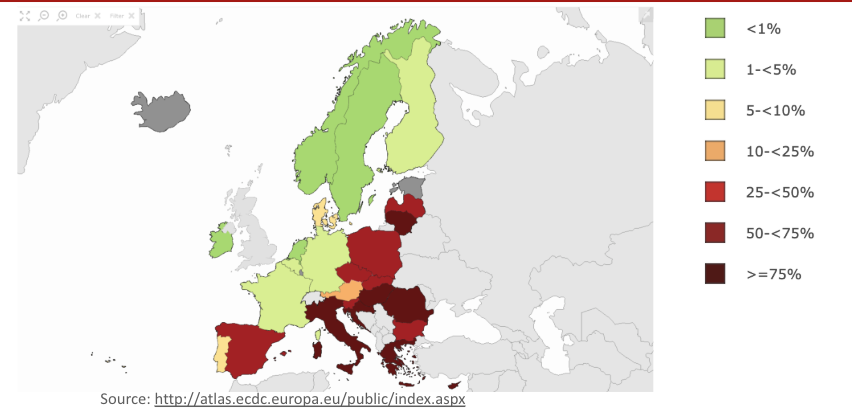
Antibiotic stewardship
 |
 |
Case Example
Chief complaint: 34 year-old farmer from Sicily presents with worsening back pain after sitting for more than couple of hours
No other significant past medical history
Spondylitis etiologies:
> 50% Staphylococcus aureus, Staphylococcus epidermidis
~ 25% Streptococcus spp., Enterococcus spp. Pseudomonas aeruginosa, Enterobacter spp., Proteus spp. E. coli, Serratia spp., Anaerobes, Mycobacterium tuberculosis (Pott’s disease)

Could this be brucellosis?
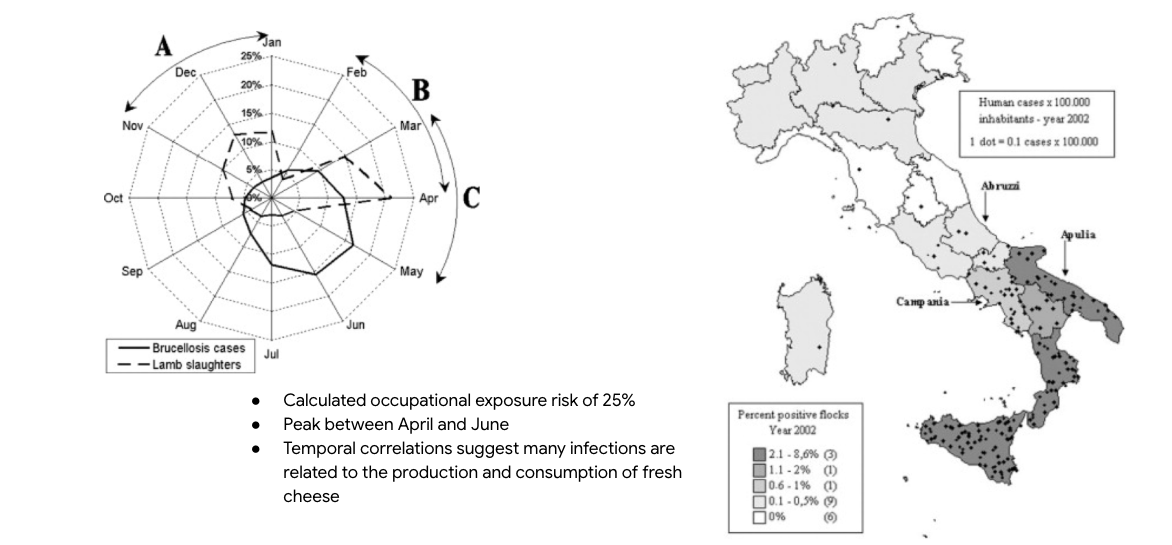 Zoonotic Gram-negative coccobacilli
Zoonotic Gram-negative coccobacilli
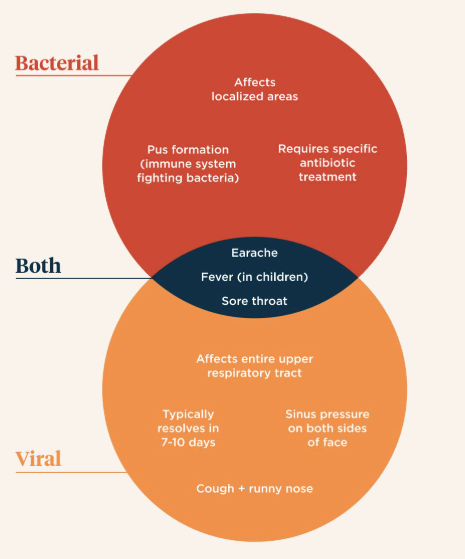
Antibiotics are usually started empirically
Antibiotics should only be started if the differential diagnosis includes likely invasive bacterial infections:
>90% of upper respiratory tract infections are caused by viruses
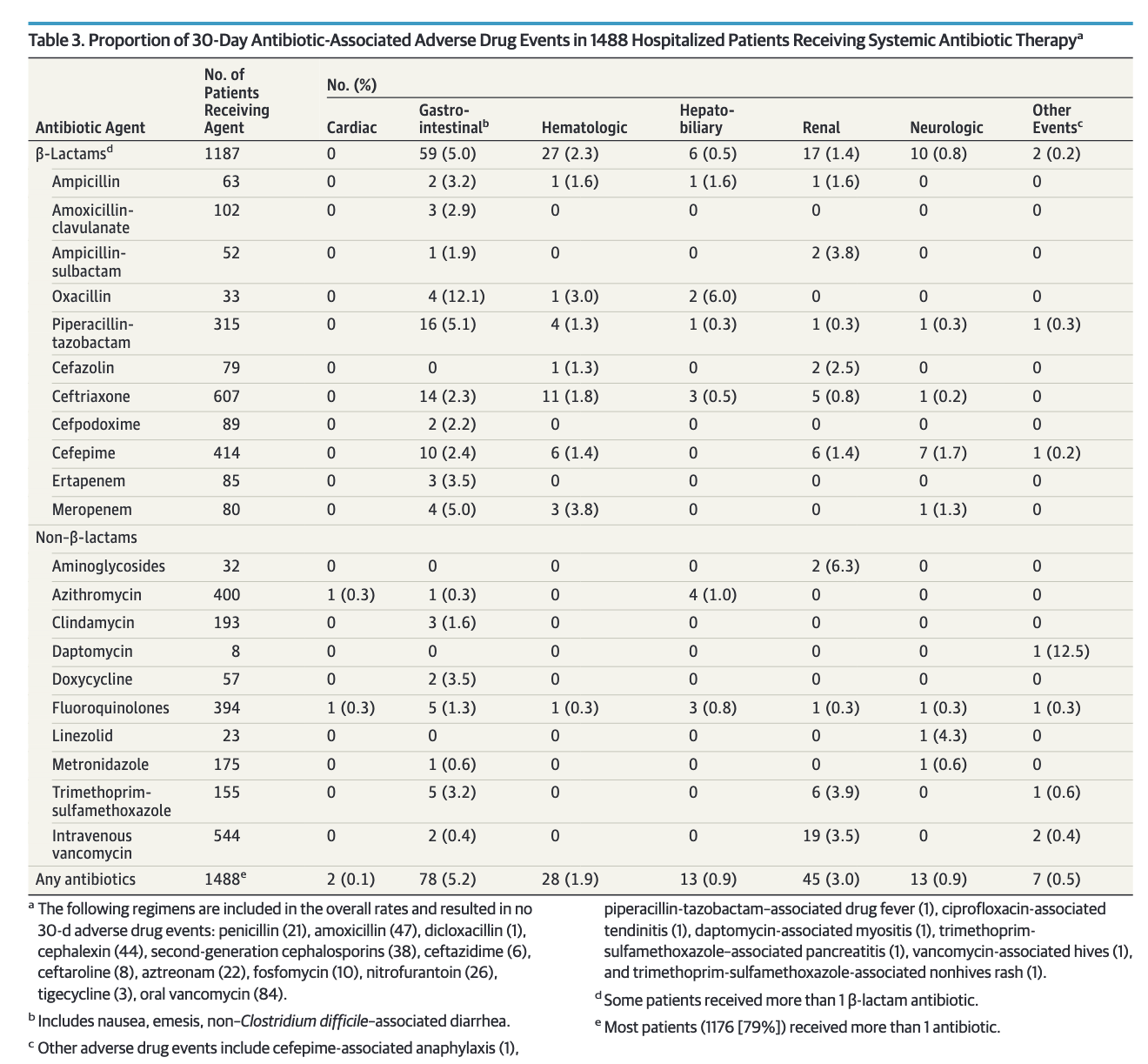
Association of adverse events with antibiotic use in hospitalized patients
Positive cultures
are not always proof of infection
A positive culture in the absence of signs or symptoms of infection should not reflexively trigger antibiotic therapy
Without symptoms, a positive culture often represents colonization or contamination
| Wound swabs | Urine cultures | Bronchial alveolar lavage | Respiratory samples | GI tract/stool |
|---|---|---|---|---|
 |
 |
 |
 |
 |
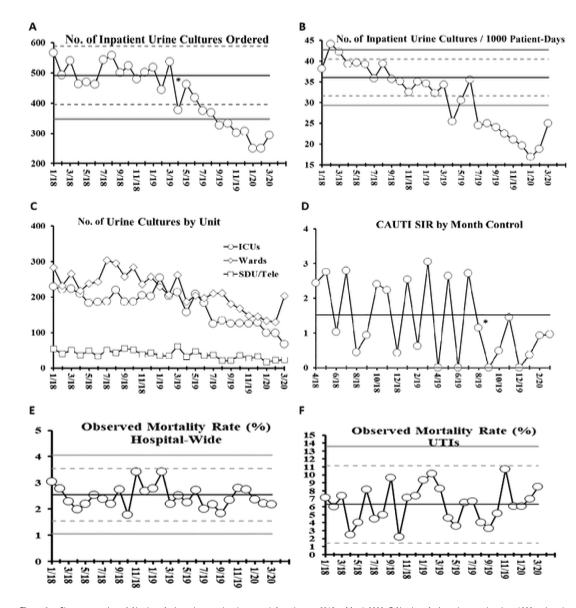
Simple stewardship interventions
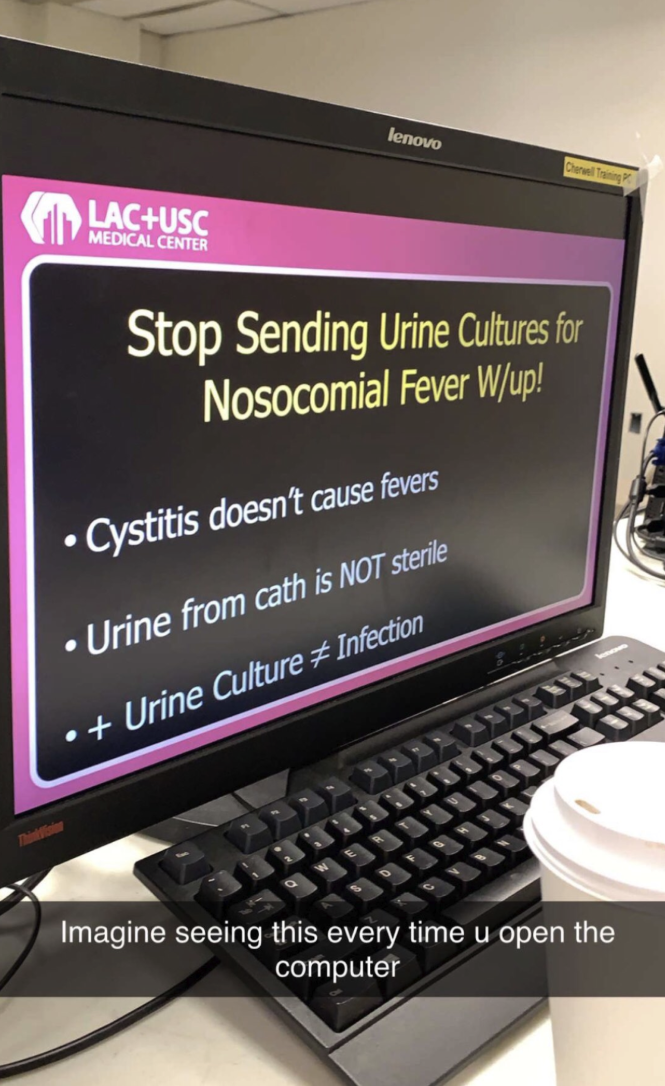
Simple stewardship intervention
Antibiotics are not the only answer
The administration of antibiotics should not be a reflexive response to infection, but should be incorporated into an overall, rational therapeutic plan for the patient.
Patients who lack bacterial infections cannot have their clinical course improved by antibiotics (as discussed in Principle #1).

Classic example: osteomyelitis with persistently exposed bone
Ethical dilemmas for use of
antimicrobial therapy
| End of life (comfort care) | Non-adherent HIV therapy |
|---|---|
 |
 |
Know the spectrum of activity
|
|
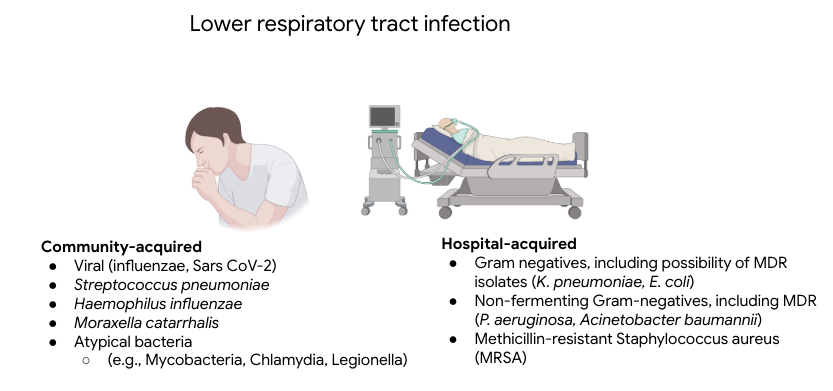
Community-acquired vs. nosocomial
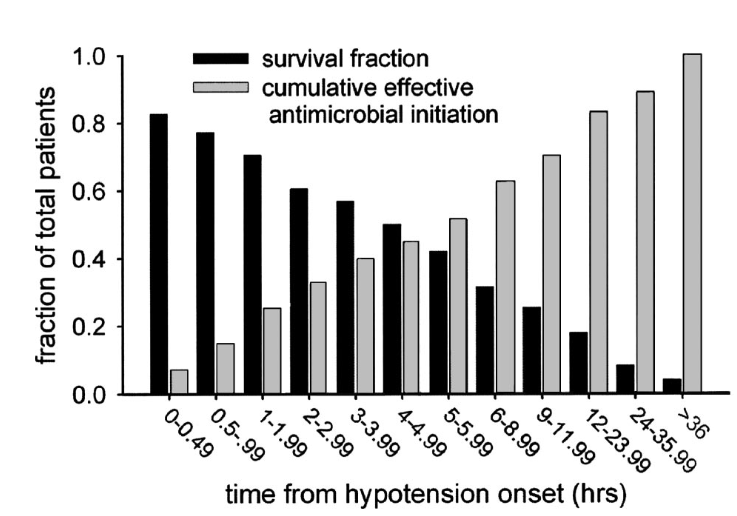
Principle #4: There is a lower threshold for empirical therapy in critically-ill patients

Antibiotic timing is critical in septic shock
Principle #5: Host factors affect the spectrum of empirical therapy
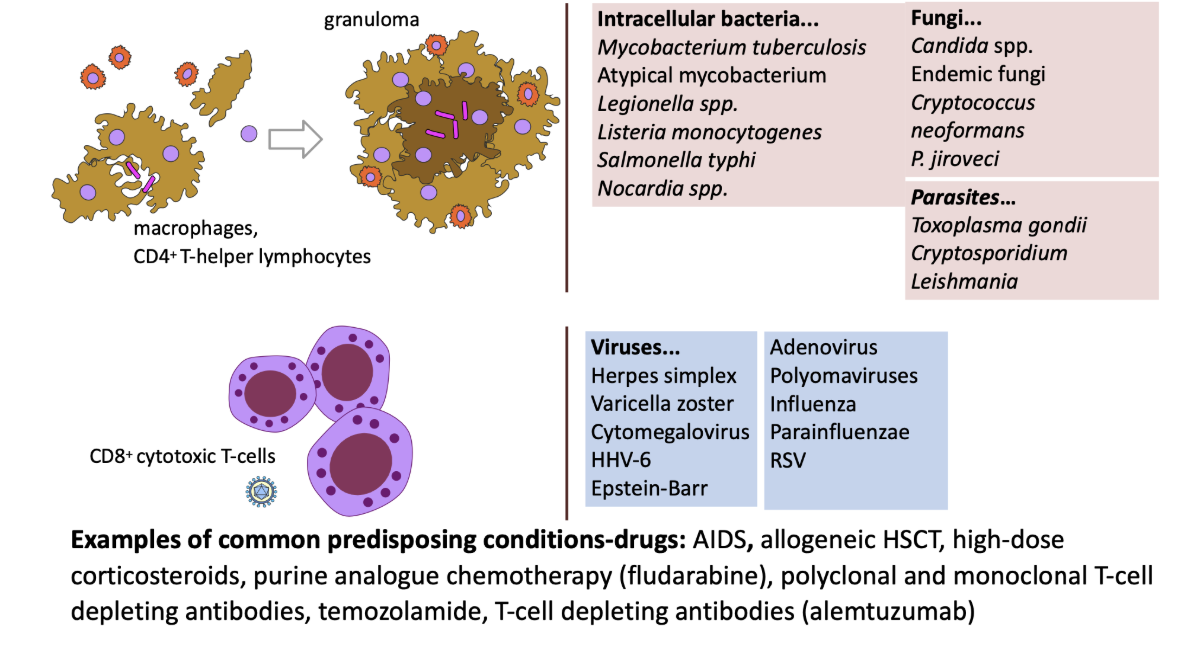
Common immunocompromised conditions
 |
|
Glucocorticoids:
“Credit cards” of immunosuppressive therapy
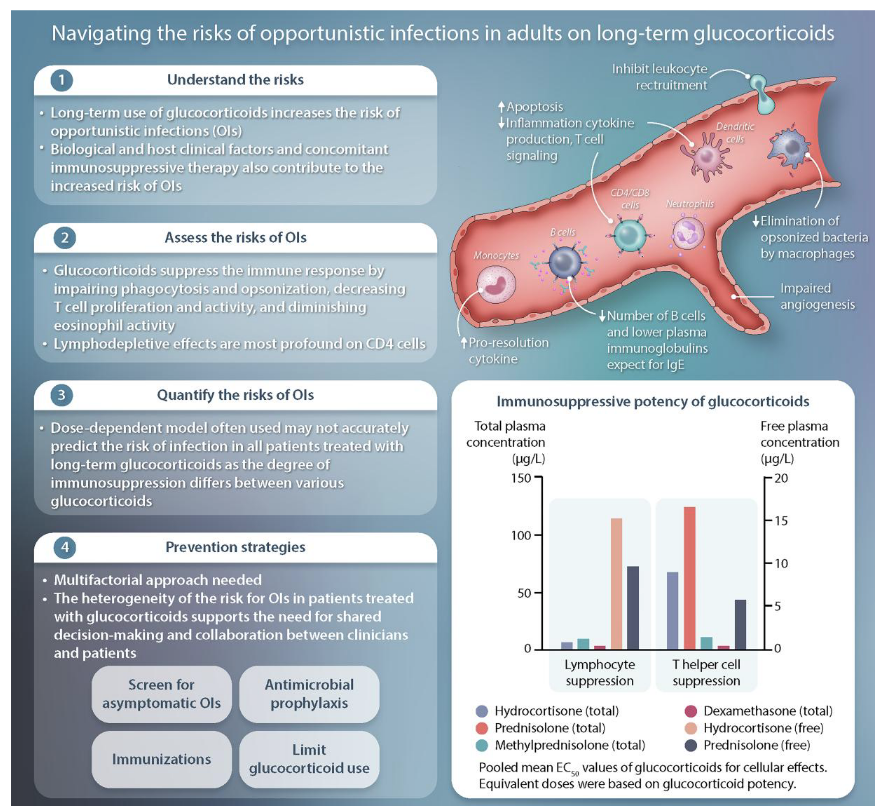
Dose-dependent increase in the risk of opportunistic infections > 10 mg of prednisone equivalents (PEQ) per day for 2-4 weeks
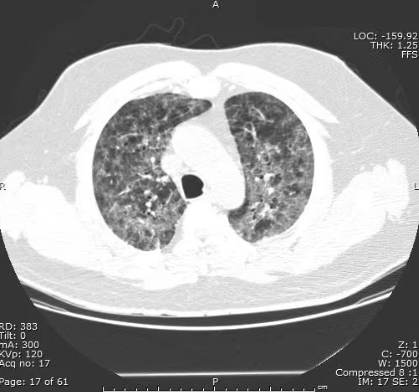
Community acquired pneumonia (CAP)
vs. Pneumocystis jirovecii pneumonia (PCP)
Diffuse bilateral infiltrates |
Patchy areas of ground-glass attenuation |

Key pharmacokinetic variables
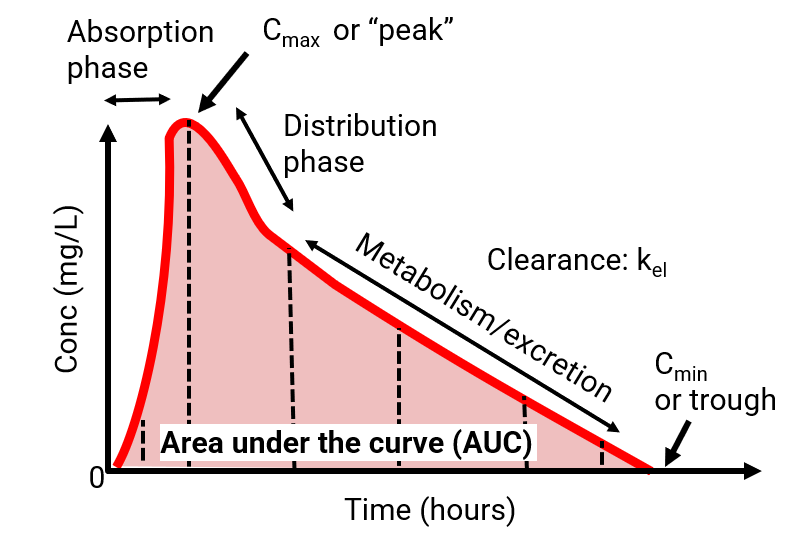
Key pharmacokinetic variable:
Volume of distribution (Vd)
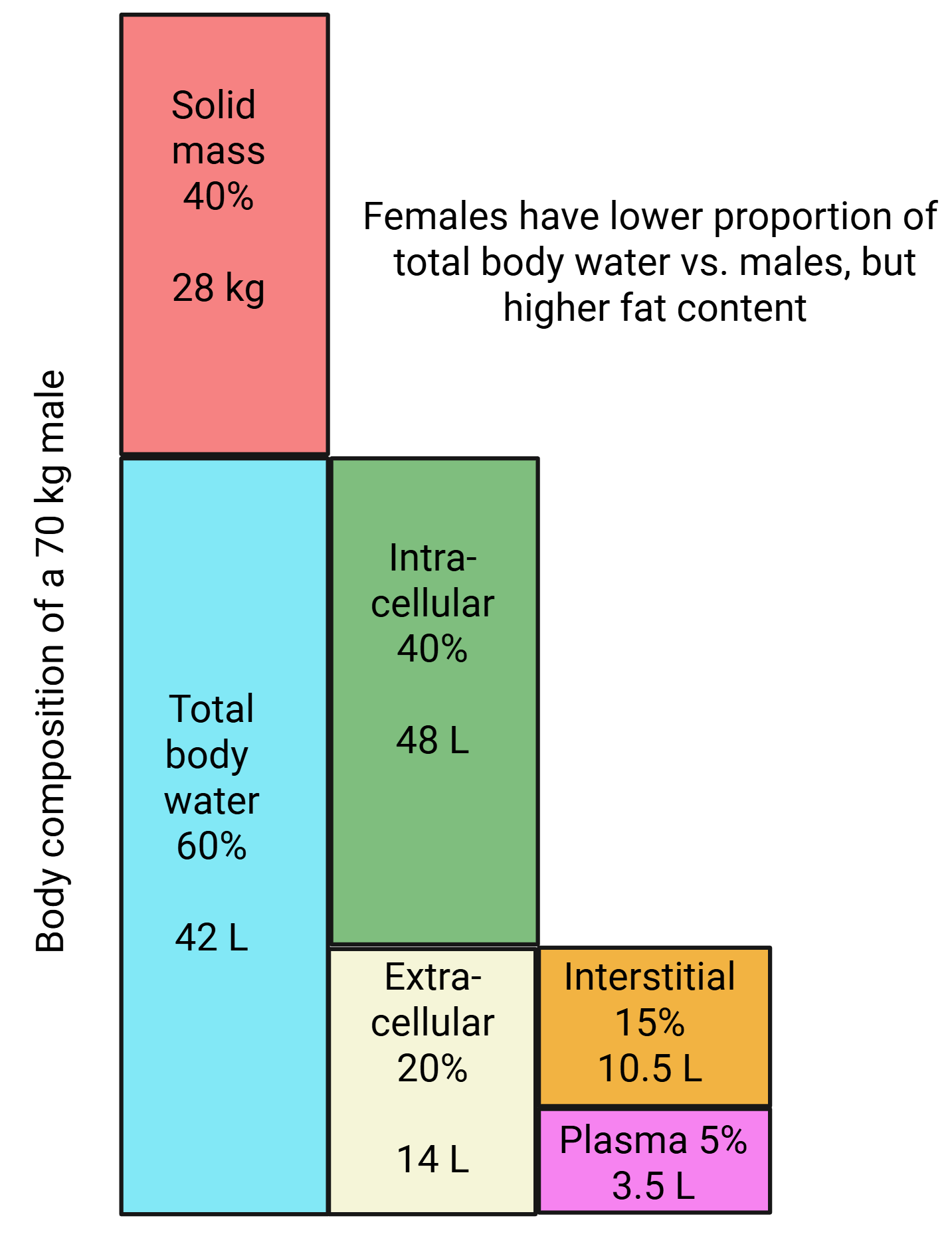
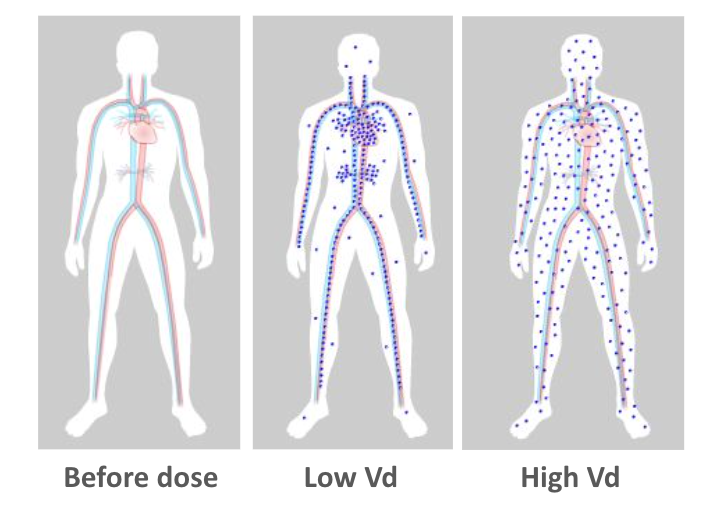
Volume of distribution
Plasma volume= 3L+ Extracellular water 16 L = Total body water (~20L)
Higher Vd (e.g., > 46 L Vd)= sequestered in depot (e.g., fat) and serum concentrations will be lower
Volume of distribution (Vd):
relevance for antibiotic selection
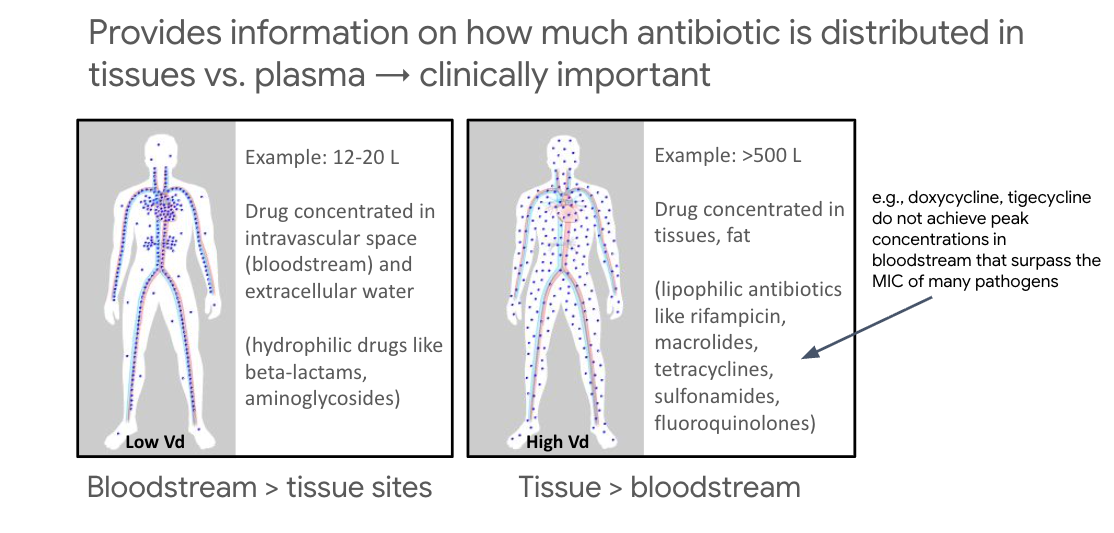
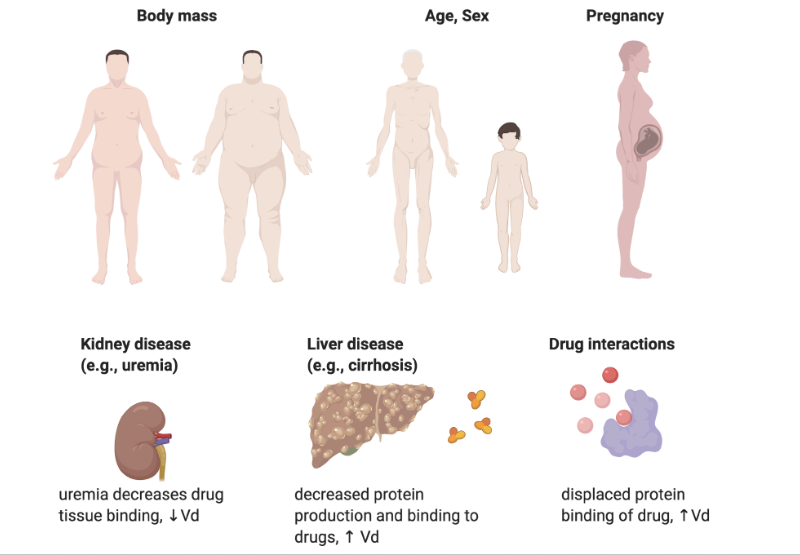
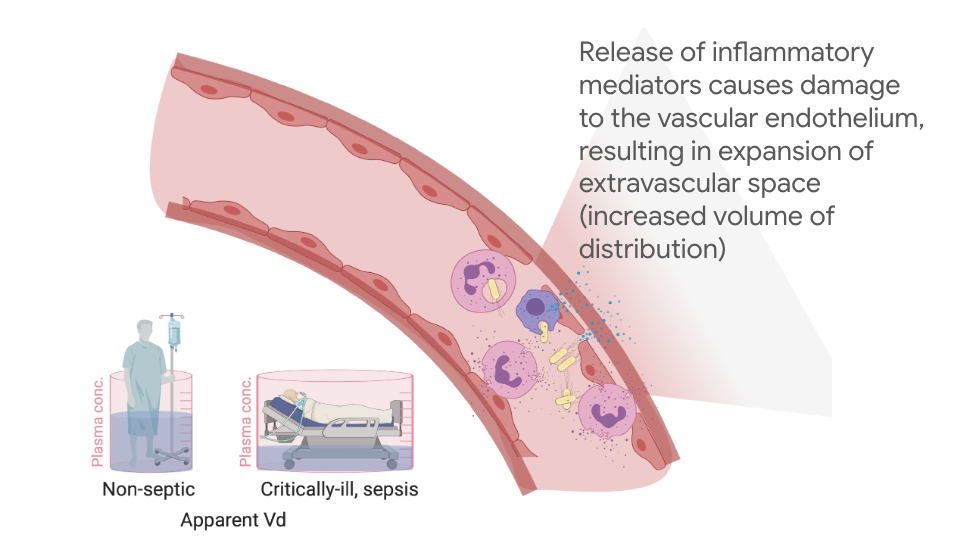
Vd alterations
Vd changes in critical illness
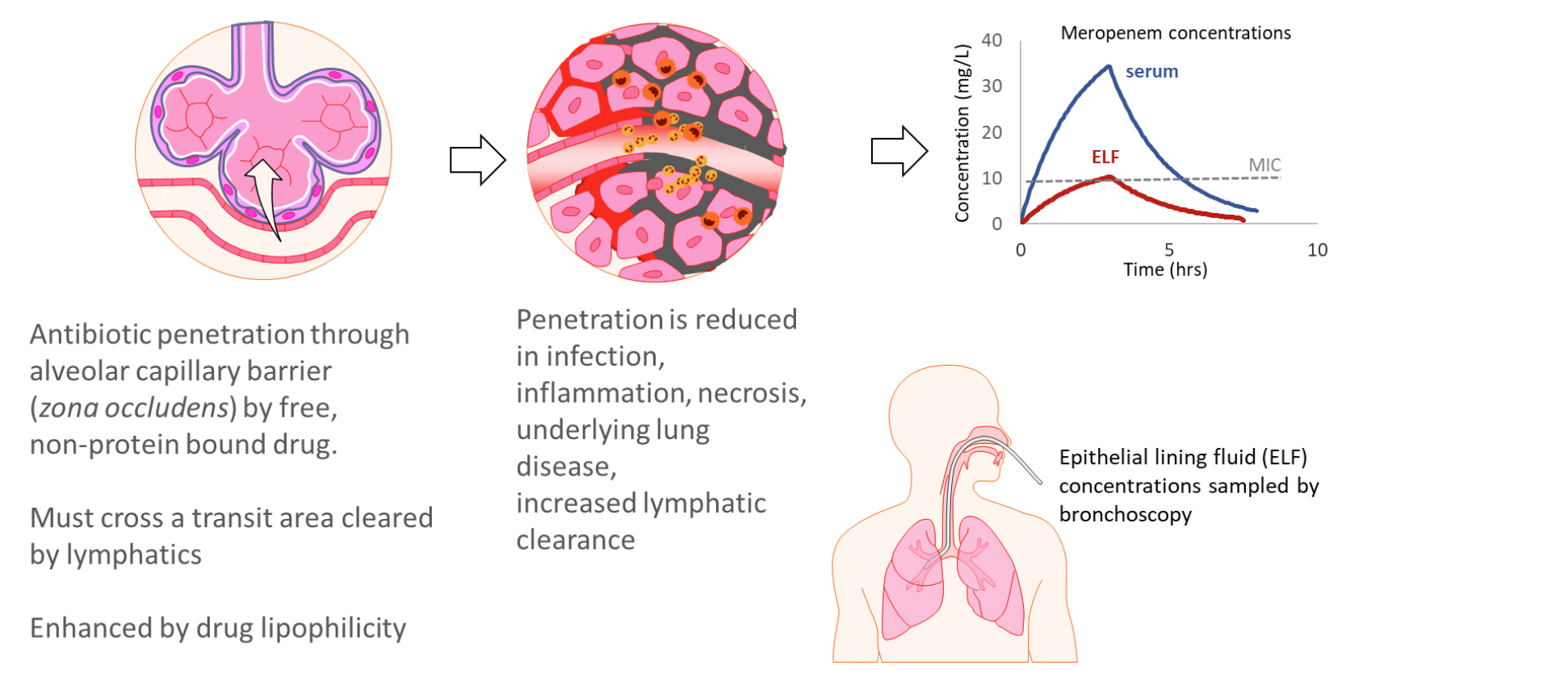
Drug penetration in ventilator-associated pneumonia
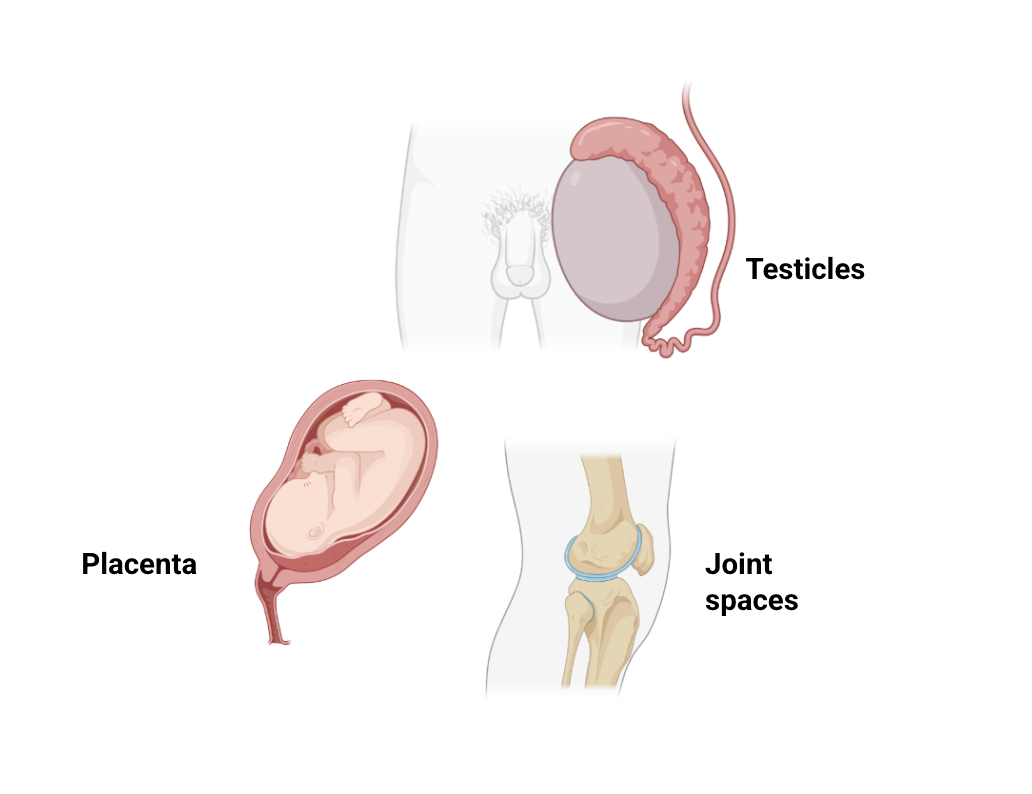
Anatomically-privileged sites
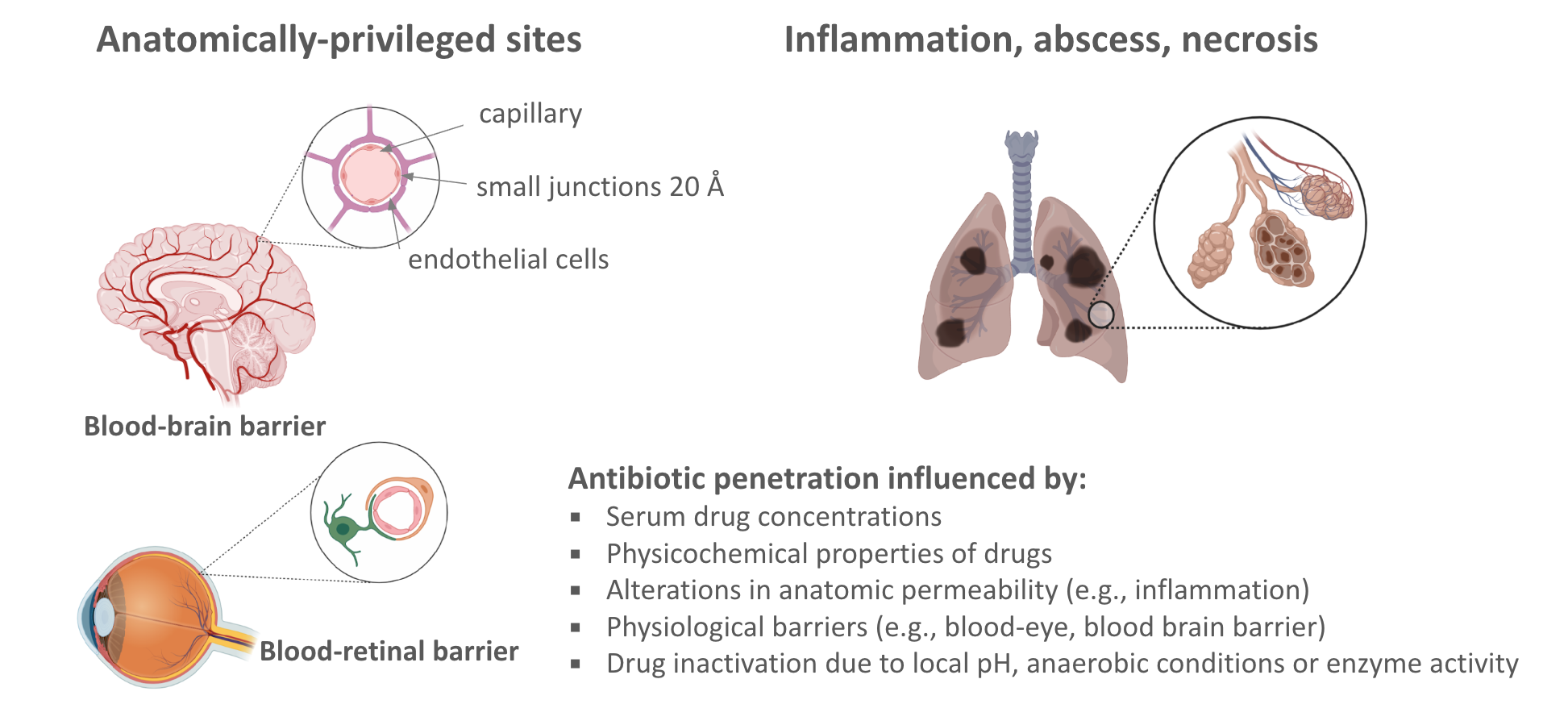
Anatomically-privileged sites
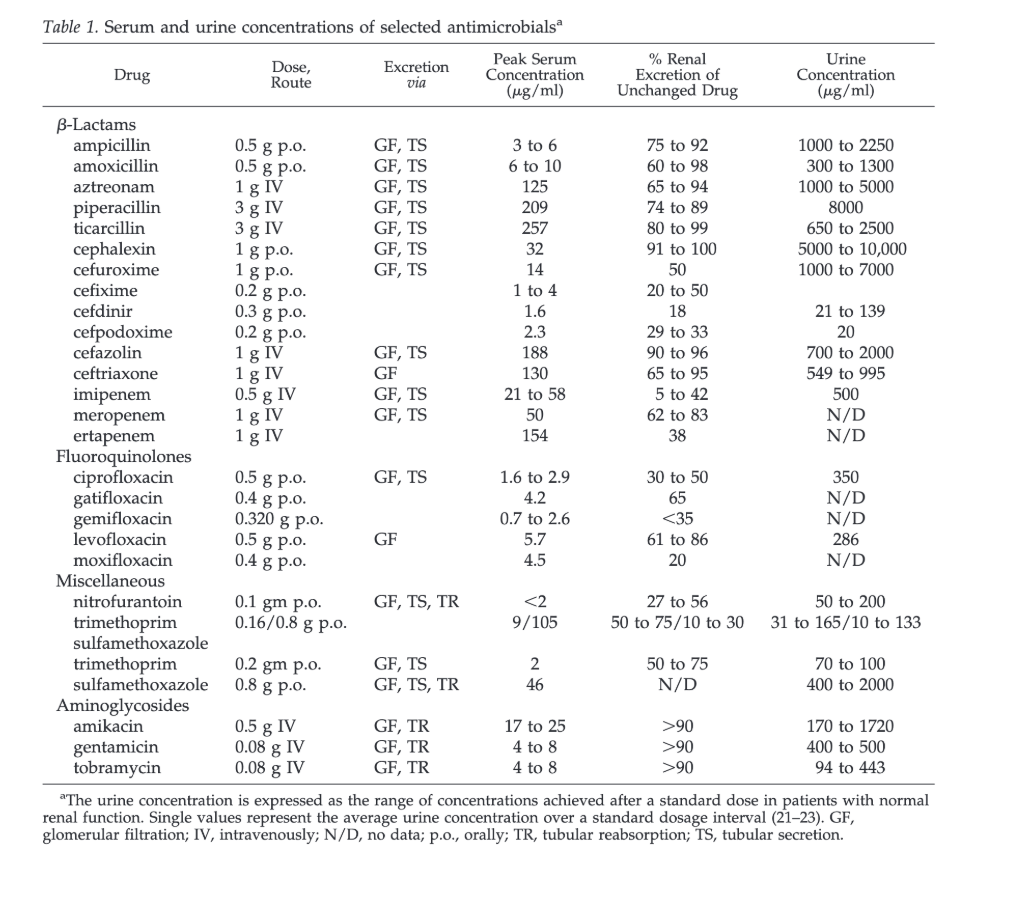
Match the antibiotic to site of infection
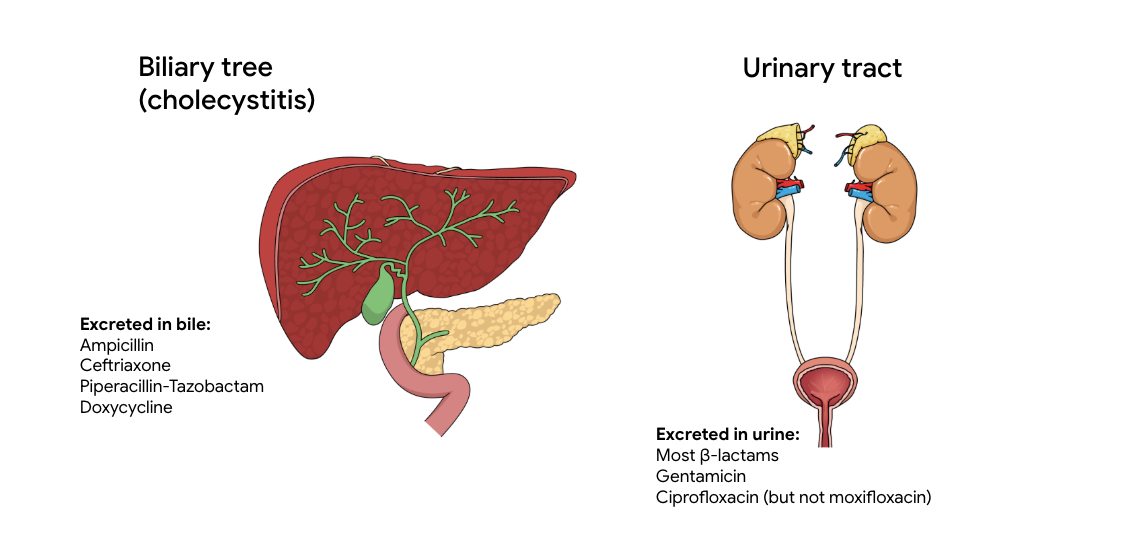
Urinary concentrations of antibiotics
Second key pharmacokinetic variable:
Clearance (CL)
![]()
Drug elimination from the body
Described by volume of blood removed of drug unit per time
Unit of measure mL/min or L/hr
Clearance is affected by patient’s disease, organ function genetics, interactions with other drugs…etc.
Total body clearance:
- CL renal + CL hepatic + CL other
Formulas for calculating antibiotic clearance can be found in the medical literature or some drug references
Most antibiotics are eliminated via the kidneys and maintenance doses must be adjusted for renal function

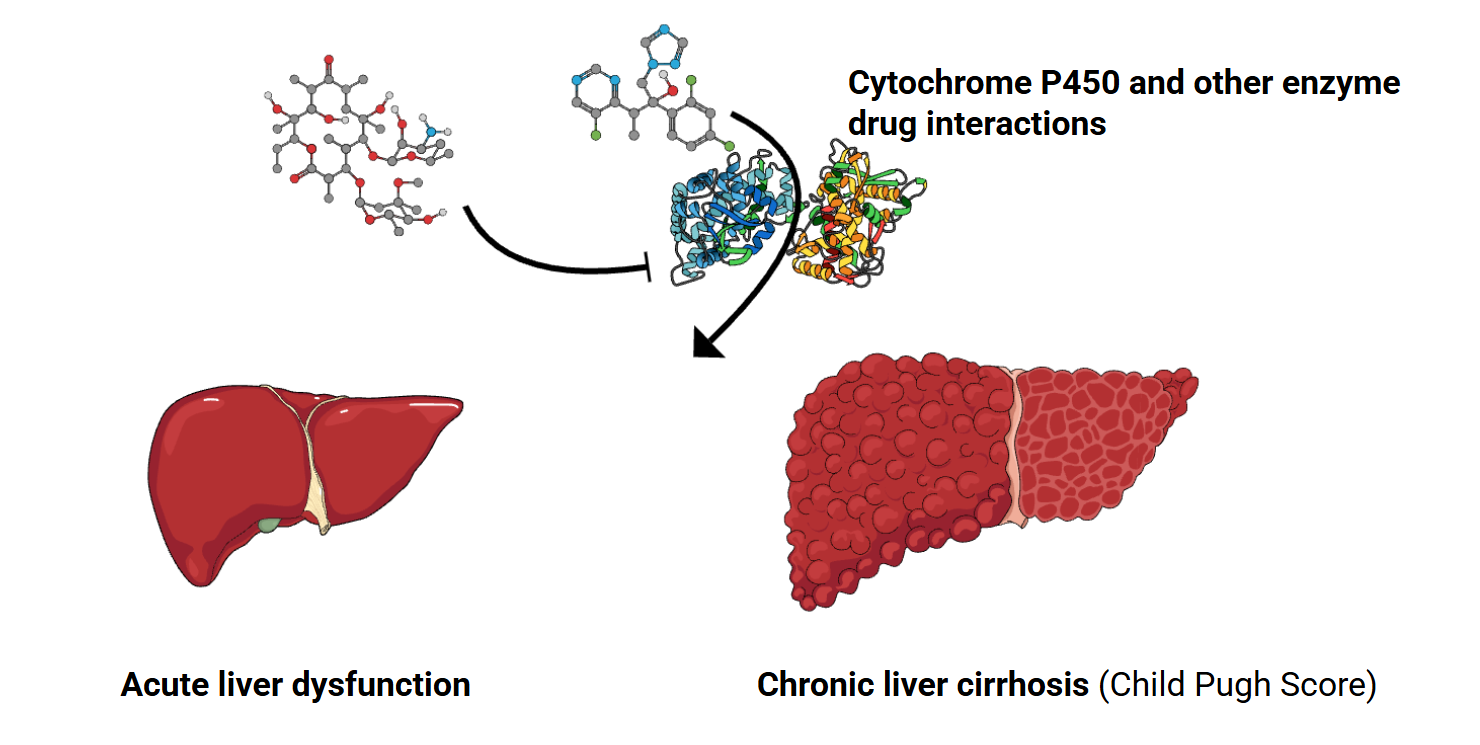
Hepatic clearance of antibiotics
PK/PD indices
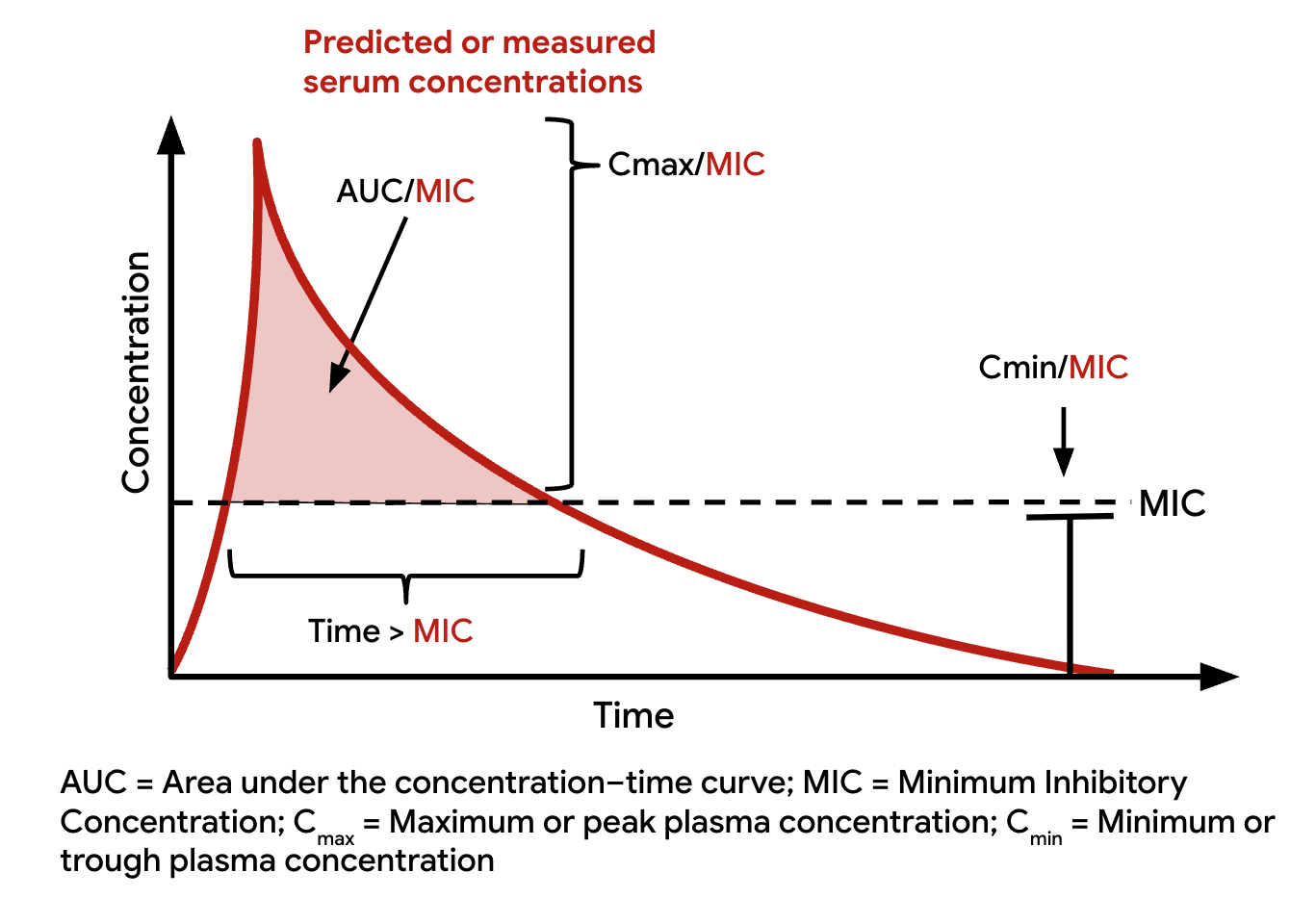
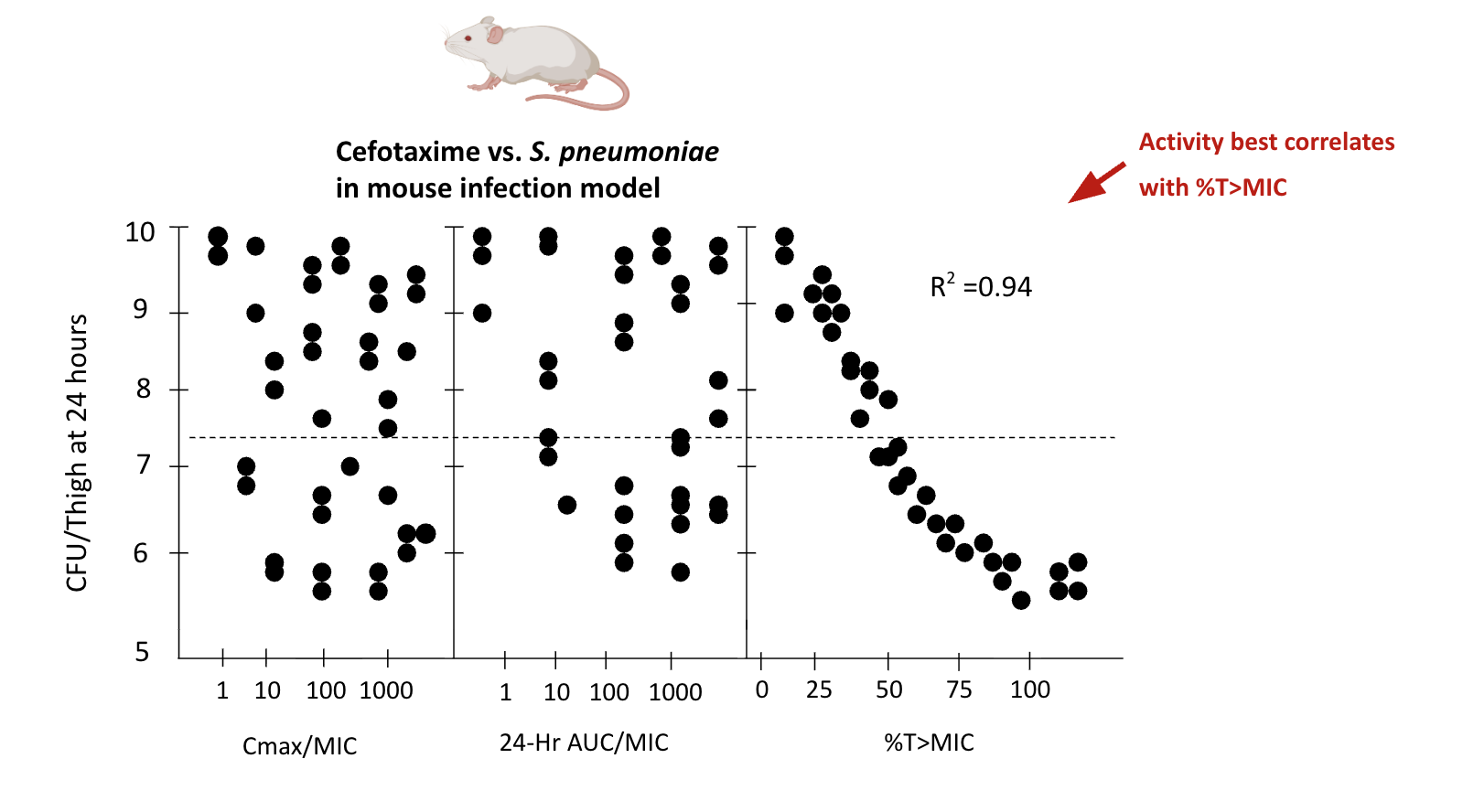
How is the PK/PD index identified?
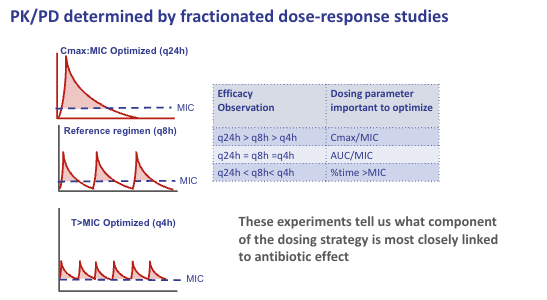
How are PK/PD indices identified?
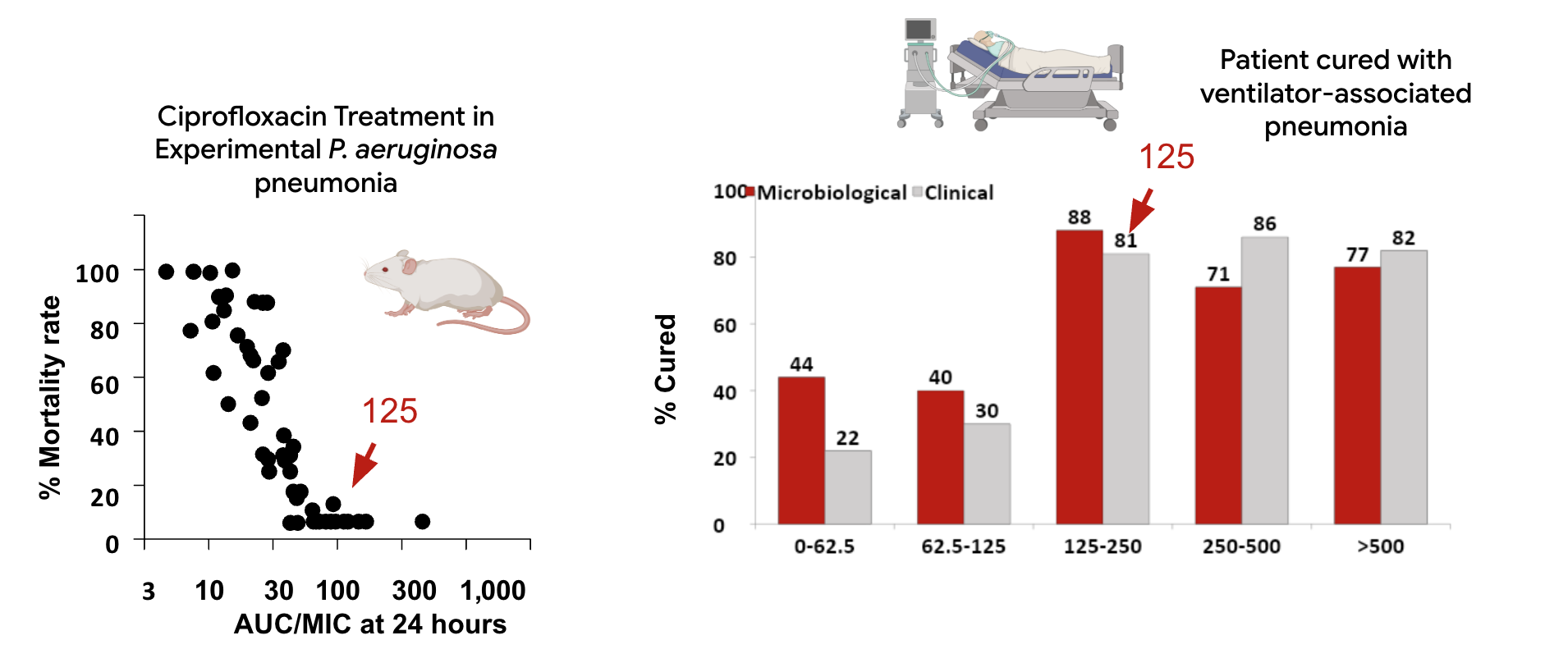
Do PK/PD indices correlate with
clinical outcome of antibiotic therapy
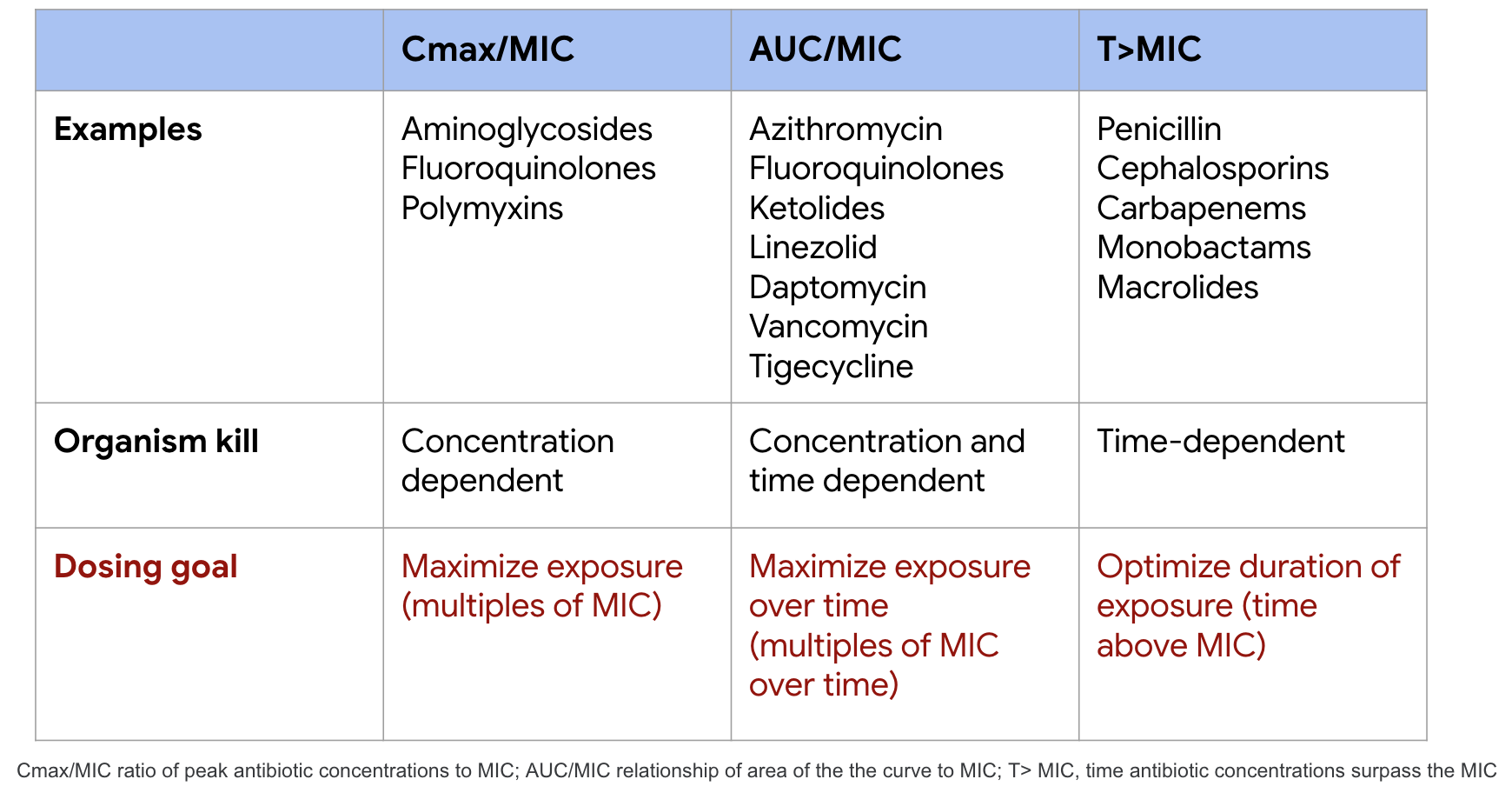
PK/PD characteristics of common
antibiotic classes
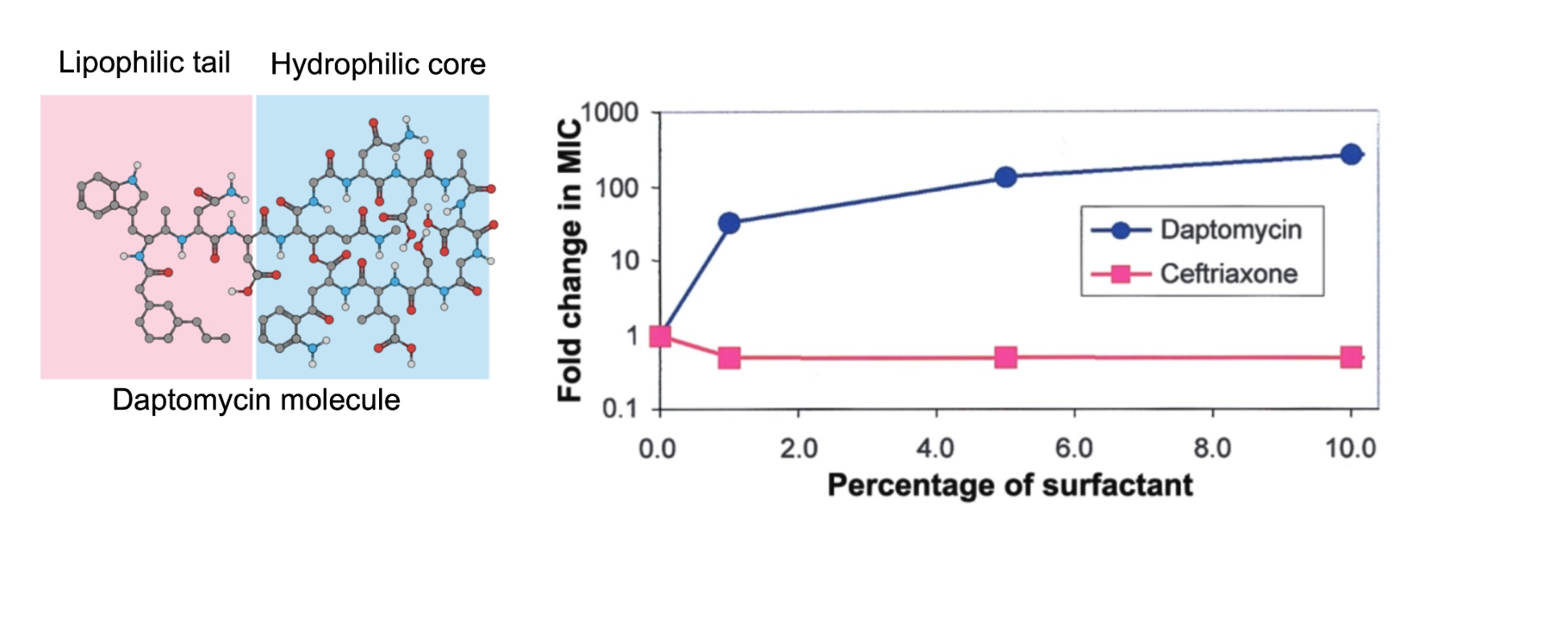
Daptomycin is inactivated in the lung
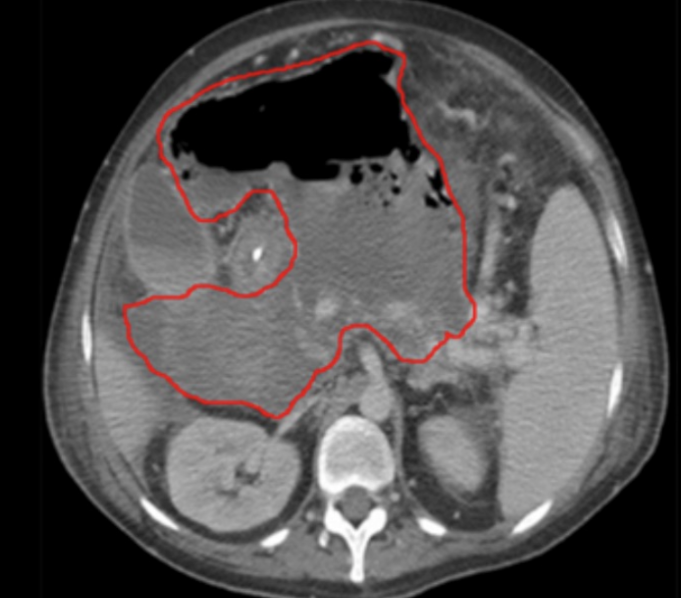
Antibiotic activity in abscess
Aminoglycosides
Bind and are inactivated by purulent material
Decrease aminoglycoside uptake into facultative aerobic bacteria at low pH
Penicillins and tetracyclines
Bound by hemoglobin, less effective with hematoma formation
Emphasizes importance of source control (abscess drainage, removal of prosthetic material)
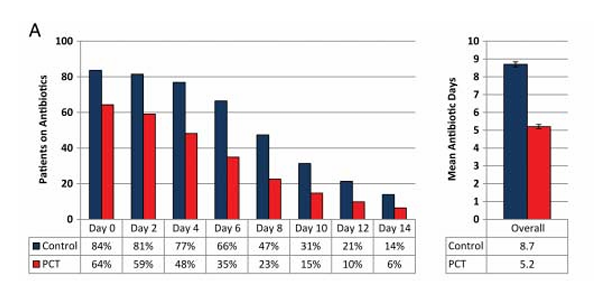
Principle #7: De-escalate antibiotic therapy based on microbiology results and clinical (biomarker) responses
Incorporation of procalcitonin into therapeutic decisions reduces antibiotic use
Choosing therapy :
gram-stain vs. guidelines
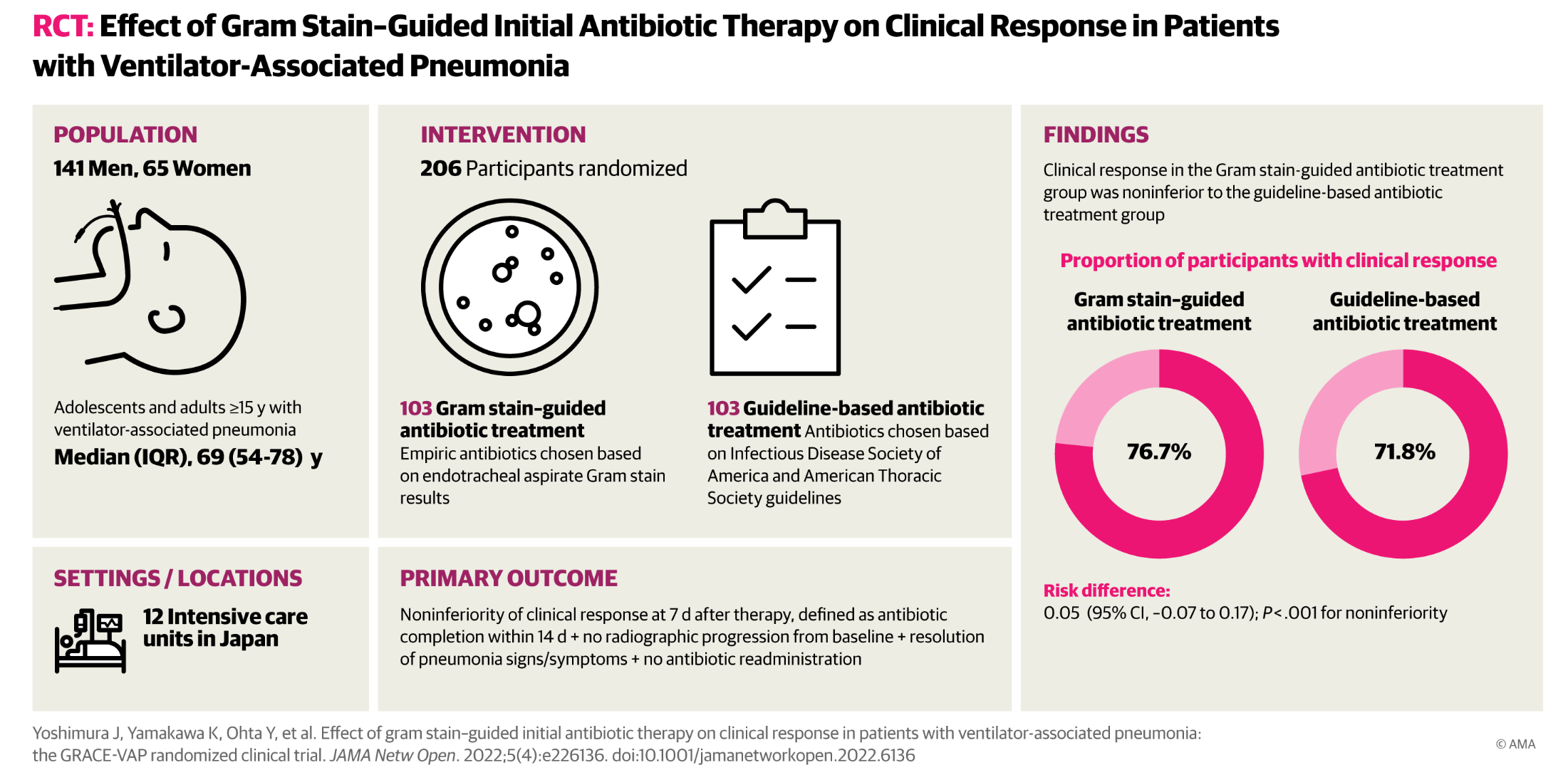
Gram strain guided therapy resulted in a 30% reduction in use of anti-pseudomonal agents and 40% reduction in MRSA agents
Gram-stain guided therapy resulted in higher rate of appropriate antibiotic escalation (7% vs. 1%, p=0.03)
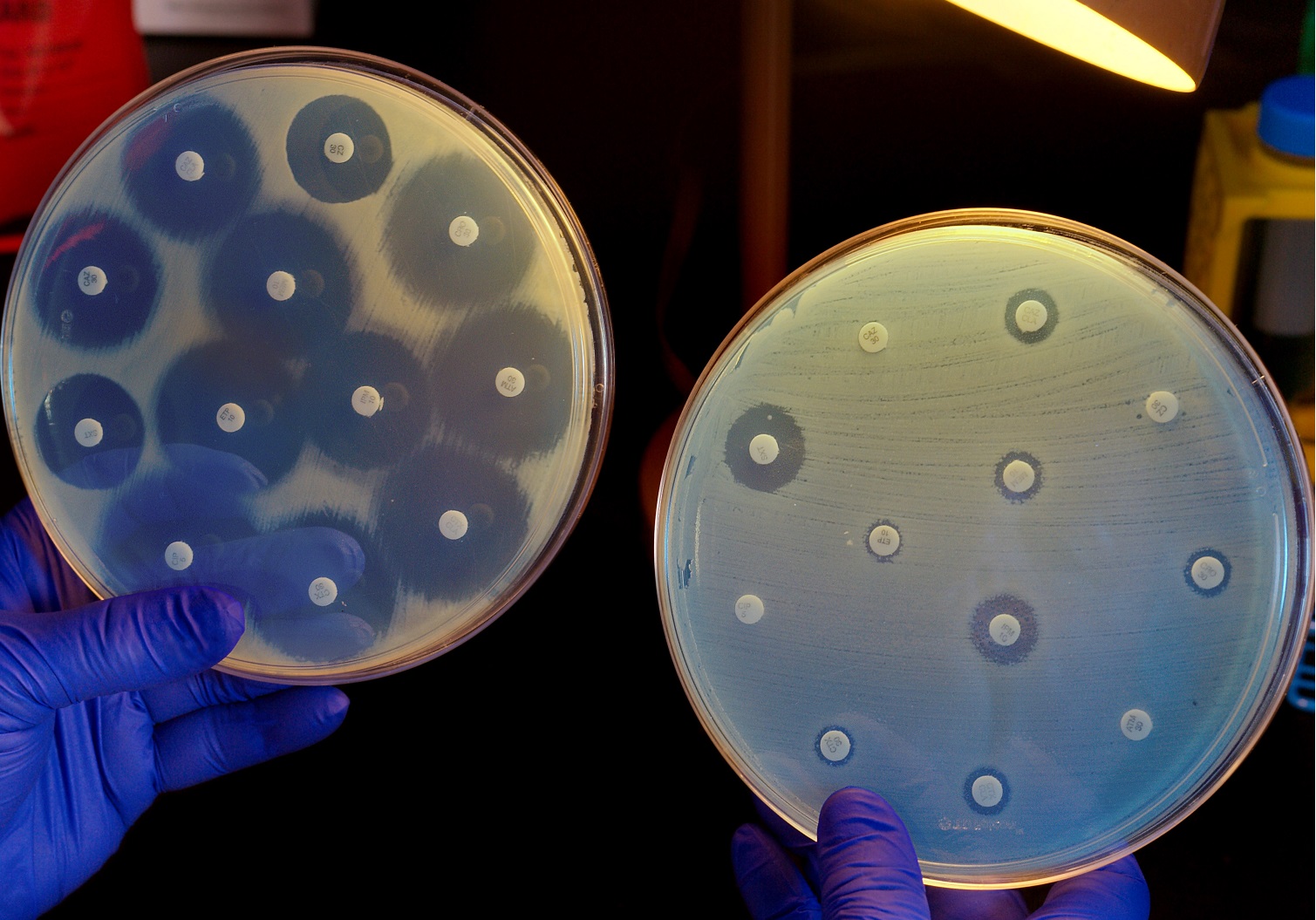
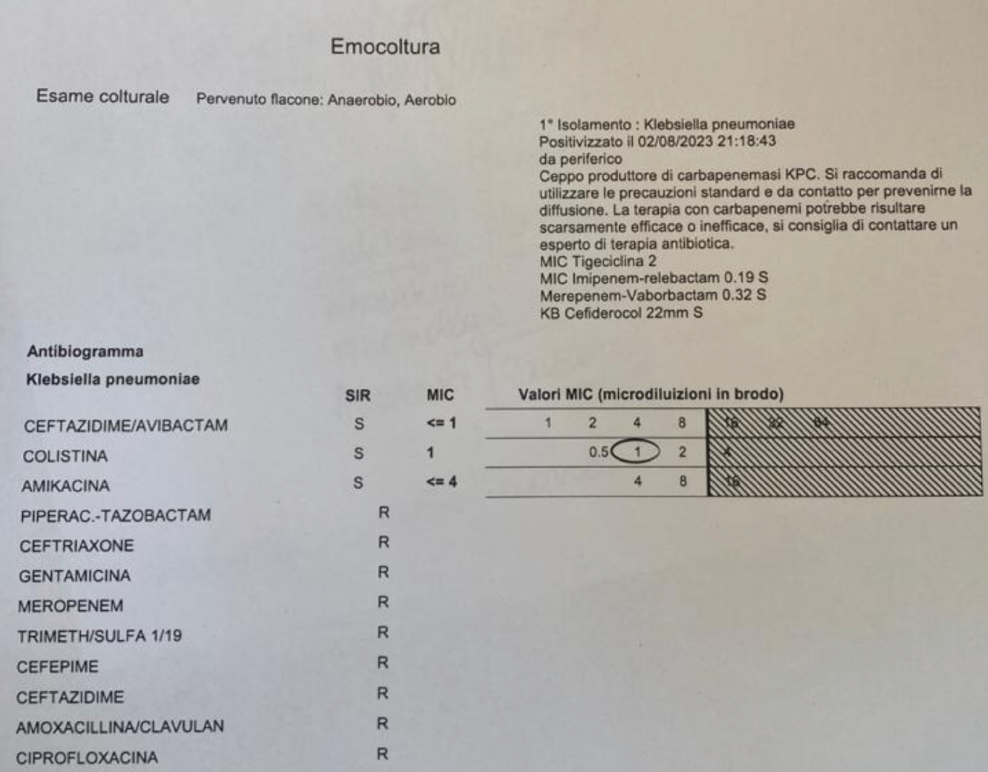
Susceptibility testing-Mean inhibitory concentration
Source control
| Occult subcutaneous abscess in cellulitis | New abscess formation in intraabdominal infection | Empyema in community-acquired pneumonia | Visceral or skeletal abscess in patient with bacteremia | Failure to remove a central venous catheter |
 |
 |
 |
|
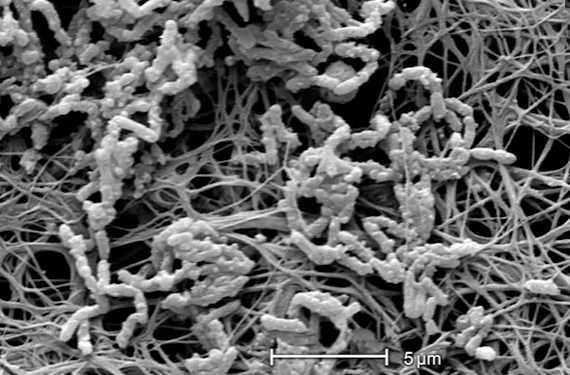 |
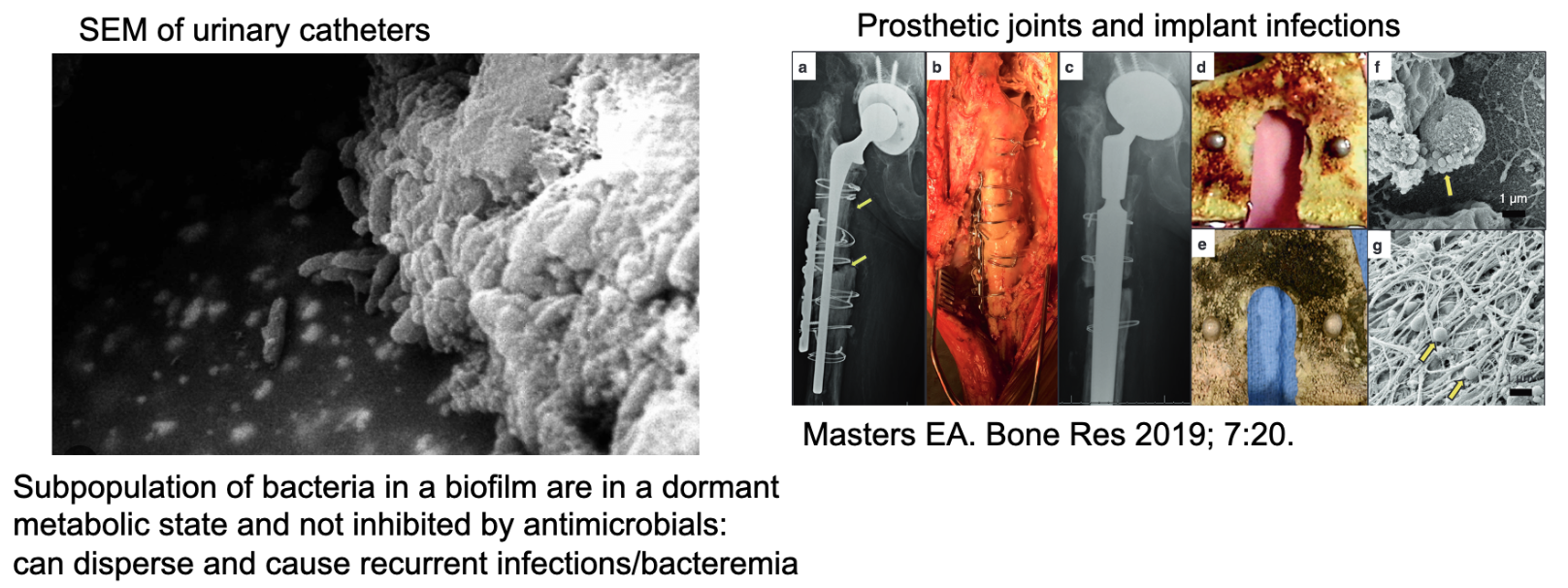
Biofilms: A key source of antibiotic failure
Myth 1:
“Bactericidal” antibiotics are more effective
than “bacteriostatic”
Bactericidal activity: concentration of drug that results in 1000-fold reduction in inoculum within 24 hours
Bactericidal antibiotic: MBC of drug is 4-fold or less above the MIC
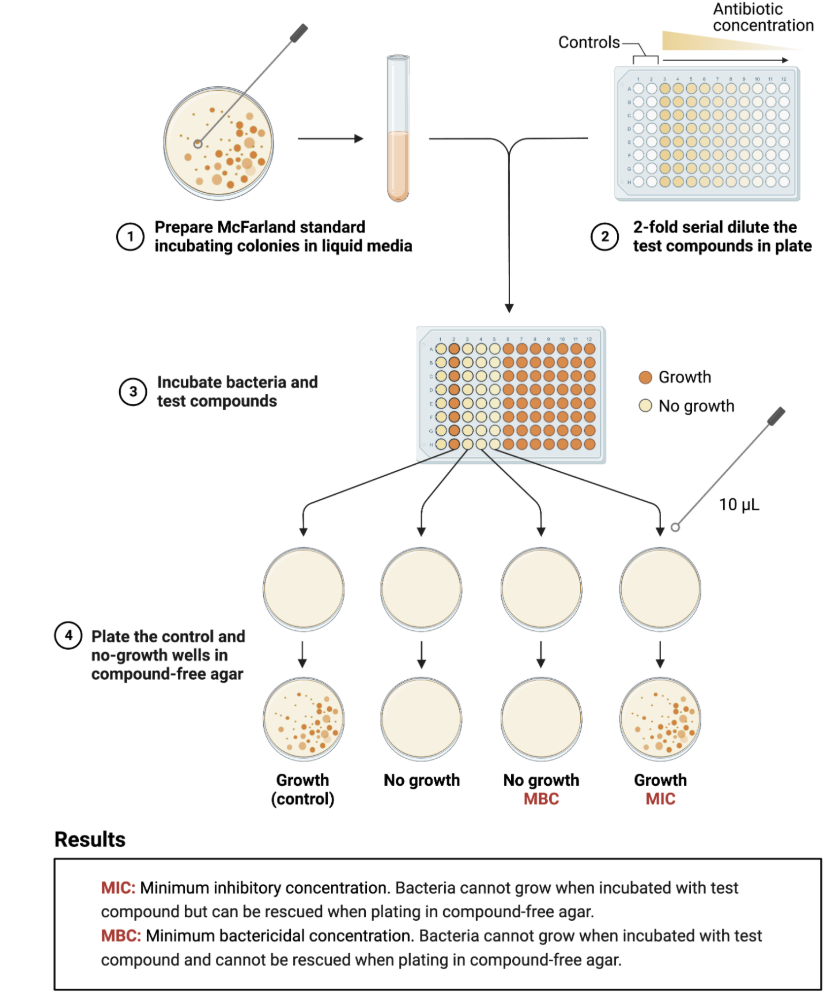
However, “bacteriostatic” drugs do kill bacteria, they just require higher concentrations
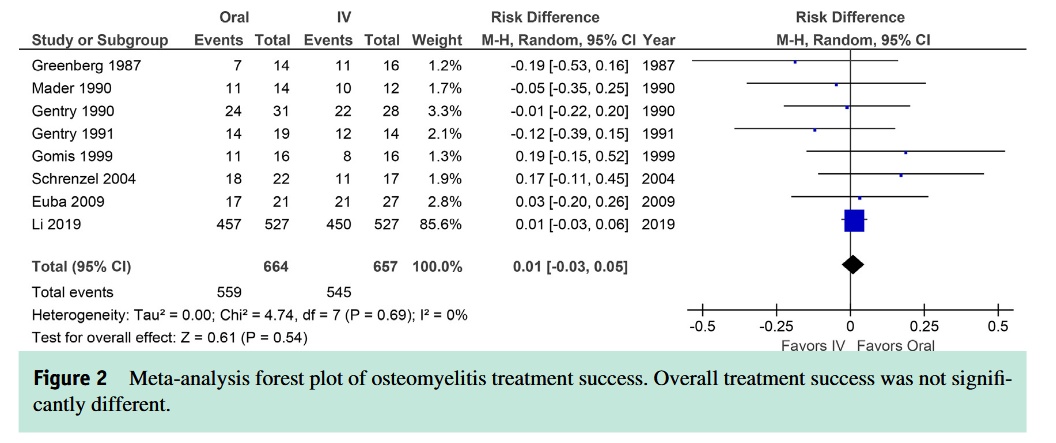
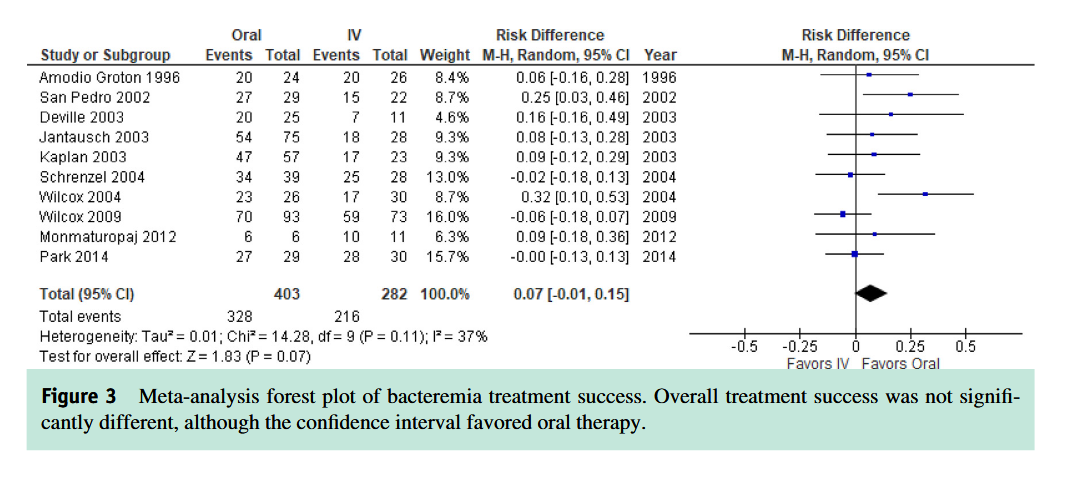
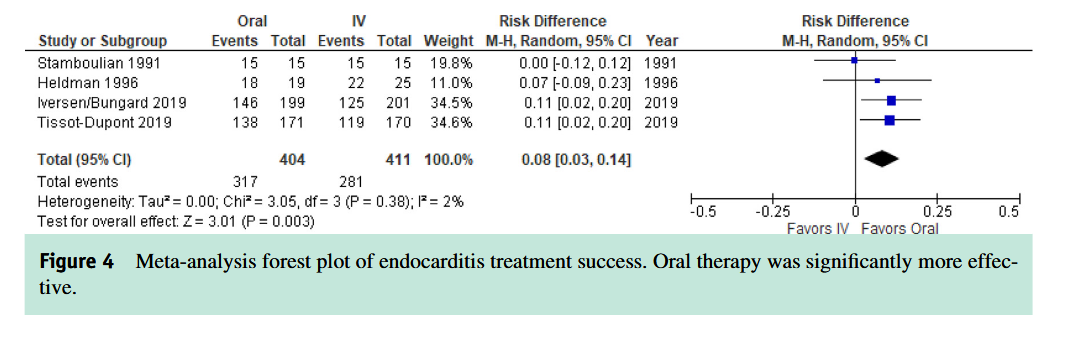
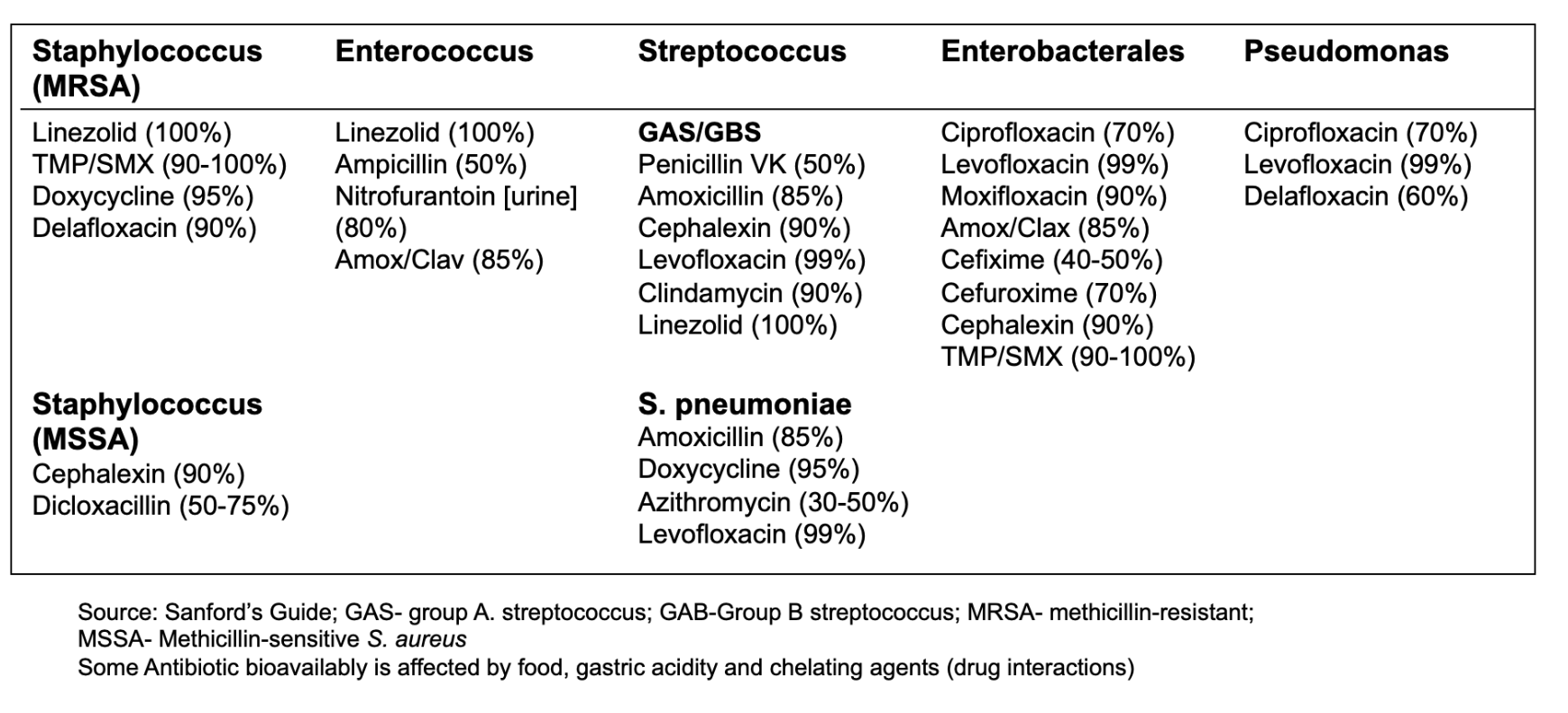
Oral is the new IV
Oral bioavailability of antibiotics
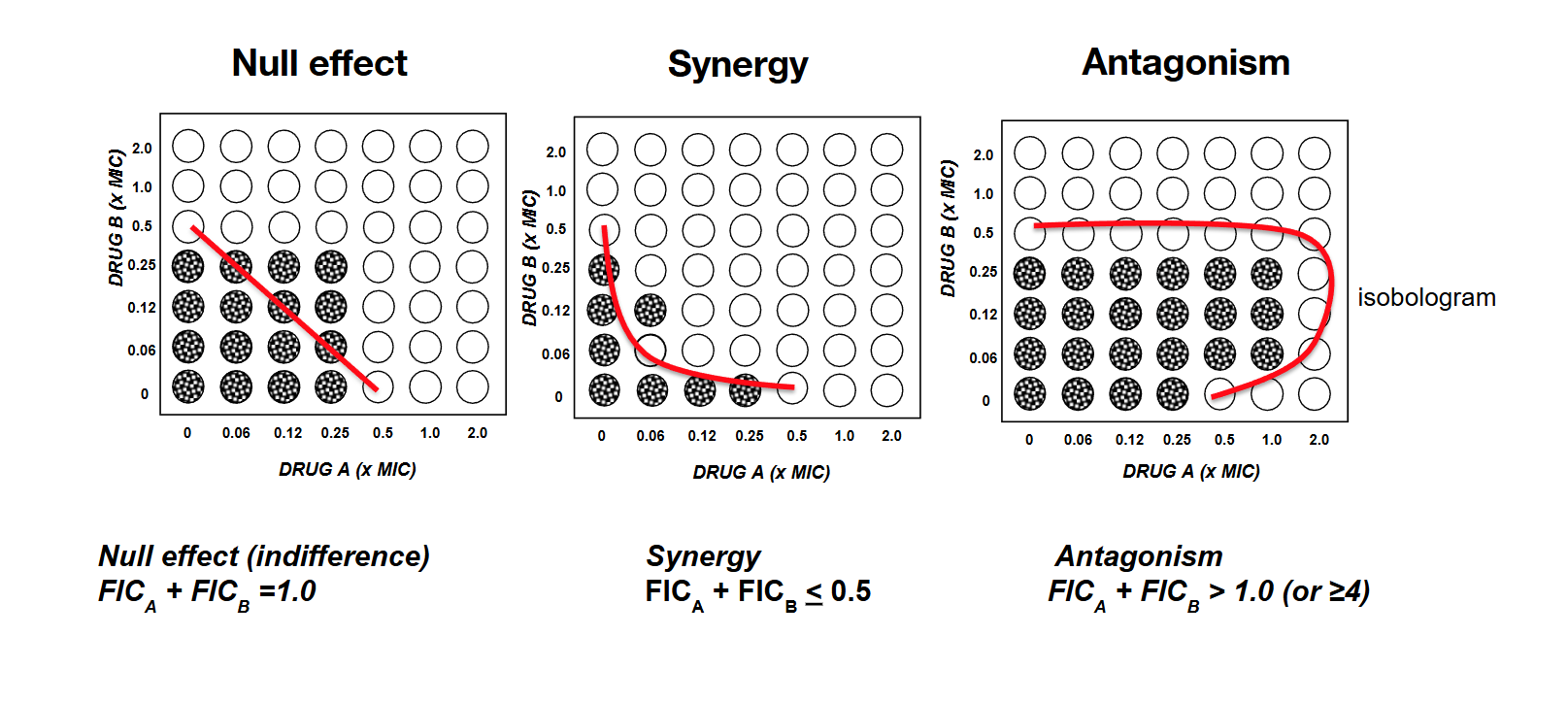
Microbiological rationale: Checkerboard test
Exotoxin-mediated infections-
Necrotizing fasciitis

- Streptococci or Clostridium infections that are extremely destructive and aggressive
- Addition of clindamycin or linezolid as a 2nd agent terminates protein synthesis: shutting down toxin production in the bacteria
- Adding protein synthesis inhibitors to backbone antibacterial therapy has been associated with improved survival in retrospective studies
Combination therapy for
Pseudomonas aeruginosa
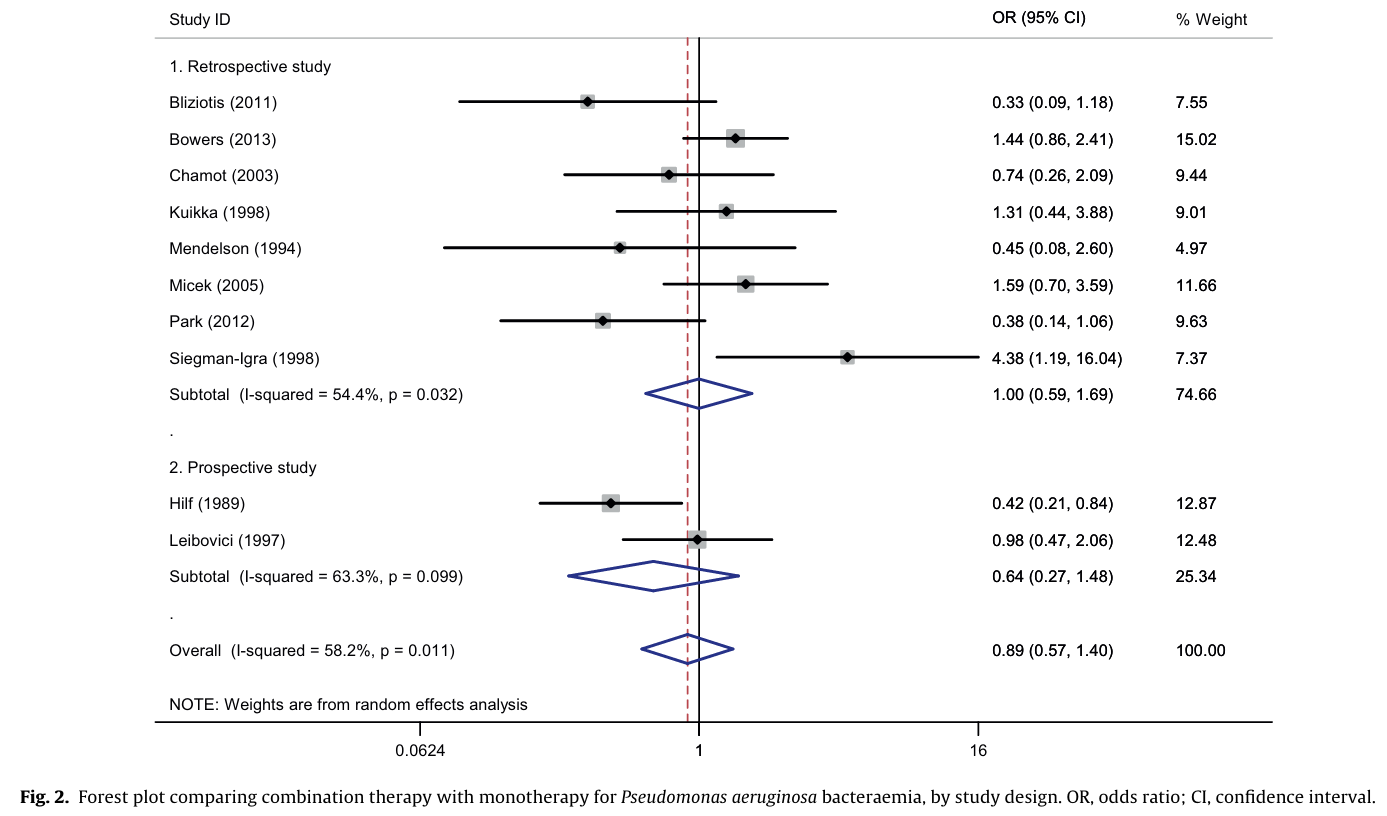
Combination therapy studies for severe infections/sepsis have also found no advantage for dual therapy
Dual therapy more likely to result in toxicity and microbiome harm- potential resistance to 2 drug classes