Daptomycin and streptogramins
2026-06-08
Daptomycin and Streptogramins
Russell E. Lewis, Pharm.D., FCCP
Associate Professor of Infectious Diseases

russelledward.lewis@unipd.it
Slides and course materials: www.idpadovaid.com
Learning Objectives
After this lecture, you should be able to:
- Describe the mechanism of action of daptomycin
- Understand daptomycin’s spectrum of activity and susceptibility testing
- Explain mechanisms of daptomycin resistance
- Apply appropriate dosing for different clinical scenarios
- Recognize adverse effects and monitoring requirements
- Identify clinical indications for daptomycin use
Part 1: Daptomycin basics
What is daptomycin?
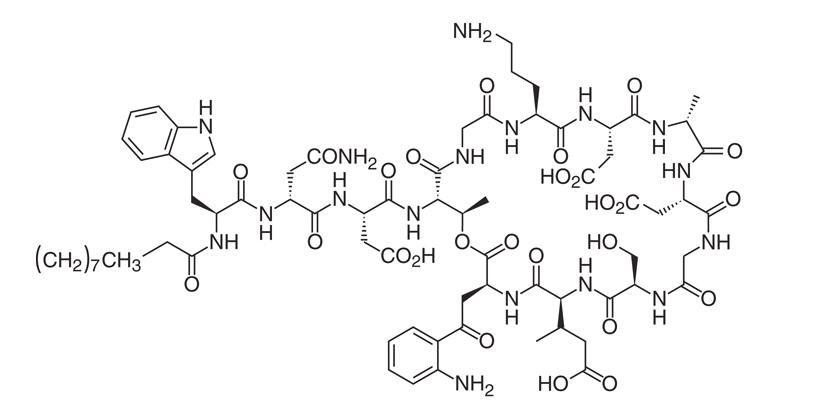
- Cyclic lipopeptide antibiotic (1620.67 Da)
- Produced by Streptomyces roseosporus
- Discovered in the 1980s- Eli Lilly
- FDA approved: 2003 (US), 2006 (Europe)
Chemical structure
Mechanism of action
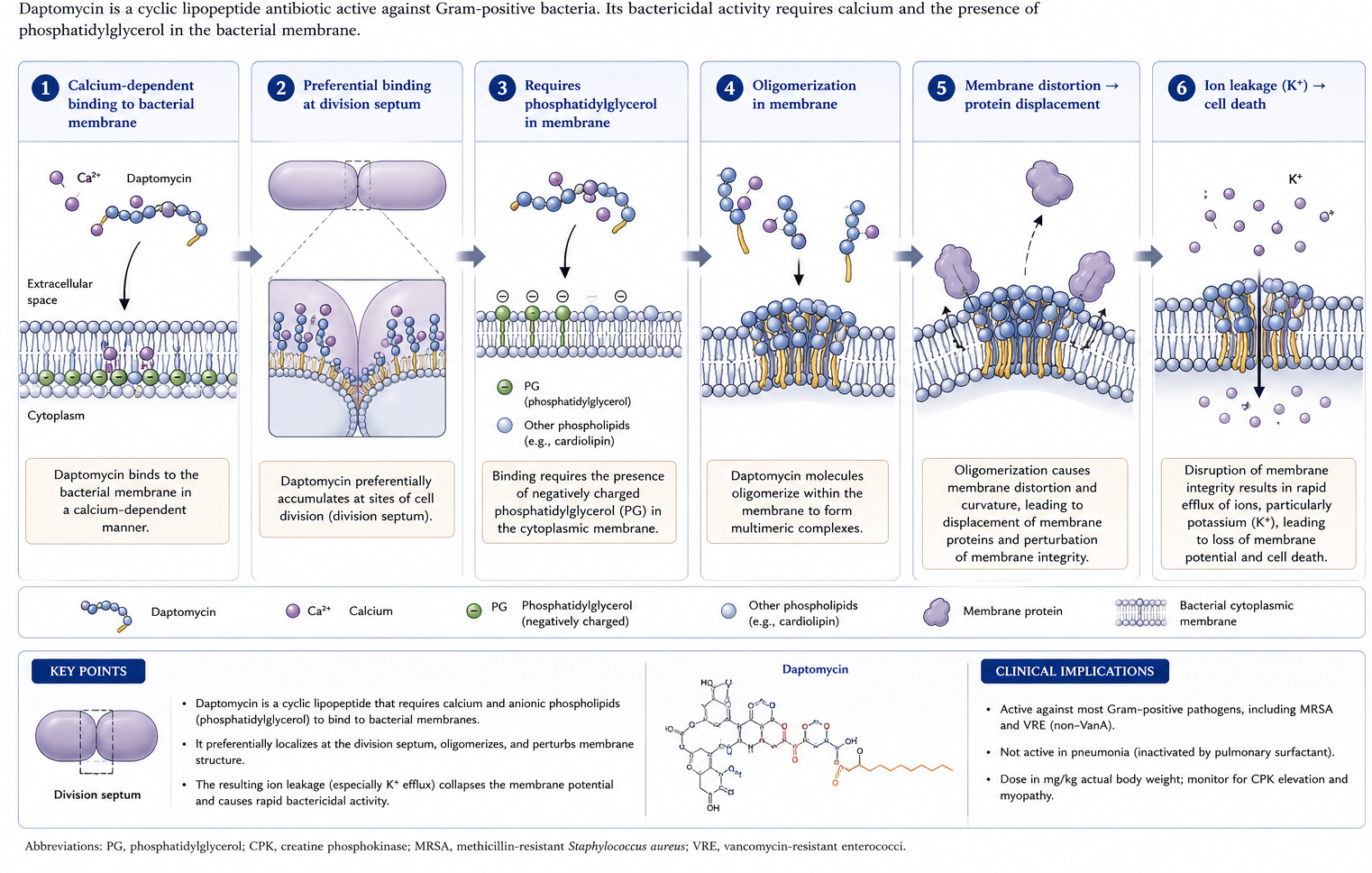
Key feature: Bactericidal without lysis
- Kills bacteria without significant cell lysis
- Results in reduced inflammatory response
- Less release of proinflammatory mediators
- Potential advantage in severe infections
Part 2: Antimicrobial spectrum
Spectrum of activity
Active against:
- Staphylococcus aureus (MSSA, MRSA, VISA)
- Coagulase-negative staphylococci
- Enterococcus faecalis and E. faecium (including VRE)
- Streptococci
- Some gram-positive anaerobes
Organisms with variable/No activity
Variable activity:
- Actinomyces spp. (MIC90 4-32 μg/mL)
- Lactobacillus spp.
- Some clostridial species
No activity:
- Gram-negative organisms
- Pulmonary infections (surfactant inactivation!)
Susceptibility testing challenges
Warning
Calcium-supplemented Mueller-Hinton broth is REQUIRED (50 μg/mL calcium concentration)
- Disk diffusion: NOT recommended
- Etest: Variable reproducibility
- Broth microdilution: Preferred method
- Significant interlaboratory variability exists
Susceptibility breakpoints
| Organism | Susceptible | Intermediate | Resistant |
|---|---|---|---|
| Staphylococci | ≤1 μg/mL | - | >1 μg/mL |
| Streptococci | ≤1 μg/mL | - | >1 μg/mL |
| E. faecalis (FDA) | ≤4 μg/mL | - | - |
| E. faecium (CLSI 2019) | - | 2-4 μg/mL (SDD) | ≥8 μg/mL |
Part 3: Resistance Mechanisms
Resistance is uncommon but…
- In vitro- resistance after serial passage is uncommon
- However “clinical resistance” emerges during therapy
- 6% of patients in pivotal bacteremia trial developed elevated MICs
- Risk factors:
- Deep-seated/undrained infections
- Prior vancomycin exposure
- Inadequate dosing
Phenotypic changes in resistant strains
- Enhanced membrane fluidity
- Increased positive surface charge
- Resistance to depolarization
- Reduced phosphatidylglycerol content
- Increased pigment production
- Decreased daptomycin binding
Genetic basis (S. aureus)
Key genes implicated:
- mprF - LPG synthase/flippase → increased surface charge
- yycFG/walKR - Cell envelope homeostasis
- vraSR - Cell wall stress response
- dlt operon - D-alanylation of teichoic acids
- pgsA/cls - Phospholipid metabolism
The “Seesaw effect”
Clinical Pearl
Daptomycin resistance often leads to increased β-lactam susceptibility
- Basis for daptomycin + β-lactam combinations
- Demonstrated in vitro and in animal models
- Multiple β-lactams effective (oxacillin, ceftaroline, etc.)
- May prevent emergence of resistance
Enterococcal resistance
- LiaFSR system is central to resistance
- Homologue of VraTSR in staphylococci
- Cell envelope stress response system
- Additional mutations in gdpD, cls genes
- Resistance can emerge WITHOUT prior exposure
Part 4: Pharmacokinetics
Key PK parameters
| Parameter | Value |
|---|---|
| Half-life | 7.3-9.6 hours |
| Protein binding | 90-93% |
| Volume of distribution | 92-117 mL/kg |
| Elimination | Renal (unchanged) |
Peak concentrations by dose
| Dose (mg/kg) | Peak (μg/mL) | AUC (μg·hr/mL) |
|---|---|---|
| 4 | ~55 | ~500 |
| 6 | ~86 | ~750 |
| 8 | ~116 | ~850 |
| 10 | ~130 | - |
| 12 | ~165 | - |
Tissue penetration
Good penetration:
- Skin/soft tissue (~68% of plasma)
- Cardiac vegetations (~50% of serum)
Poor penetration:
- CNS (~2-6%)
- Bone (variable)
- Lungs (inactivated by surfactant!)
Part 5: Dosing
FDA-EMA approved dosing
| Indication | Dose | Route |
|---|---|---|
| ABSSSI | 4 mg/kg q24h | IV |
| Bacteremia/Right-sided endocarditis | 6 mg/kg q24h | IV |
BUT…
Experts recommend 8-12 mg/kg/day for serious infections!
Renal dose adjustment
| CrCl | Dose Adjustment |
|---|---|
| ≥30 mL/min | No adjustment |
| <30 mL/min | Every 48 hours |
| Hemodialysis | After HD, q48h |
| CRRT | Variable - consider TDM |
Special populations
- Obesity: No dose adjustment (use actual body weight)
- Hepatic impairment: No adjustment (Child-Pugh B)
- Pediatrics: FDA-approved, age-based dosing
- Pregnancy: Category B (insufficient human data)
Part 6: Adverse effects
Muscle toxicity (Primary concern)
- CPK elevation (dose and duration dependent)
- Mechanism: Direct membrane toxicity to myofibers
- Risk factors:
- Cmin ≥24.3 mg/L
- Concurrent statin use
- Renal impairment
- Duration >7 days
CPK monitoring & management
When to Stop Daptomycin
- CPK >1000 units/L WITH symptoms
- CPK >2000 units/L (10× ULN) even without symptoms
Monitor:
- Baseline CPK before starting
- Weekly CPK (more often in renal impairment)
- Weekly in patients on statins
Other adverse effects
| Effect | Frequency | Notes |
|---|---|---|
| Eosinophilic pneumonia | Rare | After ~10 days; stop drug |
| Peripheral neuropathy | 9% vs 2% | Usually mild, reversible |
| GI symptoms | Common | Similar to comparators |
| Renal/hepatic | Rare | May be protective vs aminoglycosides |
Drug interactions
Minimal CYP450 interactions (not metabolized hepatically)
Monitor closely with:
- Statins - increased CPK risk
- PT/INR assays - may cause false elevation
Part 7: Clinical applications
FDA/EMA-approved indications
- ABSSSI (Acute Bacterial Skin & Skin Structure Infections)
- S. aureus (MSSA, MRSA)
- Streptococcus pyogenes
- E. faecalis (vancomycin-susceptible)
- S. aureus bacteremia & right-sided endocarditis
Off-label uses
- VRE infections (bacteremia, endocarditis)
- Left-sided endocarditis (with other agents)
- Osteomyelitis
- Prosthetic joint infections
- CNS infections (limited data)
When to consider daptomycin
- MRSA with vancomycin MIC ≥1.5-2 μg/mL
- Vancomycin failure or intolerance
- VRE infections
- Concern for nephrotoxicity
- Desire for once-daily dosing
When NOT to use daptomycin
Important
NEVER use for pneumonia!
Also avoid:
- Known daptomycin-resistant organism
- Prior daptomycin failure
- Active rhabdomyolysis
- Untreated source of infection
Part 8: Combination therapy strategies
Rationale for Combinations
- Prevent emergence of resistance
- Exploit the seesaw effect
- Enhance bactericidal activity
- Treat complicated/deep-seated infections
Daptomycin + β-lactam
Best supported combination:
- Oxacillin/nafcillin
- Ceftaroline (excellent data)
- Ceftriaxone, cefotaxime
- Ertapenem
- Even ampicillin-sulbactam
Other combinations
| Partner | Evidence | Comment |
|---|---|---|
| Gentamicin | In vitro synergy | Nephrotoxicity concern |
| Rifampin | Variable | May be antagonistic |
| Fosfomycin | Emerging data | Limited availability |
| Trimethoprim-sulfamethoxazole | Case reports | For MRSA |
Case example: Persistent MRSA bacteremia
Scenario: Day 7 of vancomycin, blood cultures still positive
Approach:
Switch to high-dose daptomycin (8-10 mg/kg)
Add β-lactam (ceftaroline or oxacillin)
Ensure source control 4. Monitor CPK closely
Part 9: Quinupristin-Dalfopristin
(Brief overview)
Quinupristin-dalfopristin basics
- Streptogramin B (30%) + Streptogramin A (70%)
- Trade name: Synercid
- Target: 50S ribosomal subunit
- Limited clinical use due to:
- Central line requirement
- Arthralgias/myalgias
- Infusion site reactions
- Limited availability
Quinupristin-dalfopristin spectrum & dosing
Active against:
- Most gram-positives EXCEPT E. faecalis
- Some gram-negatives (H. influenzae, M. catarrhalis)
Dosing: 7.5 mg/kg IV q12h (1-hour infusion)
No renal adjustment needed
Quinupristin-dalfopristin: Why it’s rarely used
- Arthralgias/myalgias (up to 50%)
- Severe infusion site reactions
- Requires central venous access
- CYP3A4 drug interactions
- Limited availability -Italian marketing authorization revoked
- Better alternatives exist (linezolid, daptomycin)
Summary & Key Takeaways
Daptomycin key points
- Calcium-dependent cyclic lipopeptide
- Bactericidal without cell lysis
- Spectrum similar to vancomycin but active against VISA/VRE
- Never use for pneumonia (surfactant inactivation)
- Monitor CPK - stop if elevated with symptoms
- Use high doses (8-12 mg/kg) for serious infections
Clinical pearls
Tip
- Consider daptomycin when vancomycin MIC ≥1.5-2 μg/mL
- Add β-lactam for persistent bacteremia
- The “seesaw effect” makes β-lactam combinations logical
- Renal dosing: extend interval, don’t reduce dose
- Check CPK baseline and weekly; more often with renal impairment or statins
Questions to consider
- Why can’t daptomycin be used for pneumonia?
- What is the seesaw effect and how is it clinically useful?
- When should you suspect daptomycin resistance?
- What CPK level should prompt discontinuation?
- Why is high-dose daptomycin preferred for serious infections?