Fever of Unknown Origin
2026-03-01
Fever of Unknown Origin (FUO)
Prof. Russell E. Lewis
Department of Molecular Medicine
University of Padua
russelledward.lewis@unipd.it
https://github.com/Russlewisbo
slides available at: www.padovaid.com
 |
.svg) |
The history of fever
- 10th Century BCE Persian Physician Akhawayni defined a system for fever curves in Hidāyat al-Muta’allimīn fī al-Tibb (The Student’s Handbook of Medicine)
- Hippocratic physicians proposed that body temperature, and physiologic harmony in general, involved a delicate balance among four corporal humors—blood, phlegm, black bile, and yellow bile.
- Fever was due to excess of yellow bile (many infections caused jaundice)
- Galen: many types of fever developed from putrefaction of humors.
- Middle ages: demonic possession
- 18th century (Harvey’s discovery of circulation)- friction of blood flow through body causing fermentation and putrefaction in intestines
- Claude Bernard in the 19th century- metabolic processes in the body
Febris - Roman Goddess of Fever

The legend of Febris was said to center around the haunting marshes of Camagna in Southern Italy where like clockwork every year, the people would become deathly ill with a mysterious disease. She was so feared by the Romans that the suffering population had created a cult to Febris. They went so far as to wear protective amulets and build her temples in order to worship her to win her favour.
Early thermometers
A typical design of a thermoscope is a tube in which a liquid rises and falls as the temperature changes. The Sanctorius thermoscope. Source: Professor Francis Ring, the University of Leeds
Fever in modern medicine
Wunderlich’s pioneering studies of thermometry reported normal temperature at 37°C
Since the 19th century, humans have become gradually colder - 0.05° to 0.5°C per decade!
- Current normal range is 36.3 to 36.5°C
- Less manual labor, less chronic inflammation-infection, poor dental health, increased body mass
Mackowiak (1992): mean oral temperature 36.8 ± 0.4°C; only 8% had 37°C
Fever now defined as: early-morning temperature ≥37.2°C or anytime ≥ 37.8°C

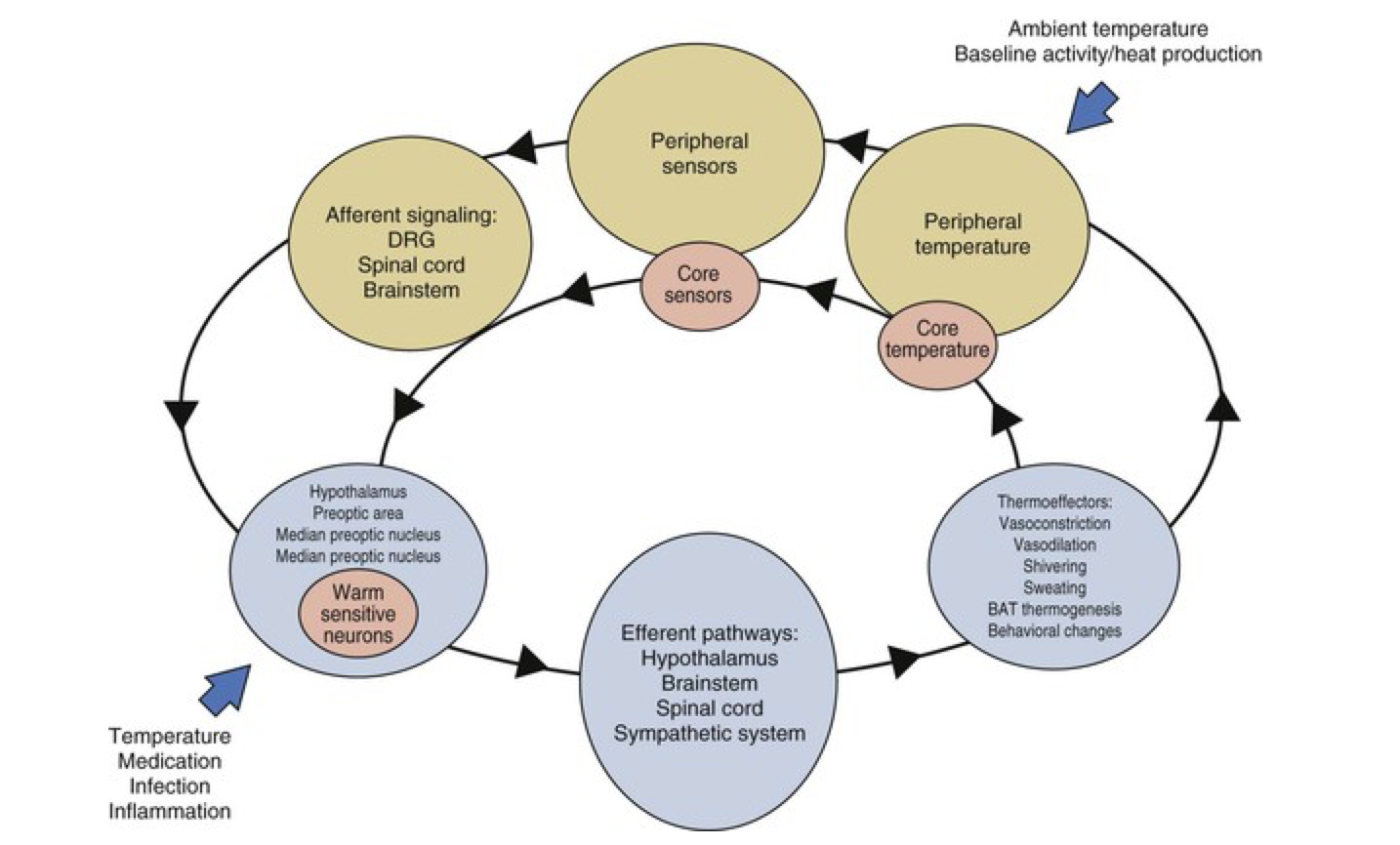
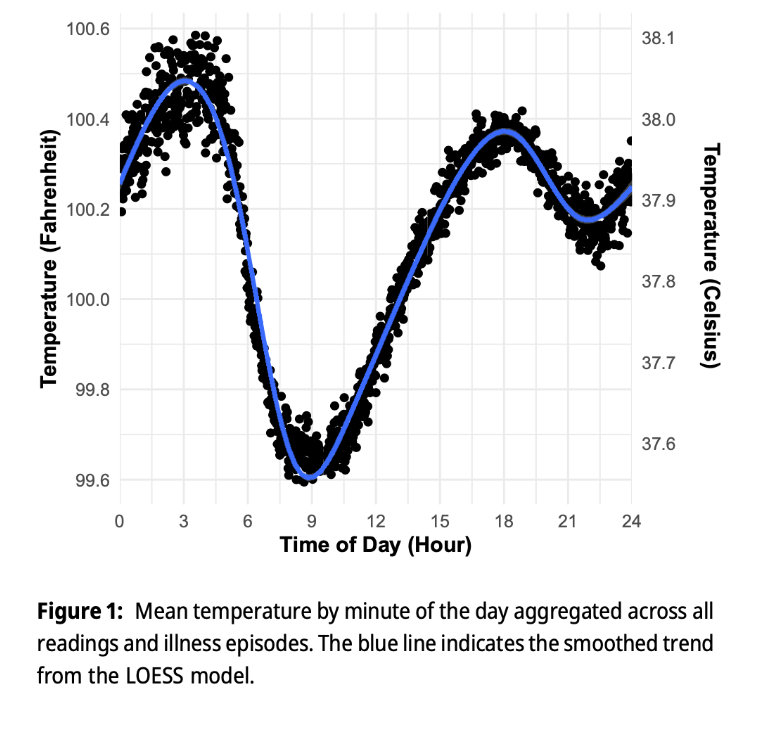
Thermal homeostasis
Diurinal pattern of body temperature
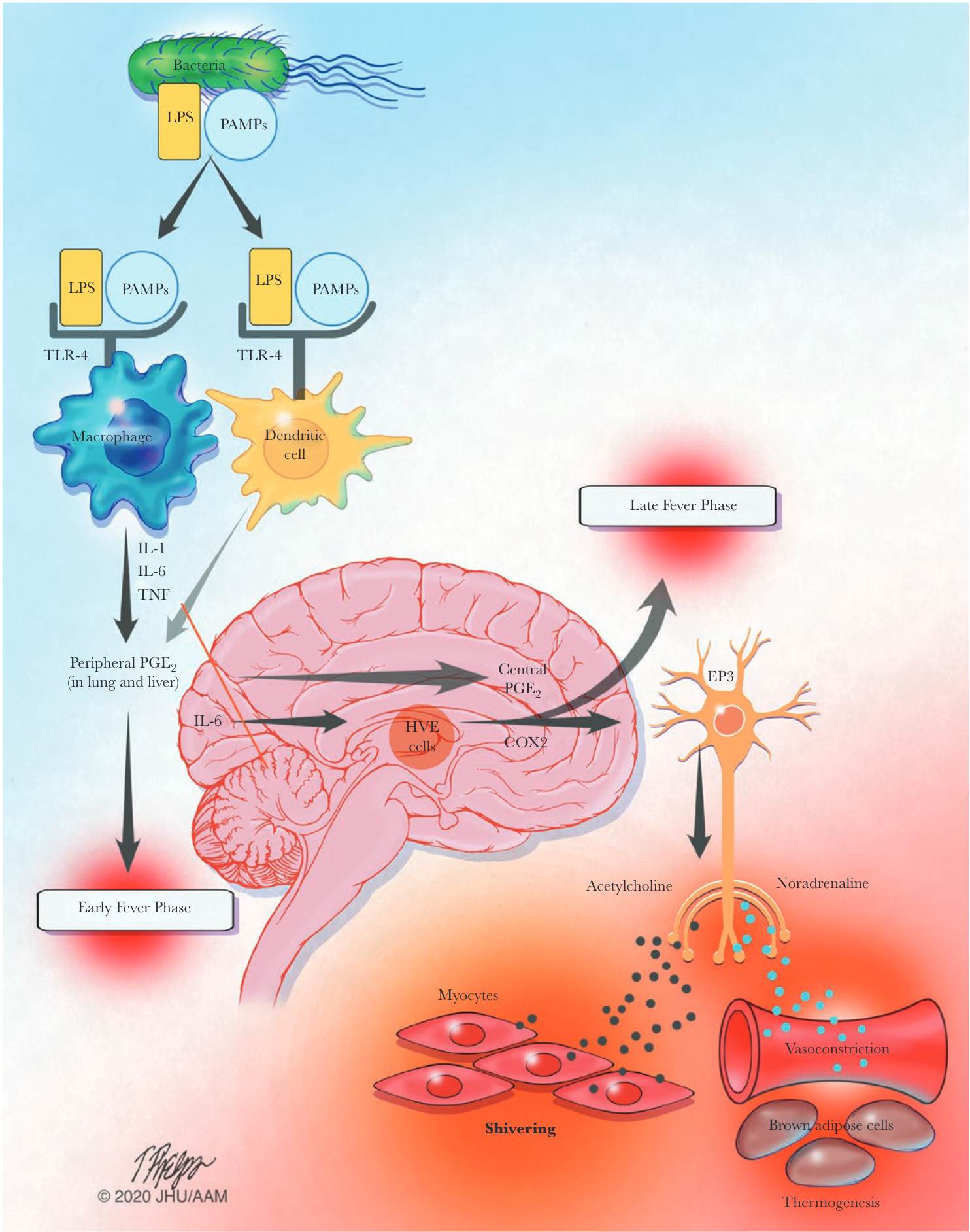
Infection-associated fever - The febrile response
Fever therapy to treat neurosyphilis

Treponema pallidum is uniquely sensitive to increased temperatures
Fever therapy involved purposely infecting the patient with Plasmodium vivax with control of the infection with anti- malarians while maintaining the fever it causes to the detriment of other, ongoing, and then-incurable infections such as late-stage syphilis
This type of pyrotherapy was most famously used by psychiatrist Julius Wagner-Jauregg, who won the Nobel Prize for Medicine in 1927 for his elaboration of the procedure in treating neurosyphilis
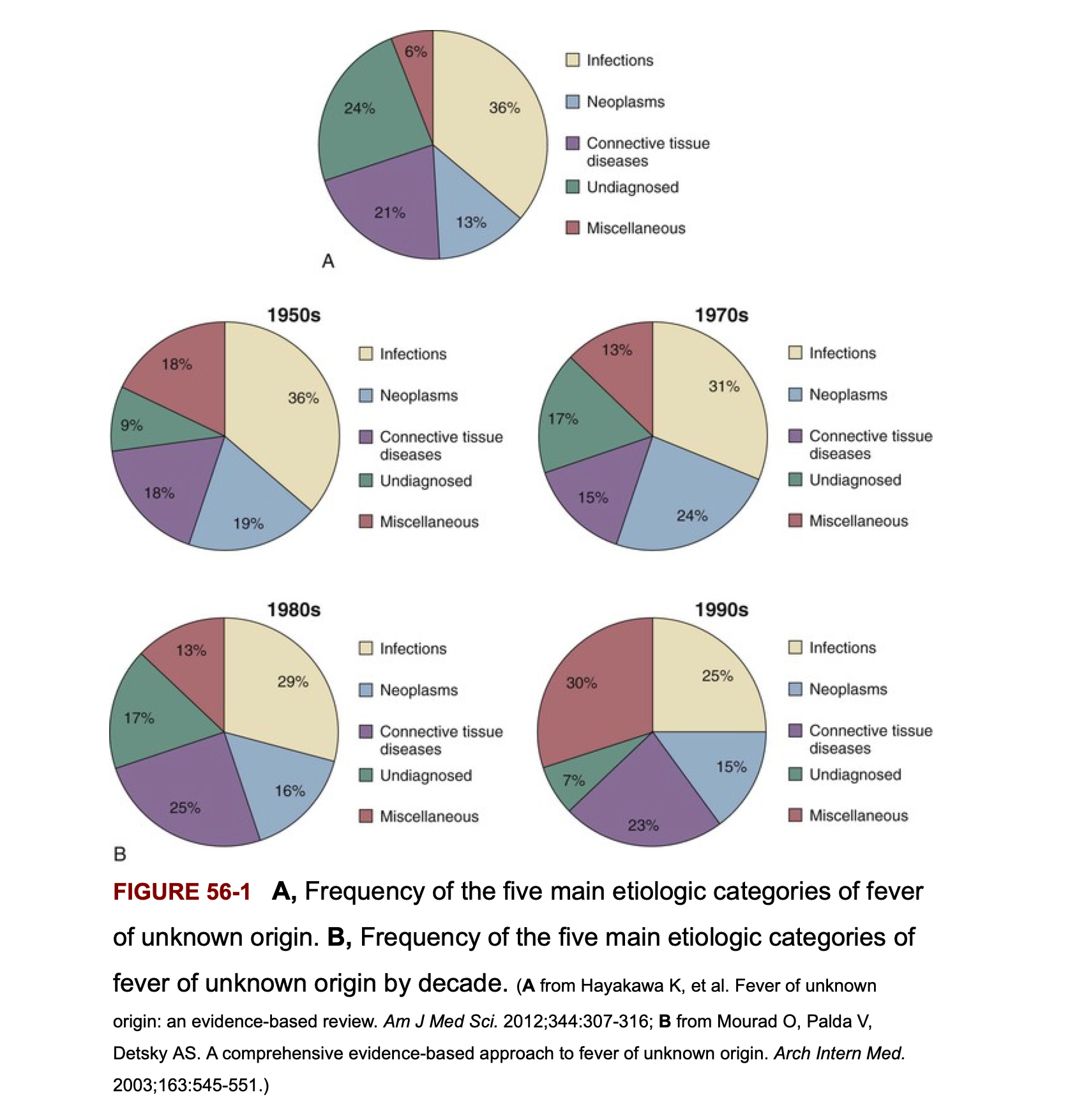
Frequency of the 5 main etiologic categories of FUO
Classic FUO in infants and children
- Respiratory tract infections - viral, atypical organisms
- Other infections:
- UTIs (especially important in young girls)
- Brucellosis, tuberculosis, bartonellosis
- Systemic inflammatory conditions:
- Kawasaki disease (critical, age < 5 years)
- Inflammatory bowel diseases
- Still’s disease (juvenile rheumatoid arthritis)
- Note: Connective tissue diseases and cancers are generally rare in children
- Important: Joint involvement is a sign of serious disorder - consider endocarditis, leukemia, connective tissue disease

Classic FUO in elderly patients
- In developed countries: connective tissue diseases > infections
- Temporal arteritis (critical diagnosis - risk of blindness)
- Polymyalgia rheumatica
- Other vasculitides
- Diagnostic challenge: symptoms are subacute and non-specific, easily attributed to aging
- Infections still need to be considered:
- Intra-abdominal abscess
- Complicated UTIs (often without pyuria)
- Tuberculosis (may be reactivation)
- Endocarditis (prosthetic valves more common in elderly)
- Malignancy: solid tumors and hematologic malignancies increase with age

Fever in post-operative patients

- Epidemiology: > 1/3 of patients manifest fever in first 5 days post-surgery
- Infectious vs. non-infectious: < 10% of febrile patients have an identified source or positive cultures
- Pathophysiology: Fever may represent a physiological response to surgically-induced tissue injury
- Release of pyrogenic cytokines and interleukins
- Not necessarily indicative of infection
- Clinical pearl: Early fever (post-op day 1-3) is usually non-infectious; later fever (day 5+) warrants infection investigation
FUO in ICU patients
- Early fevers are common and often non-infectious
- Associated with good prognosis
- Related to inflammatory response to critical illness
- Prolonged fever carries a poorer prognosis
- Common complications:
- Sinusitis (from mechanical ventilation, supine positioning, feeding tubes)
- Ventilator-associated pneumonia
- Catheter-related bloodstream infections
- Other causes similar to nosocomial FUO
- Abscess, drug fever, septic thrombophlebitis, pulmonary emboli

FUO in stroke patients
- Non-infective fevers are common in stroke patients
- Occur earlier after stroke than infection
- Related to hypothalamic injury and cytokine release
- Infection-related complications:
- UTI (from urinary catheterization)
- Aspiration pneumonia
- DVT/PE
- Clinical challenge: Distinguishing fever from infarct-related inflammation vs. infection can be difficult; broad-spectrum antibiotics are often given empirically
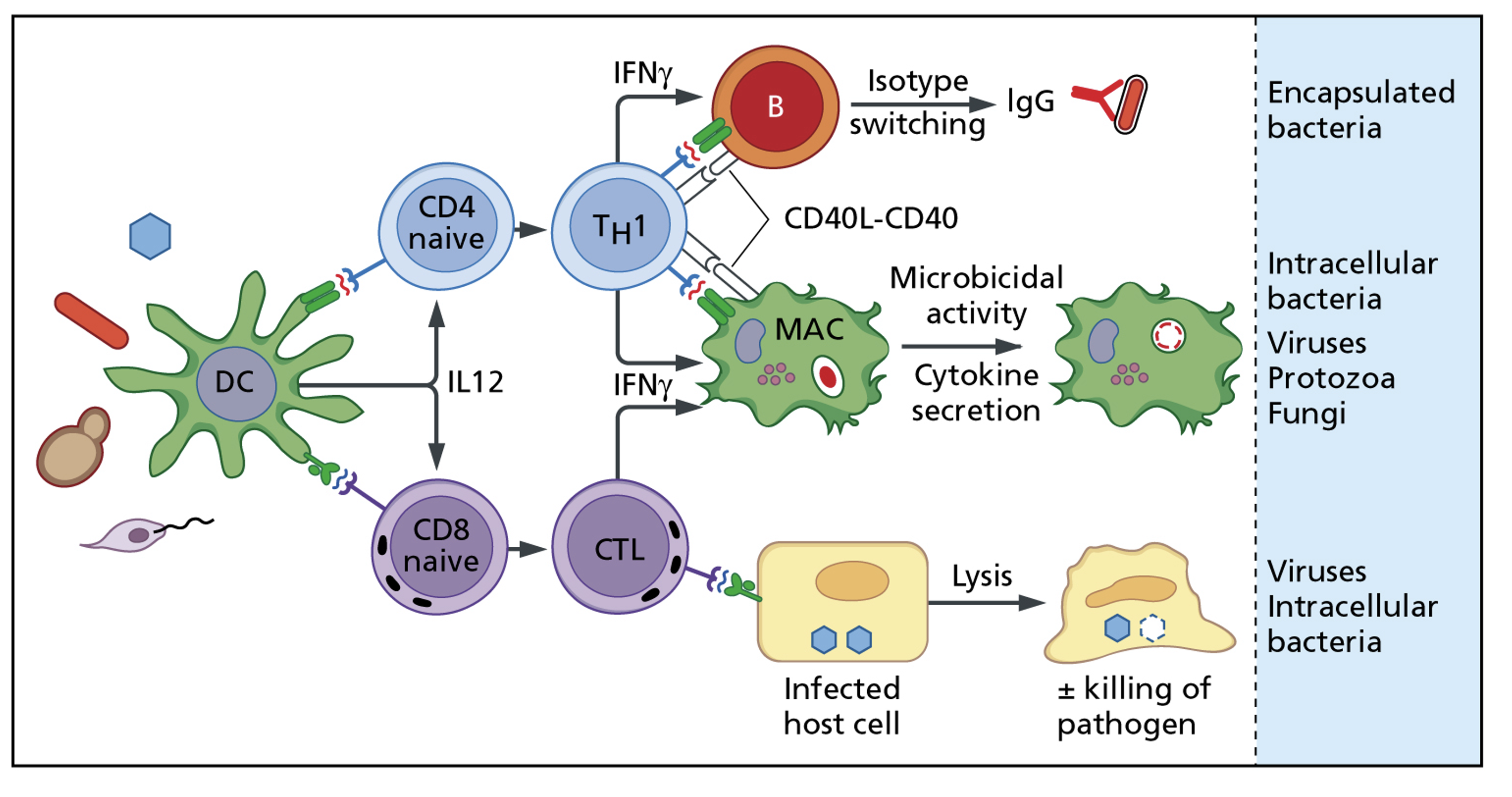
Cell-mediated immunity - Th1 pathway
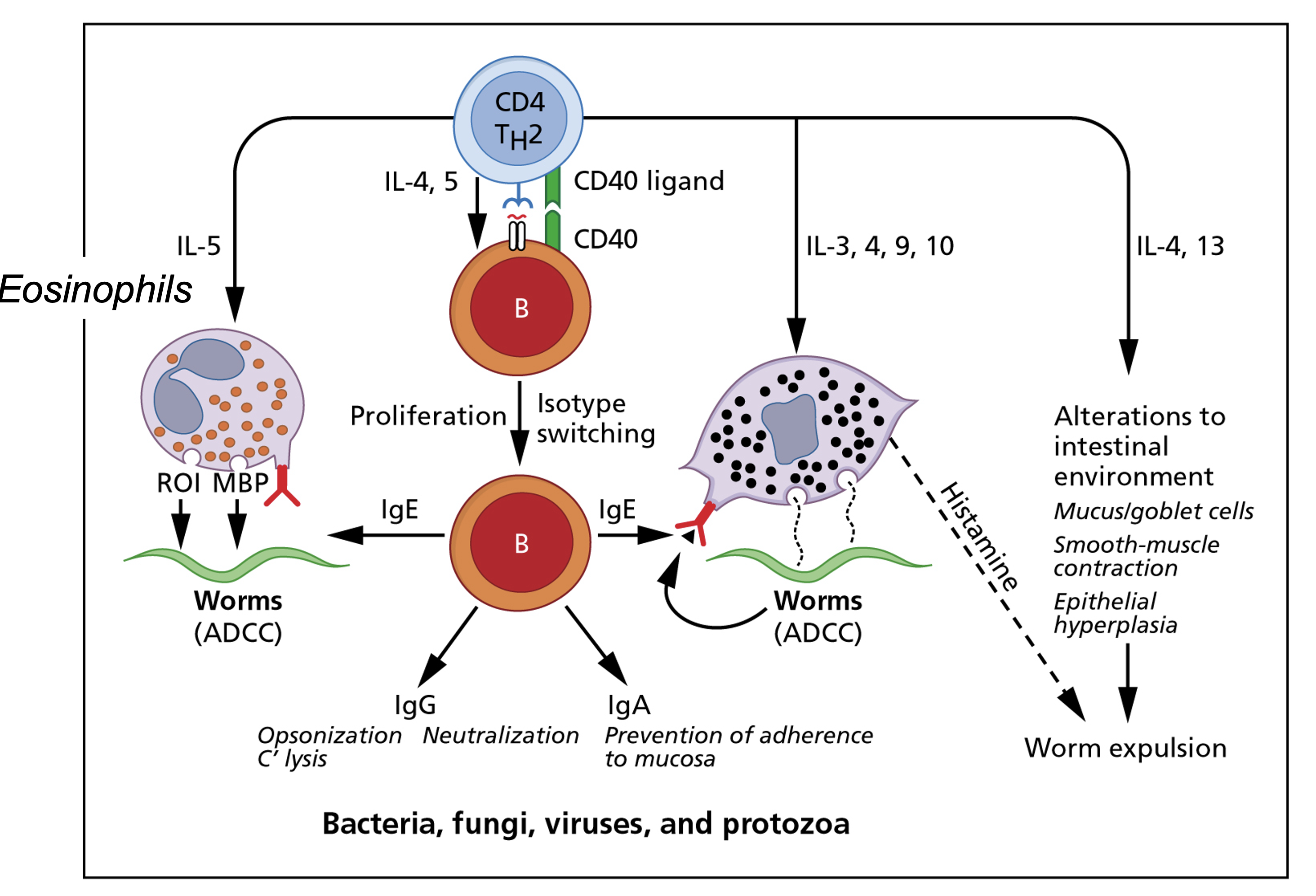
Cell-mediated immunity - Th2 pathway
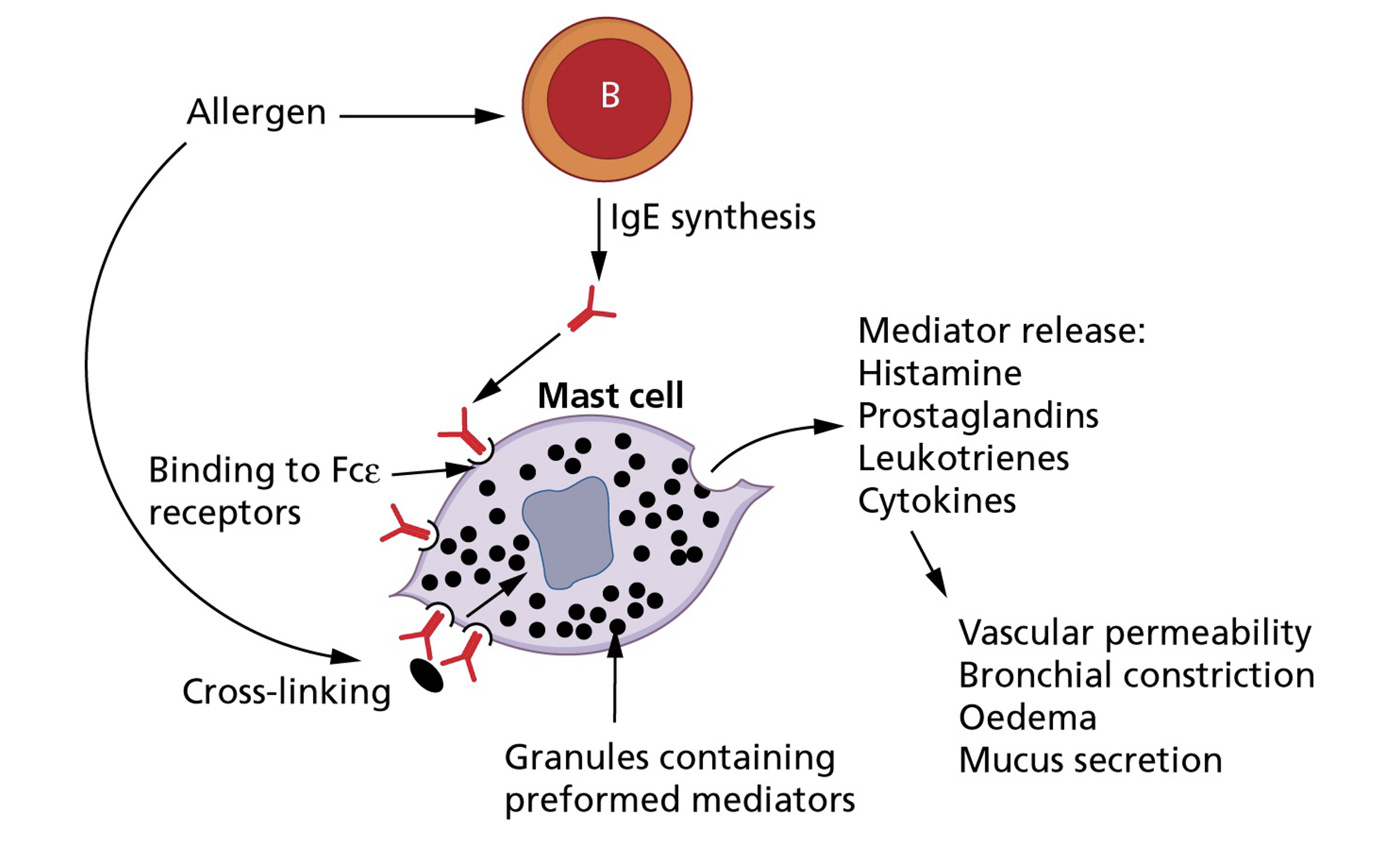
Cell-mediated immunity -
Drug allergy (Type IV hypersensitivity)
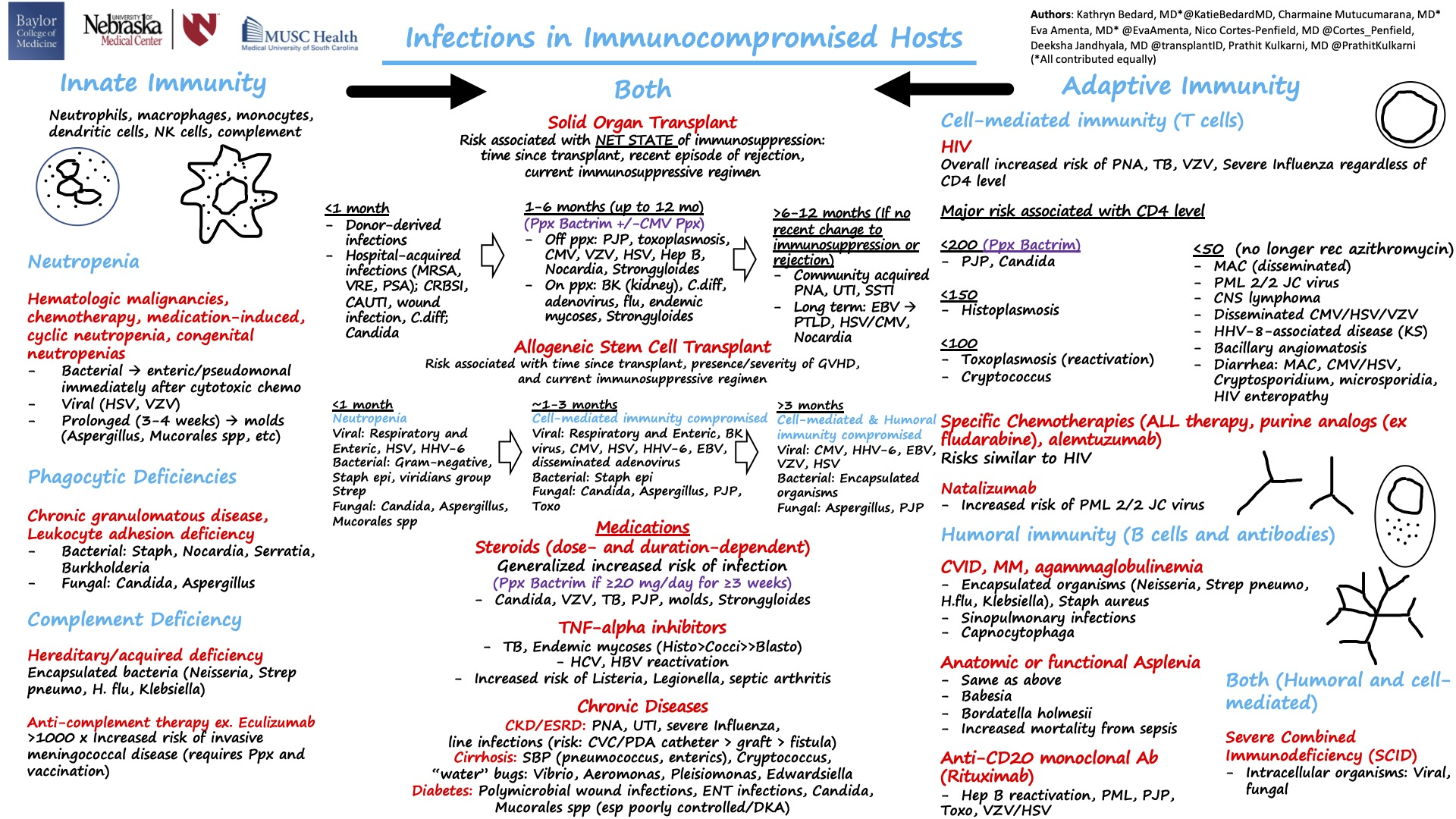
Infections in immunocompromised hosts:
A summary in one slide!
Continuous sustained fever
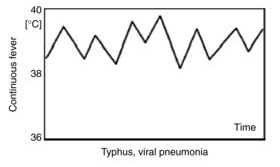
Continuous fever with slight remission not exceeding 2°C
- Lobar and gram-negative pneumonia
- Rickettsiosis
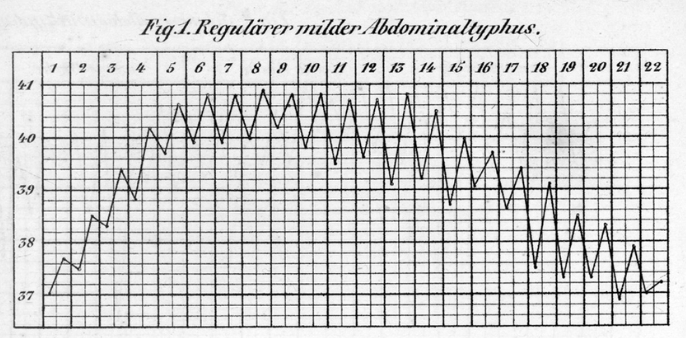
- Typhoid fever
- CNS disorders
- Tularemia
- Falciparum (malignant tertian) malaria
Intermittent (quotidian) fever
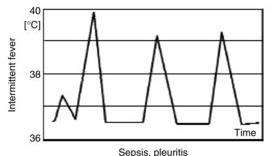
- Intermittent fever with wide fluctuations, usually normal or low in the morning and peaking between 4:00 and 8:00 PM
- Localized pyogenic infections and bacterial endocarditis with chills and leukocytosis
- Malaria may present with daily (quotidian), every 3rd day (tertian), or every 4th day (quartan) patterns
- Double quotidian pattern (two daily spikes) seen with:
- Salmonellosis
- Miliary tuberculosis
- Double malarial infections (>1 species)
- Gonococcal and meningococcal endocarditis
Malaria fever - Paroxysmal patterns
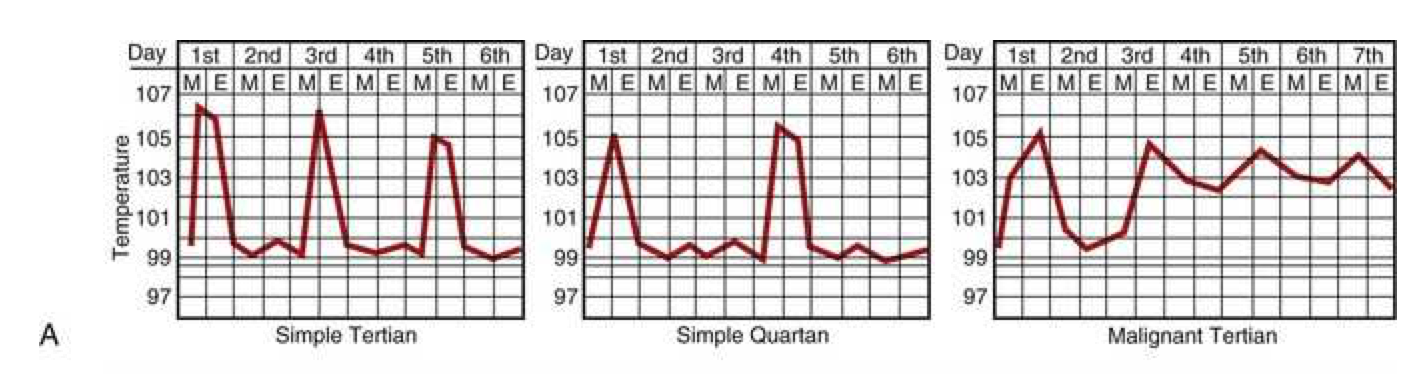
Febrile paroxysms may occur every other day for P. vivax, P. ovale, and P. falciparum (tertian fever) and every third day for P. malariae (quartan fever).
Paroxysms occurring at regular intervals are more common in P. vivax or P. ovale than P. falciparum. With improvements in early diagnosis and treatment, this traditional description of cyclic fever is seen infrequently.
Saddle-back (biphasic) fever
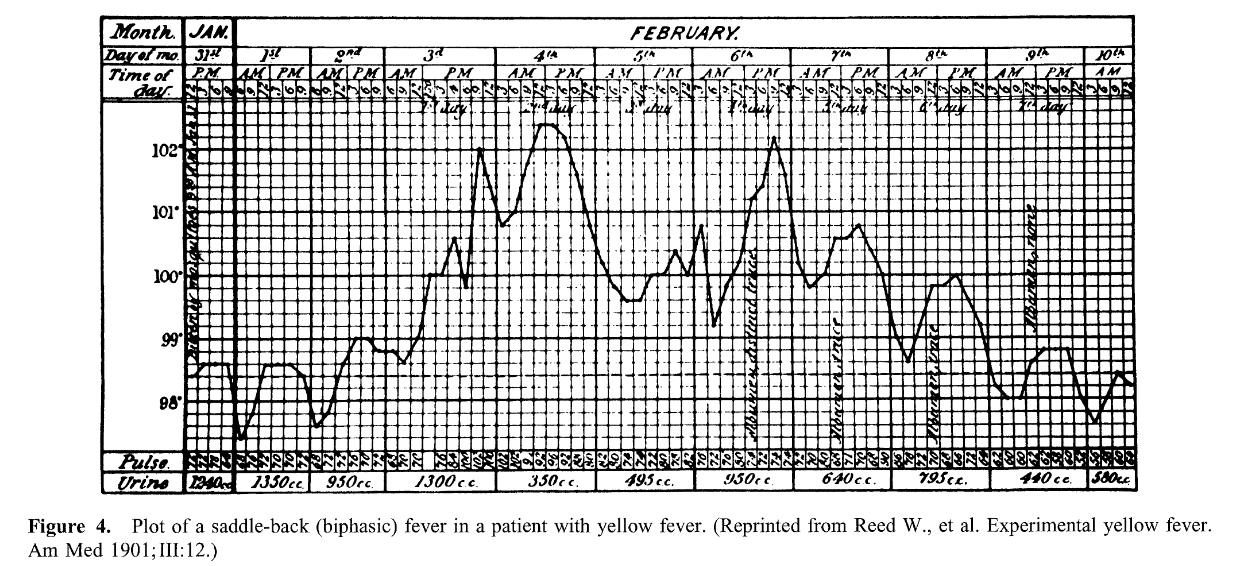
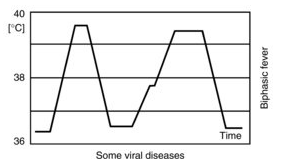
- Several days of fever, distinct reduction in fever for ~1 day, then several days of higher fever
- Dengue and yellow fever
- Colorado tick fever
- Rift valley fever
- Influenza and other viral infections
Intermittent hectic (Charcot’s) fever
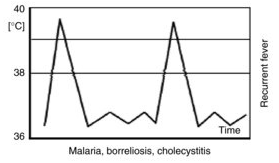
- Sporadic episodes of fever with periods of normal temperature and recurrence
- Frequently seen in cholangitis associated with cholelithiasis
- Classic teaching: jaundice, fever, right upper quadrant pain (Charcot’s triad)
- Often associated with leukocytosis and toxic appearance
Undulating (Pel-Ebstein) fever
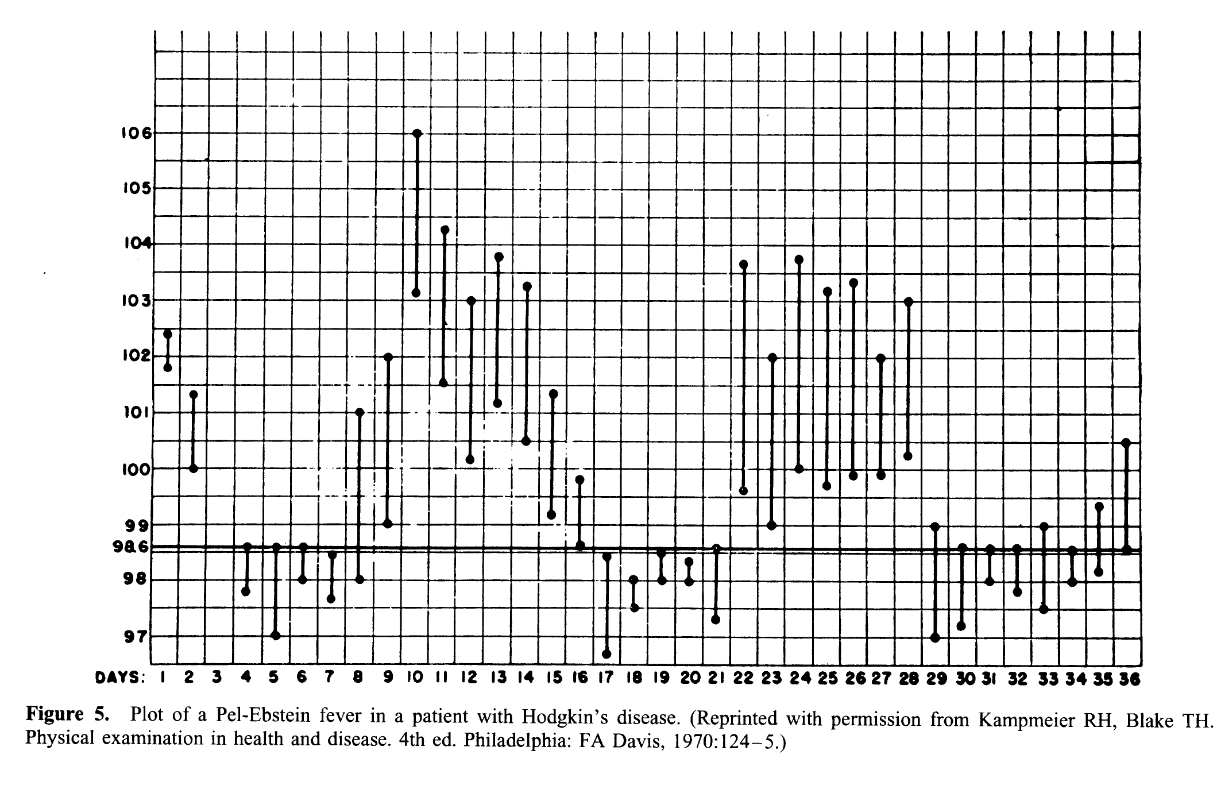
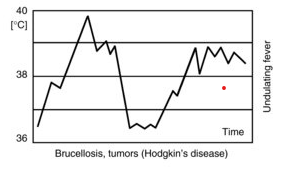
- Weekly or longer periods of fever and equally long afebrile periods, with repetition of the cycle
- Hodgkin’s disease (classic association)
- Brucellosis due to Brucella melitensis
- Occasionally tuberculosis
Typus Inversus
- Reversal of diurnal pattern with highest temperatures in early morning hours rather than late afternoon/evening
- Miliary TB
- Salmonelloses
- Hepatic abscess
- Bacterial endocarditis
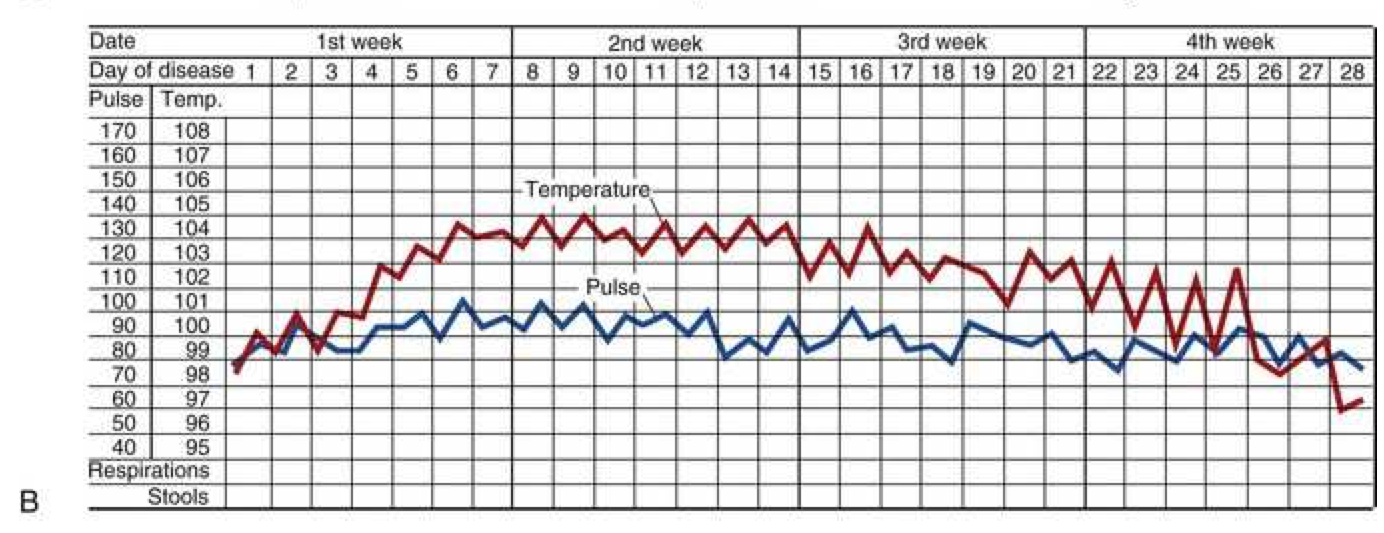
Typhoid fever - Step-ladder fever
Jarisch-Herxheimer reaction
Definition: Sharply increased elevation of temperature with rigors, chills, and constitutional symptoms occurring within hours of starting antibiotic therapy
Mechanism: Lysis of spirochetes (or other organisms) releases endotoxin triggering acute inflammatory response
Organisms associated:
- Primary or secondary syphilis
- Leptospirosis
- Tick-borne relapsing fever (Borrelia)
- Tetracycline or chloramphenicol therapy for acute brucellosis
Clinical significance: Can be severe enough to cause hemodynamic compromise; does not indicate treatment failure

Bone marrow biopsy
- Diagnostic yield: ~25% in two case series; especially valuable for:
- Granulomatous infections (TB, histoplasmosis, sarcoidosis)
- Hematologic malignancies (leukemia, lymphoma)
- Patients with abnormal CBC (anemia, thrombocytopenia, leukopenia)
- Organisms identified:
- Mycobacterium tuberculosis
- Fungi (Histoplasma, Cryptococcus, Coccidioides)
- Intracellular bacteria (Brucella, Bartonella)
- Consider: When fever pattern and presentation suggest granulomatous disease or hematologic malignancy

Imaging studies
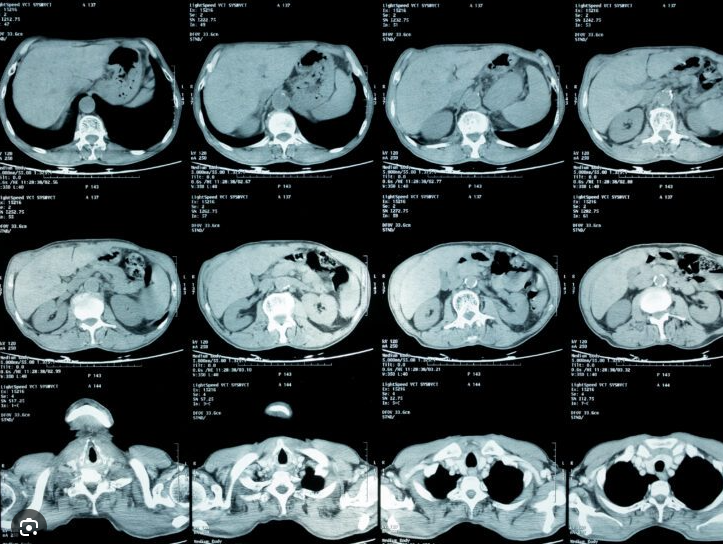
Generally low diagnostic yield without localizing symptoms
CT of abdomen and chest
Ultrasound of gallbladder and hepatobiliary systems
CT pulmonary angiogram (for pulmonary embolis)
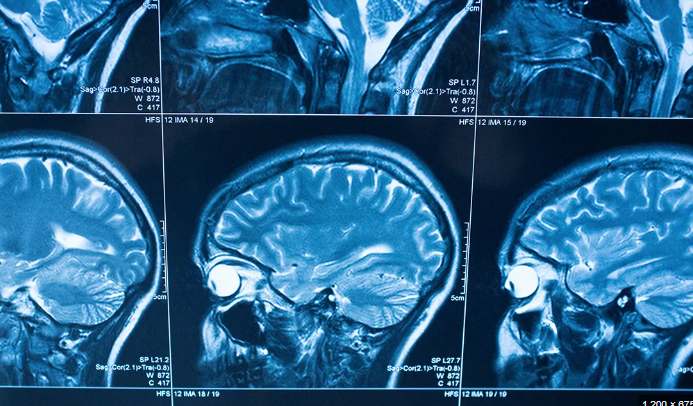
MRI for CNS, spleen, lymph nodes, aorta (vasculitis)
Indium 111-tagged white blood cell scan (becoming less common)
Gallium-67 scan (largely replaced by PET-CT)
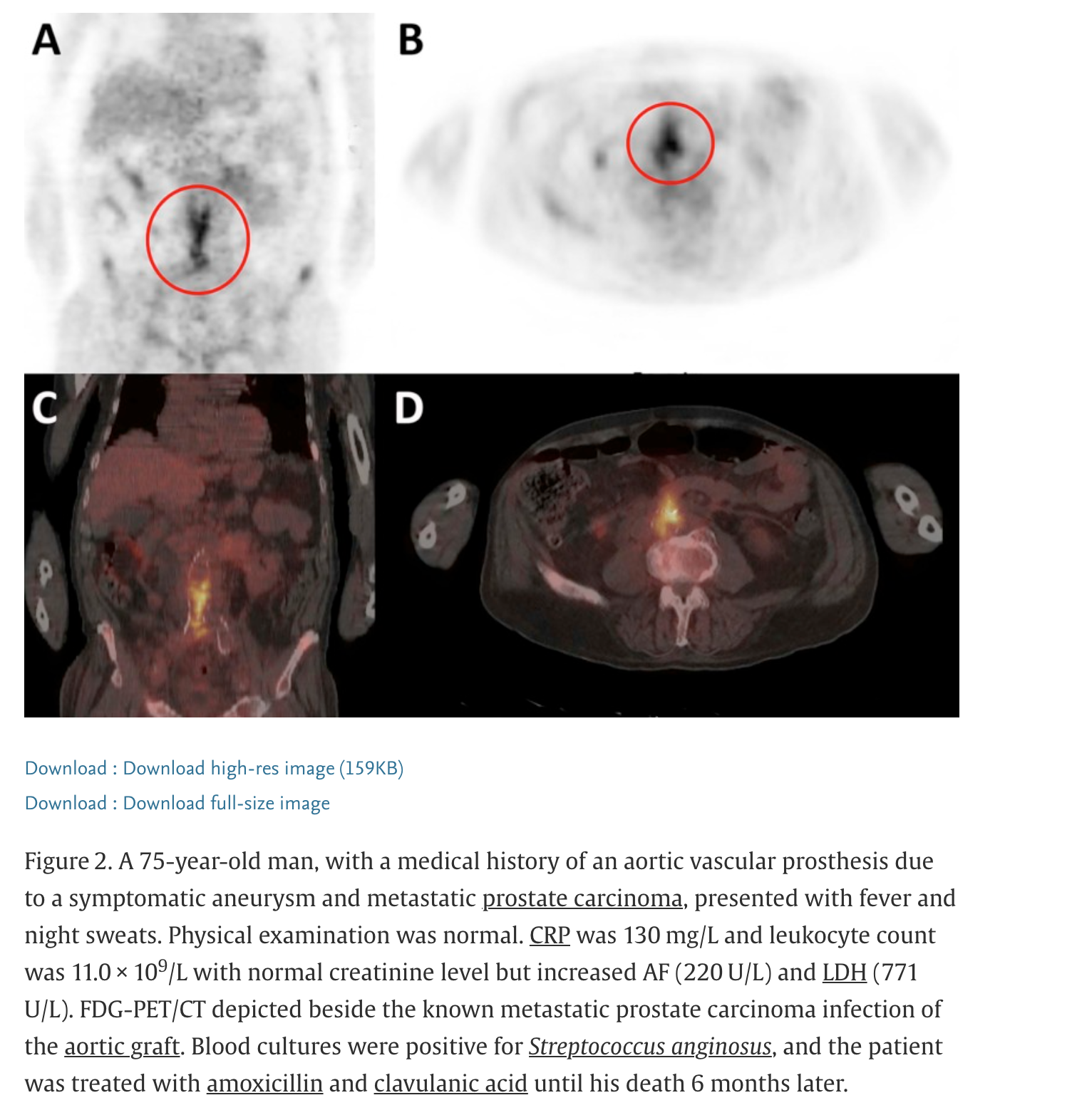
PET-CT: Superior sensitivity for inflammatory and malignant processes
¹⁸F-fluorodeoxyglucose (FDG) positron emission tomography